Fungi of clinical and medical significance:
In this clinical and medical mycology section, you will learn about:
- Basic Lab Safety in the Mycology Lab
- Types of fungi and which ones are medically significant
- The structure of fungi, including budding yeast cells, pseudohyphae, true hyphae, mycelium, vegetative and aerial hyphae, reproductive structures of yeasts and molds
- Samples to collect for analysis for identification of potential infections and how to handle them safely
- Culture media, tests, and technology for identifying yeasts and molds
- Clinically significant yeasts, how to culture, identify, and treat them
- Clinically significant molds, including:
- The Zygomycetes
- The Cutaneous Molds
- The Dermatophytes and Superficial Molds
- The Subcutaneous Molds
- The Mold-Like Bacteria Actinomycetes
- The Dimorphic Molds
- The Opportunistic Molds
- The Dematiaceous Molds
- The Organisms that Can Cause Systemic Infection
- Antifungal therapy agents for mycoses
mushroom mycology:
This website focuses on medical and clinical microbiology and mycology, and infectious yeasts and molds. If you are interested in learning more about environmental mycology and mushroom structure and identification, please visit my biology website (jensbiology) at https://www.jensbiology.weebly.com and select the Kingdom Fungi tab.
https://www.jensbiology.weebly.com
sAFETY PRECAUTIONS IN THE MYCOLOGY LAB:
Many fungi produce conidia or spores that can easily become airborne, which could potentially contaminate the entire mycology lab area and cause accidental infection. For this reason, you need to follow airborne transmission precautions when working in the mycology laboratory. Airborne precautions are essential to prevent contamination of the lab and infection of laboratory techs.
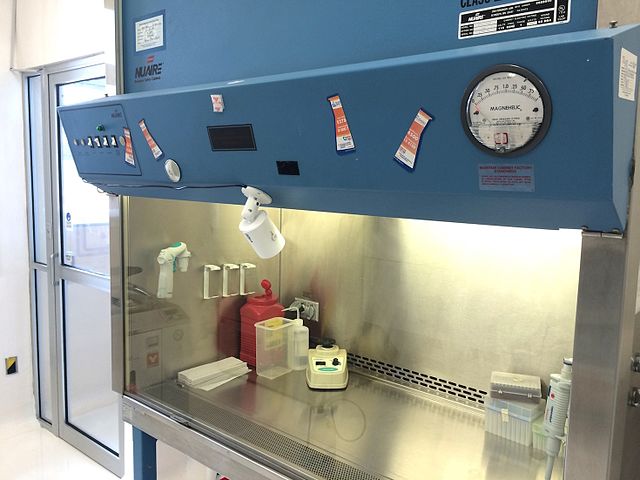
Always work under a calibrated and fully functional biological safety cabinet or hood in a negative pressure room. Proper PPE needs to be worn, including an N95 mask, a disposable lab apron, and gloves. Eye protection is not needed if you are working behind the glass of the biologial safety cabinet.
The work area should be disinfected at least daily and if there are any spills. After handling mycology cultures, laboratory personnel should remove their gloves and wash their hands thoroughly with soap and water for 20 seconds, and dry them with a paper towel. Any contaminated materials need to be bagged properly in biohazard bags and autoclaved before they are removed from the room to be discarded.
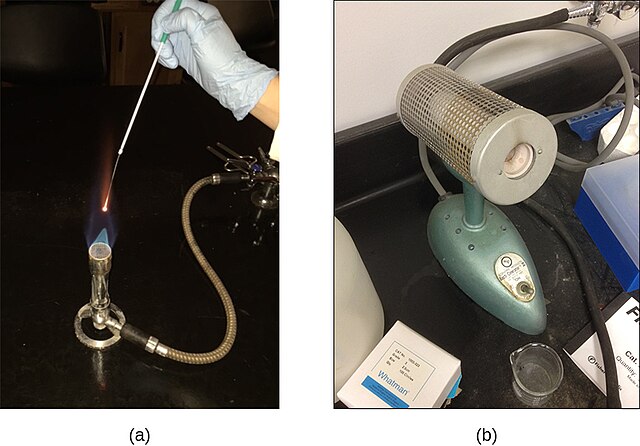
When working under the biological safety cabinet, any stainless steel loops, inoculating needles, spatulas, should all be incinerated for sterlization carefully, avoiding any aerosolization or spattering of infectious material.
Sterile slants of tubed media are preferred to agar plates when possible. All plates should be shrink-sealed prior to removal from the biological safety cabinet and incubation. Wet preps should be prepared under the biological safety cabinet of all molds before setting up any slide cultures because the systemic organisms should never be set up on slide cultures. Cultures should never be sniffed to determine odors due to the fact that there may be spores on the plate that could potentially be inhaled.
Under the biological safety cabinet, a container should be made fresh each day with disinfectant, to decant any supernatant into. Another container with disinfectant should remain under the hood to soak any disposable loops in prior to discarding them, and to soak any tools in prior to autoclaving them.
You should never eat, drink, chew gum, smoke, or apply cosmetics or lip balm or touch your eyes in the mycology laboratory.
Always work under a calibrated and fully functional biological safety cabinet or hood in a negative pressure room. Proper PPE needs to be worn, including an N95 mask, a disposable lab apron, and gloves. Eye protection is not needed if you are working behind the glass of the biologial safety cabinet.
The work area should be disinfected at least daily and if there are any spills. After handling mycology cultures, laboratory personnel should remove their gloves and wash their hands thoroughly with soap and water for 20 seconds, and dry them with a paper towel. Any contaminated materials need to be bagged properly in biohazard bags and autoclaved before they are removed from the room to be discarded.
When working under the biological safety cabinet, any stainless steel loops, inoculating needles, spatulas, should all be incinerated for sterlization carefully, avoiding any aerosolization or spattering of infectious material.
Sterile slants of tubed media are preferred to agar plates when possible. All plates should be shrink-sealed prior to removal from the biological safety cabinet and incubation. Wet preps should be prepared under the biological safety cabinet of all molds before setting up any slide cultures because the systemic organisms should never be set up on slide cultures. Cultures should never be sniffed to determine odors due to the fact that there may be spores on the plate that could potentially be inhaled.
Under the biological safety cabinet, a container should be made fresh each day with disinfectant, to decant any supernatant into. Another container with disinfectant should remain under the hood to soak any disposable loops in prior to discarding them, and to soak any tools in prior to autoclaving them.
You should never eat, drink, chew gum, smoke, or apply cosmetics or lip balm or touch your eyes in the mycology laboratory.
https://upload.wikimedia.org/wikipedia/commons/thumb/6/61/Biological_Safety_Cabinet_%28Class_II%2C_Type_A2%29_Front_view.jpg/640px-Biological_Safety_Cabinet_%28Class_II%2C_Type_A2%29_Front_view.jpg

https://upload.wikimedia.org/wikipedia/commons/thumb/7/7c/Superciste_prostory.jpg/640px-Superciste_prostory.jpg
https://upload.wikimedia.org/wikipedia/commons/thumb/2/22/Medical_laboratory%2C_Where_science%2C_medicine_converge_140417-F-FM358-007.jpg/640px-Medical_laboratory%2C_Where_science%2C_medicine_converge_140417-F-FM358-007.jpg
tools in the mycology lab:
Common tools you will work with in the mycology lab include:
- Basic inoculating tools: inoculating needles, loops, spreaders, teasing needles
- Sterile swabs
- Incinerator
- Autoclave
- Biohazard bins
- Containers with disinfectant
- Shrink seal
- Parafilm
- Incubators (35 degrees Celsius, 37 degrees Celsius, 42 degrees Celsius)
- Refrigerator with reagents
- Clear Scotch Tape
- Scissors
- Glass Slides
- Alcohol wipes to clean slides
- Coverslips
- Vaseline (for hanging suspensions)
- Clear nail polish (to make slides permanent)
- Pipettes
- Blood culture bottles for yeast and incubator (Bactec, BacT Alert, other...)
- Spectrophotometer for McFarland standard (if using Vitek yeast cards or susceptibility testing, Microscan, or Phoenix)
- Vortex
- Microscopes
- Specific culture media (studied in another section below), such as SABHI, BHI with blood, Mycosel, SAB slants, etc...
- MALDI-TOF mass spectrophotometer for yeast identification
- Stains:
- Lactophenol Cotton Blue
- KOH
- India Ink
- Sterile Saline
- Calcofluor White

https://upload.wikimedia.org/wikipedia/commons/thumb/9/9f/Basic_inoculating_tools.jpg/640px-Basic_inoculating_tools.jpg

https://upload.wikimedia.org/wikipedia/commons/thumb/7/76/Inoculating_loop_and_wire_used_in_Microbiology_Laboratory.jpg/640px-Inoculating_loop_and_wire_used_in_Microbiology_Laboratory.jpg
https://upload.wikimedia.org/wikipedia/commons/thumb/7/72/OSC_Microbio_13_02_LoopFlame.jpg/640px-OSC_Microbio_13_02_LoopFlame.jpg
maldi-tof mass spectrophotometry:
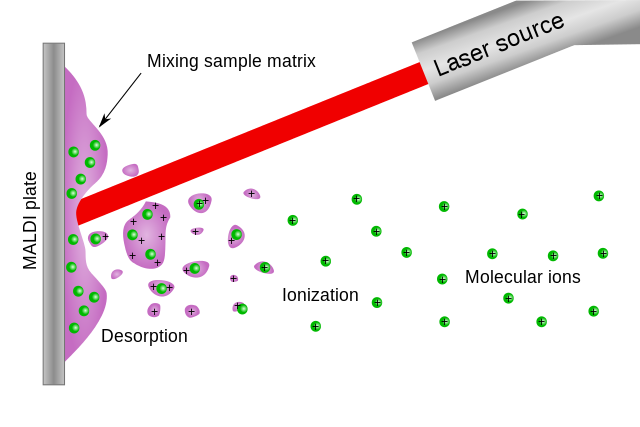
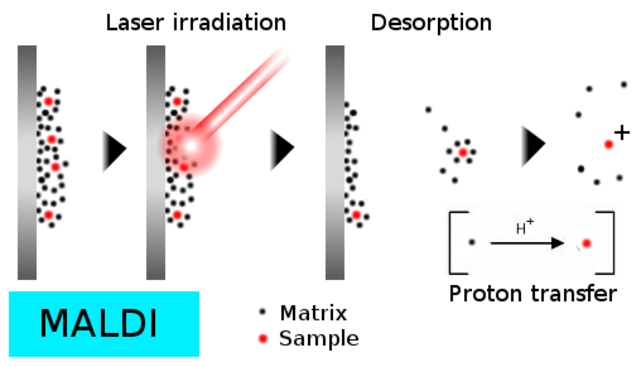
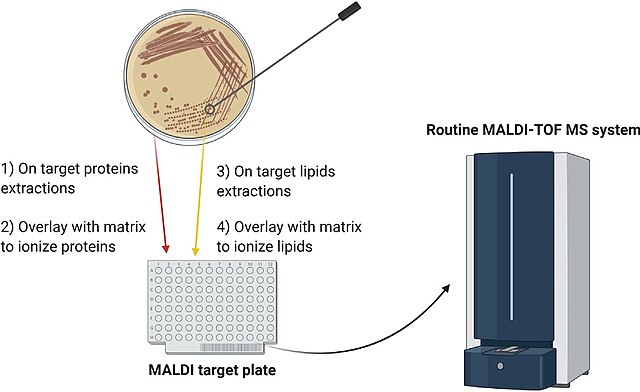
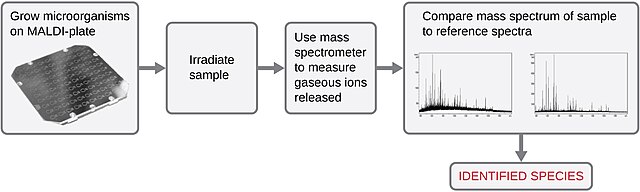
The mass spectrophotometer is an automated system used for microbial identification. It uses Matrix-Assisted Laser Desorption Ionization (MALDI) Time-of-Flight (TOF) technology and contains a database that is comprehensive for bacteria, fungi, mycobacteria, actinomycetes, and even molds. It provides clear, accurate identification for the genus, species, and family levels. It is very beneficial to clinicians, because it is quick, and they can begin appropriate treatmet contributing to excellent patient care and outcomes.
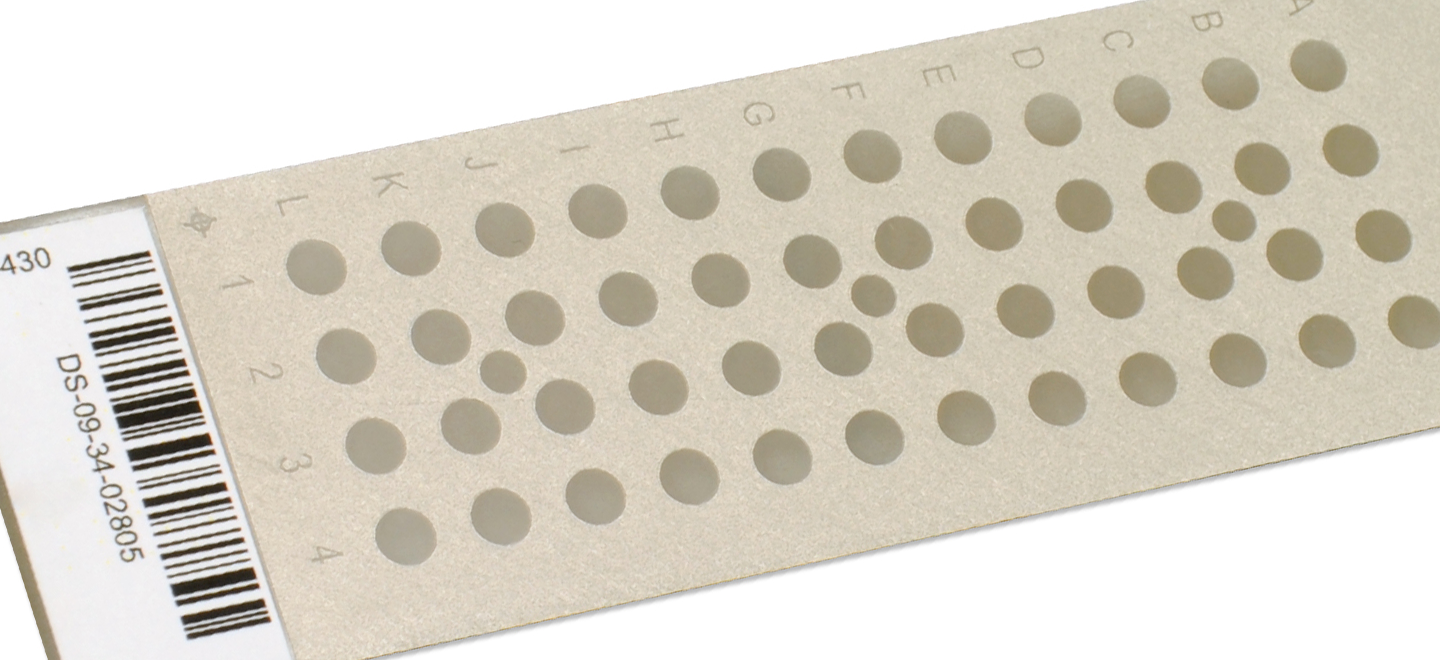
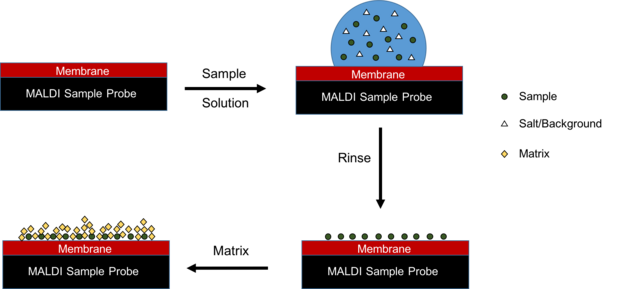
A stainless steel sample plate with small wells is used to inoculate with sample culture using a pipette tip or a special "pick-me-pen" that touches the colonies. Each section is called an "acquisition", and the central circle is smaller. There are typically 3 acquisition areas on a rectangular slide. Each acquisition area has its own calibration spot. A sample of calibrator, E. coli, is added to that circle. The slides are barcoded and scanned to match with the LMS. You can assign each well to the sample. Operation verification, fine-tuning, and alignment are all automatic.
The slides are prepared in a "prep station" that is used to scan the ID and barcodes so you can associate them with each other. The software keeps track of which wells have been prepared by the user, whether this is yeast or bacteria. You can choose whether you are putting yeast or bacteria on the slides. This is SO important: Make sure you ALWAYS wear gloves when handling the slides and NEVER touch them with your bare hands. If you touch the slides with your bare hands, the oils and any makeup, food, contamination, will cause a smear on the slide that the laser can burn. It will ruin both the slide AND the laser. ALWAYS put on a FRESH pair of gloves when you are about to hand the slide. I always like to put the slide on a KIM wipe as well, then carefully transport it to the MALDI-TOF to ensure that it is as clean as possible.
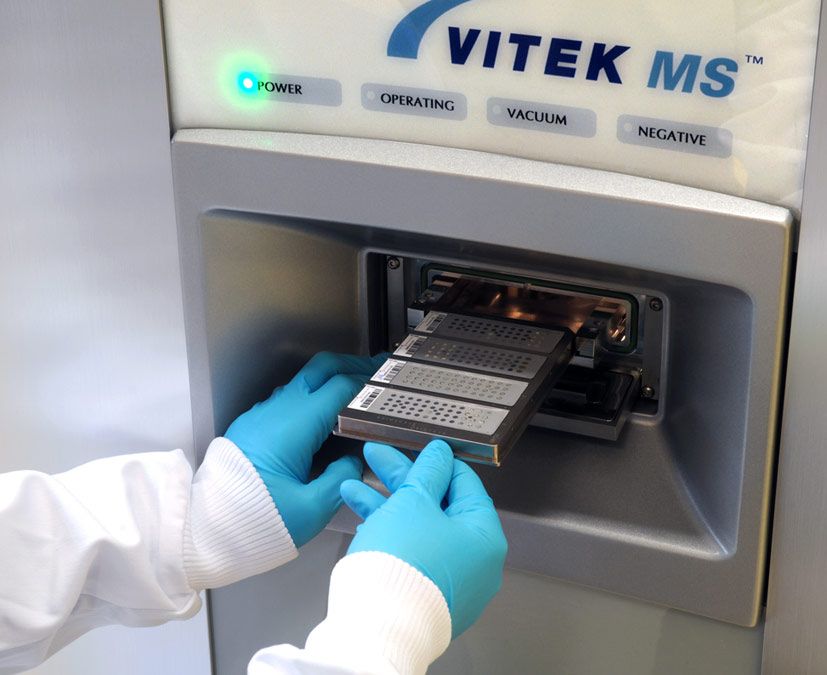
Once the smears dry, matrix is added. For yeasts, there are two. The first to be added is 0.5 microliters of formic acid. It must completely air dry before adding the second matrix. It can take a long time to dry, so plan accordingly. Once dry, add 1.00 microliters of CHCA and allow it to air dry. This one dries much faster. The slide must correctly be placed in the designated slide holder in the MALDI-TOF. The MALDI-TOF must be checked each day, and QC needs to be performed each morning prior to using the machine. Absorbant beads in the back of the machine must be changed out when they are yellow or orange. Weekly and monthly maintenance should be performed to keep the machine running smoothly and efficiently.
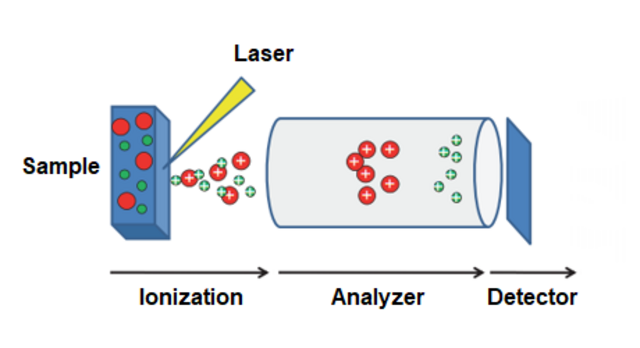
The MALDI-TOF warms up by creating a vacuum of negatively-charged elecrons. This creates an electrostatic field. There are electrodes inside that interact with charged particles. A precise laser source, often 337 nm nitrogen, is heated up, where it targets the sample on the stainless steel plate interacting with the matrix. The 50 Hz/second pulses cause the matrix and sample to break down off the plate (desorption), become a cloud of charged particles (ionization), that accelerate and speed up and become molecular ions (protons +, electrons -, and neutrons: neutral).
The ions pass through a ring electrode and go through a vacuum tube which is extremely hot inside, and this is why the analyzer is so "tall". In fact, the linear flight tube is about 1.2 meters drift length. The amount of time it takes for travel, based on molecular size and charge, in this chamber is known as "Time-of-Flight" (TOF) in the field free region, or flight tube where the vacuum exists. The vacuum is maintained by 2 turbomolecular pumps with rotary backing. Beam blanking deflects unwanted high intensity signals.
The TOF is plotted based on the measurement of the particle size and charge (proteins) that hit a molecular mirror called a "detector plate," which recognizes the ionized molecular particles. This is shown as intensity peaks on the linked database computer system (middleware), which match up to the computer database, and develop an identification score.
Some hospitals use MYLA, but others use different systems. MYLA allows the information to cross over into the the LMS computer system, and allow the user to verify the ID before "accepting" it, in case something needs to be rerun. If the circles are "green", the ID is good. If the circles are "yellow", then it likely found 2-3 organisms that are very close in ID and allows the user to pick one. If the circles are "red", the ID was unsuccessful and needs to be rerun. There is a special icon that allows you to choose when to send the ID to the chart, at which time it will show up for healthcare personnel so they can see it in the LMS.
The proteins in the analyzer are broken down into amino acid monomers, then codons, and finally DNA or mRNA, which are matched, which is why this technology is so precise, sensitive and accurate. The Advanced Spectra Classifier ensures accurate results.
See the gallery below for images of the MALDI-TOF and prep:
A stainless steel sample plate with small wells is used to inoculate with sample culture using a pipette tip or a special "pick-me-pen" that touches the colonies. Each section is called an "acquisition", and the central circle is smaller. There are typically 3 acquisition areas on a rectangular slide. Each acquisition area has its own calibration spot. A sample of calibrator, E. coli, is added to that circle. The slides are barcoded and scanned to match with the LMS. You can assign each well to the sample. Operation verification, fine-tuning, and alignment are all automatic.
The slides are prepared in a "prep station" that is used to scan the ID and barcodes so you can associate them with each other. The software keeps track of which wells have been prepared by the user, whether this is yeast or bacteria. You can choose whether you are putting yeast or bacteria on the slides. This is SO important: Make sure you ALWAYS wear gloves when handling the slides and NEVER touch them with your bare hands. If you touch the slides with your bare hands, the oils and any makeup, food, contamination, will cause a smear on the slide that the laser can burn. It will ruin both the slide AND the laser. ALWAYS put on a FRESH pair of gloves when you are about to hand the slide. I always like to put the slide on a KIM wipe as well, then carefully transport it to the MALDI-TOF to ensure that it is as clean as possible.
Once the smears dry, matrix is added. For yeasts, there are two. The first to be added is 0.5 microliters of formic acid. It must completely air dry before adding the second matrix. It can take a long time to dry, so plan accordingly. Once dry, add 1.00 microliters of CHCA and allow it to air dry. This one dries much faster. The slide must correctly be placed in the designated slide holder in the MALDI-TOF. The MALDI-TOF must be checked each day, and QC needs to be performed each morning prior to using the machine. Absorbant beads in the back of the machine must be changed out when they are yellow or orange. Weekly and monthly maintenance should be performed to keep the machine running smoothly and efficiently.
The MALDI-TOF warms up by creating a vacuum of negatively-charged elecrons. This creates an electrostatic field. There are electrodes inside that interact with charged particles. A precise laser source, often 337 nm nitrogen, is heated up, where it targets the sample on the stainless steel plate interacting with the matrix. The 50 Hz/second pulses cause the matrix and sample to break down off the plate (desorption), become a cloud of charged particles (ionization), that accelerate and speed up and become molecular ions (protons +, electrons -, and neutrons: neutral).
The ions pass through a ring electrode and go through a vacuum tube which is extremely hot inside, and this is why the analyzer is so "tall". In fact, the linear flight tube is about 1.2 meters drift length. The amount of time it takes for travel, based on molecular size and charge, in this chamber is known as "Time-of-Flight" (TOF) in the field free region, or flight tube where the vacuum exists. The vacuum is maintained by 2 turbomolecular pumps with rotary backing. Beam blanking deflects unwanted high intensity signals.
The TOF is plotted based on the measurement of the particle size and charge (proteins) that hit a molecular mirror called a "detector plate," which recognizes the ionized molecular particles. This is shown as intensity peaks on the linked database computer system (middleware), which match up to the computer database, and develop an identification score.
Some hospitals use MYLA, but others use different systems. MYLA allows the information to cross over into the the LMS computer system, and allow the user to verify the ID before "accepting" it, in case something needs to be rerun. If the circles are "green", the ID is good. If the circles are "yellow", then it likely found 2-3 organisms that are very close in ID and allows the user to pick one. If the circles are "red", the ID was unsuccessful and needs to be rerun. There is a special icon that allows you to choose when to send the ID to the chart, at which time it will show up for healthcare personnel so they can see it in the LMS.
The proteins in the analyzer are broken down into amino acid monomers, then codons, and finally DNA or mRNA, which are matched, which is why this technology is so precise, sensitive and accurate. The Advanced Spectra Classifier ensures accurate results.
See the gallery below for images of the MALDI-TOF and prep:
https://upload.wikimedia.org/wikipedia/commons/thumb/a/a9/Maldi.svg/640px-Maldi.svg.png
|
https://upload.wikimedia.org/wikipedia/commons/thumb/6/61/MALDI.png/640px-MALDI.png
|
https://upload.wikimedia.org/wikipedia/commons/thumb/d/dd/MALDI-TOF_process.jpg/640px-MALDI-TOF_process.jpg
https://external-content.duckduckgo.com/iu/?u=https%3A%2F%2Fwww.biomerieux-industry.com%2Fsites%2Fdefault%2Ffiles%2Fstyles%2Fimage_large_1440_x_660_%2Fpublic%2F2019-06%2FVITEK%2520MS%2520PERFORM.png%3Fitok%3D5FAvKRzY&f=1&nofb=1&ipt=cc3bcb12a301d4d259ee574a741fa1f12e9384734175dd27f06a58ea3da59b81&ipo=images
|
https://external-content.duckduckgo.com/iu/?u=https%3A%2F%2Fi.pinimg.com%2Foriginals%2F74%2F6e%2F0a%2F746e0a03c9425aba3086dc0c4db9115d.jpg&f=1&nofb=1&ipt=86a89d5f9f86fb0d98c336f87ebdedc9036554ea4718372883bd057a559d7442&ipo=images
|
https://upload.wikimedia.org/wikipedia/commons/thumb/2/28/MALDI_TOF_EN.png/640px-MALDI_TOF_EN.png
https://upload.wikimedia.org/wikipedia/commons/thumb/7/7f/MALDI-_Sample_Preparation.png/640px-MALDI-_Sample_Preparation.png
https://upload.wikimedia.org/wikipedia/commons/thumb/5/5e/OSC_Microbio_07_05_maldi.jpg/640px-OSC_Microbio_07_05_maldi.jpg
OVERVIEW OF FUNGI AND MYCOLOGY:
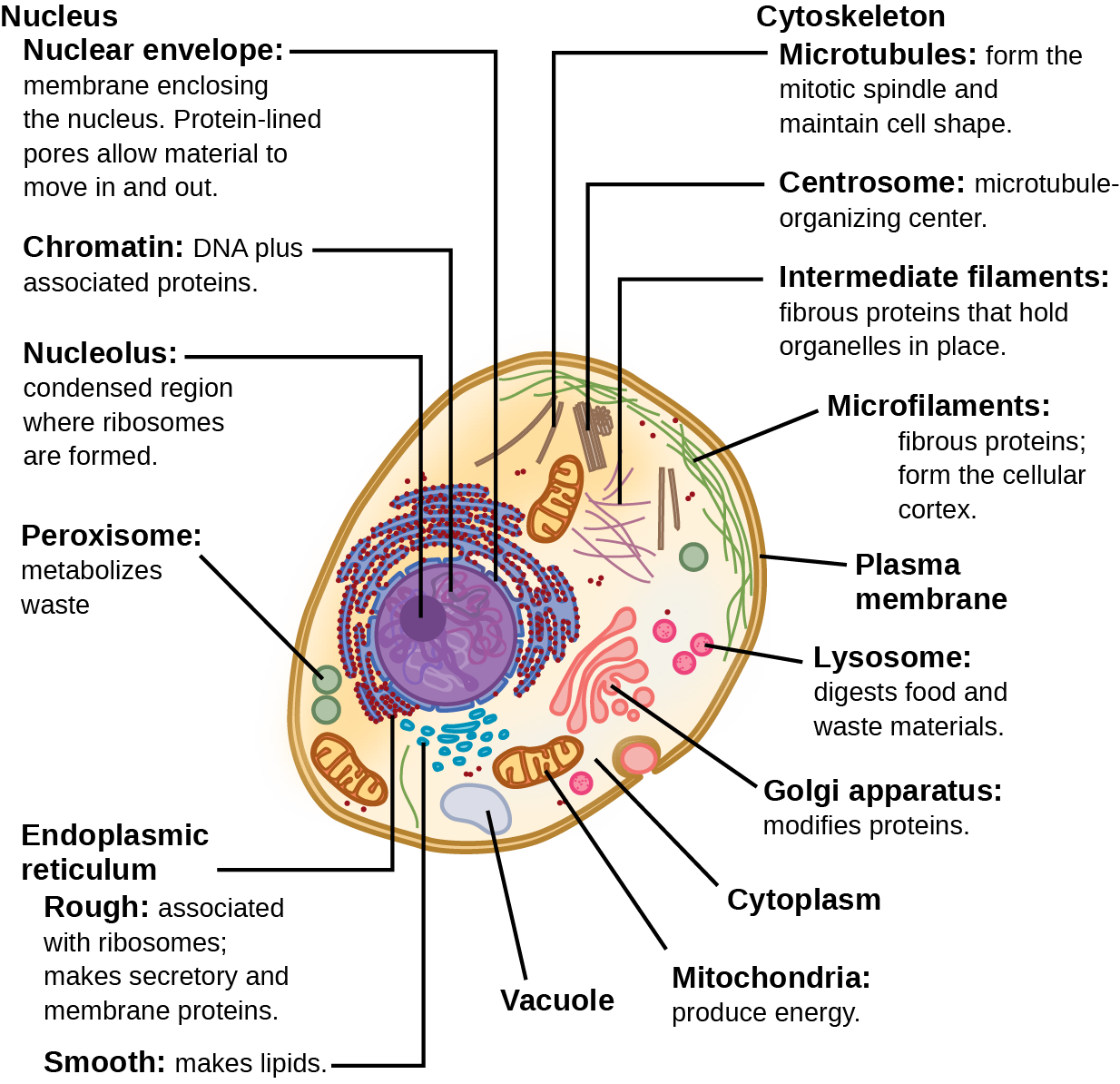
Fungi are categorized as eukaryotic cells. This means that they have a true nucleus and membrane-bound organelles. They require an aerobic environment, because they need oxygen to grow, and most are ubiquitous, or found just about everywhere in the environment. Many types of fungi exist, and many normally cause no harm (are nonpathogenic) unless the conditions are just right for infection. Many of the fungal infections are caused by opportunistic fungi, meaning that they only cause infection if the conditions are just right. Fungi include both yeasts AND molds. Medical mycology is the area of microbiology that studies and identifies fungi, including those that are pathogenic to humans and are possible causes of disease.
Fungi include the following:
Fungi are categorized as eukaryotic cells. This means that they have a true nucleus and membrane-bound organelles. They require an aerobic environment, because they need oxygen to grow, and most are ubiquitous, or found just about everywhere in the environment. Many types of fungi exist, and many normally cause no harm (are nonpathogenic) unless the conditions are just right for infection. Many of the fungal infections are caused by opportunistic fungi, meaning that they only cause infection if the conditions are just right. Fungi include both yeasts AND molds. Medical mycology is the area of microbiology that studies and identifies fungi, including those that are pathogenic to humans and are possible causes of disease.
Fungi include the following:
- Yeasts:
- Unicellular eukaryotes
- Elliptical/oval/egg-shaped or round spheres
- Reproduce by budding, which can be observed microscopically on a wet mount
- Buds can form long chains of yeast cells known as pseudohyphae, which can also be observed microscopically on a wet mount or KOH wet mount
- Growth is slower than that of bacteria
- Typically "creamy", "pearly", "matte", or "lacy" growth on agar dishes
- Best recovery is on SAB Dextrose Agar (SDA) or Cornmeal Agar, which can then be successfully identified on the MALDI-TOF mass spectrophotometer
- Molds:
- Hyphae
- Filaments that are hair-like or thread-like, branching, cylindrical tubules made up of fungal cells from end-to-end
- Grow and extend from the tubule tips
- Tend to be dry and fuzzy
- Can be observed microscopically via KOH wet mount, LPCB Scotch Tape Method , Sandwich Method, Slide Method or Tease Mount
- Mycelium
- Branching, intertwined hyphae
- Extend and growth in length, producing spores
- Spores
- Reproduction bodies of molds
- Dimorphic fungi:
- Can grow either as a yeast or as a mold, depending on temperature and environment
- Saprophytes:
- Live in and break down organic matter such as soil, leaves, old, dead, decaying vegetation
- Hyphae
- Mushrooms
- Gills
- Pores
- "Teeth"
https://external-content.duckduckgo.com/iu/?u=https%3A%2F%2Fs3-us-west-2.amazonaws.com%2Fcourses-images%2Fwp-content%2Fuploads%2Fsites%2F3206%2F2018%2F05%2F03174549%2FFigure_04_03_01a.png&f=1&nofb=1&ipt=8516f4d4cfe1c3cf527fbe06a4b6edbb638dd04e1c60f9e81903910df9d0347b&ipo=images
sample collection and techniques used in mycology:
The Five "A's" of Obtaining and Processing a Sample:
The ability to accurately identify a fungus begins with an adequate sample. There are several good things to keep in mind when collecting a good sample or when educating healthcare personnel about obtaining one for the lab.
Sample Sources to Collect From:
The ability to accurately identify a fungus begins with an adequate sample. There are several good things to keep in mind when collecting a good sample or when educating healthcare personnel about obtaining one for the lab.
- First, the sample should be collected from the area of the body that is most likely to be infected, and it should be a good sample.
- For a sputum sample, make sure that you instruct the patient to take a deep breath and produce a deep cough. Sometimes an induced sputum can be obtained by helping a cough with mist first. Saliva, or spit, is not a good sample.
- Second, the sample needs to be adequate, or "enough", to perform cultures and tests needed to isolate fungi.
- Third, always use sterile aseptic technique when collecting the sample, wearing proper PPE and performing good hand hygiene before donning and after doffing your gown and gloves and mask.
- Fourth, please make sure that you deliver the sample to the laboratory promptly, within two hours, so the sample can be set up as soon as possible or be properly preserved until it can be processed. Why is this important?
- Many fungi are slow-growing. The quicker the sample gets processed, the sooner it can be identified so the patient can be administered the most effective medication for their condition.
- Fungi can be overgrown by the rapid-growing bacteria and opportunists.
- Last, but not least, accessioning is important! The sample must be properly labeled with at least two patient identifiers, along with the date and time of collection, collector's initials, source, and any other site-specific information required by your facility, and scanned in or accepted and associated with your lab.
Sample Sources to Collect From:
- Blood
- The most common fungal pathogen isolated from blood cultures is the yeast Candida spp.
- Commercial blood culture systems like Bactec and BacT Alert are found in the microbiology lab. They incubate the blood culture bottles, rock them gently, and have special sensors that monitor carbon dioxide production every ten minutes. Both aerobic and anaerobic blood culture bottles are used to support the growth of yeasts and bacteria, and both oxygen-needing and oxygen-hating microbes. Bactec has a fungal medium that actually enhances the recovery of yeasts.
- The blood sample can be drawn into a Vacutainer tube with 0.35% polyantholsulfonate (SPS) (yellow-top) and then transferred using transfer devices into blood culture media in the laboratory. It can also be drawn directly into the blood culture media at the bedside, however, blood culture bottles are not sterile and once the plastic tops are removed, the tops of the bottles must be carefully cleansed with either an iodine-alcohol solution, or an iodine solution follwed by an alcohol (isopropyl) solution, in addition to cleaning the patient's arm prior to collection.
- Blood cultures are held for 3-4 weeks if a slow-growing fungal organism is suspected, depending upon your facility.
- Bone Marrow
- Bone marrow biopsies and cultures are the ideal sample for identifying Histoplasma capsulatum. Bone marrow is normally a sterile site, so no microbes should be in it. Any microbes seen in bone marrow are significant.
- Cerebrospinal Fluid (CSF)
- CSF is collected aseptically and the sample is cytocentrifuged. The supernatant should be poured off, and the button of sediment should be vortexed and one drop of sediment should be placed on the slide with a coverslip and microscopically examined for fungal elements with the condenser turned down and under low light.
- Another slide should be made with one drop of sediment, one drop of India Ink, and a coverslip, and examined for the presence of encapsulated yeast indicative of Cryptococcus neoformans.
- A third slide should be made with one drop of sediment, air-dried, and Gram-stained to look for any yeasts and/or bacteria and any white blood cells present.
- Enough sediment should be saved to inoculate aerobic fungal media and anaerobic fungal media (if Actinomyces is suspected), and to perform a cryptococcal antigen rapid test, PCR (such as the Biofire MEPAN to look for meningitis), and any other pertinent fungal tests your facility performs.
- Cutaneous Samples (Hair, Nails, Skin):
- If a hair fungus is suspected, the suspicious hair should be plucked out of the scalp by the roots with sterile forceps or sterile tweezers.
- If a hair fungus is suspected, UV lamp or Wood's Lamp can be used to see if the hair fluoresces. Hairs that fluoresce should be chosen for testing, since some fungi that cause scalp and hair infections fluoresce in UV light. Look for broken hairs, scaling, or peeling, and send them to the lab in a sterile cup or sterile Petri dish.
- If a nail fungus is suspected, the nails should first be scrubbed and cleaned with 70% isopropyl alcohol. A sterile blade should be used to scrape away the outer layers of nail, and to concentrate on the inner layers of nail that appear infected. Send them in a sterile cup or sterile Petri dish.
- If a skin fungus is suspected, the skin should be thoroughly cleaned first and scrubbed with 70% isopropyl alcohol to reduce the level of normal microflora on the skin. If a dermatophyte is suspected, the outer portions of the red ring should be scraped off with a sterile blade and sent to the lab in a sterile cup or sterile Petri dish.
- Once in the lab, a hair, nail or skin scraping should be cut into tiny pieces and mixed with KOH potassium hydroxide. Cover with a coverslip and set it on top of a slide warmer for 10-20 minutes to accelerate the breakdown process of the protein keratin and to remove cellular debris. Keep enough sample to inoculate the fungal media for culture. Observe microscopically for any fungal elements, including:
- Budding yeast cells
- Pseudohyphae
- Hyphae
- Mycelium
- NOTE: If the yeast Malassezia furfur is suspected, add a layer of sterile olive oil (autoclaved, but not in plastic) to a SABHI tube or plate, because this will enhance the growth of this organism.
- Respiratory Samples: We have a lot of normal microflora that resides in our lungs and throat, mouth, and nasal passages. The respiratory tract can accidentally become infected with inhaled organisms, including when swallowing wrong, getting "choked up", aspirating, or when a patient is on a mechanical ventilator, causing VAP (ventilator-associated pneumonia). They can seed to other parts of the body.
- Bronchial Washings: These samples are obtained in the OR. A tube is placed down the patient's throat while they are under general anesthesia, and some sterile saline is injected or squirted through the tube to "wash" the lungs and collect microbes in the lungs, which aspirates the material. The downside to this procedure is that sometimes normal throat flora is picked up, too.
- Sputum: Spit or saliva are not good samples, and will lead to the sample being rejected and a call for a recollect. A good sputum sample should:
- always be collected first thing in the morning, right when the patient wakes up
- always be collected before they eat or drink anything since overnight incubation in the lungs will have allowed multiplication of microbes in the lungs, including any fungi present
- always be collected after the patient brushes their teeth and rinses with water and mouthwash
- always be collected after the patient takes a deep breath and produces a deep gutteral cough
- be placed in a sterile cup or sterile Petri dish and be sent to the laboratory immediately
- Throat Swabs: Throat samples are obtained on swabs. Two sterile swabs should be rolled over the affected area and follow these rules:
- be collected prior to eating
- be kept moist with 0.5 mL of sterile saline
- include material scraped off with a tongue depressor if thrush is suspected on the tongue or side of the cheeks
- Transtracheal Aspirates: This type of sample is obtained in the OR under general anesthesia. A slit is made surgically into the trachea, and a tube is inserted through it down to the bronchi and aspirating secretions of the lung. This procedure should:
- Be performed in the morning because lung secretions will build up overnight
- Pleural Fluid: Pleural fluid can be pulled out a number of ways, including through a syringe. This fluid is typically straw-colored and thick. Some laboratories will have you cytocentrifuge it to thin it out prior to making a slide for microscopic observation. The needle must be removed and the syringes must be capped prior to sending them to the lab for safety and sterility.
- Bronchioalveolar Lavage (BAL): This procedure is similar to a bronchial wash and is performed under general anesthesia in the OR.
- Bronchial Brushings: This procedure is the same as the bronchial wash, but a brush is also attached to scrape cells from the lung tissue. The entire brush is sent to the laboratory. Using sterile technique under the biological hood, the technologist should carefully cut the brush off of the long wire with sterile scissors, and place it in a sterile cup with sterile saline or broth and vortex it. The solution is then used to prepare plates for culture and to make slides for microscopic analysis.
- Fine Needle Aspirate (FNA): This procedure is used if acid-fast bacilli or Actinomyces is suspected. It is performed in the OR under general anesthesia.
- Respiratory samples are often analyzed for TB culture in addition to other respiratory tests, which is discussed in another section (See Mycobacteriology Tab)
- Tissue Biopsies: These samples are obtained by the patient's physician. They are often done under local or general anesthesia. These samples should include the center and edge of the lesion, including both normal and abnormal tissue. They should be kept moist with sterile saline until processing. Once in the lab, the technologist will use a tissue grinder kit to homogenize the tissues and tease them apart in a sterile Petri dish under the biological hood, examining them for any granules, pus, or areas of necrosis, and these should be the sections that are examined and cultured. Aerobic, anaerobic, and fungal culture media should be plated, and slides with KOH potassium hydroxide with a coverslip, along with a slide made for Gram stain, should be analyzed.
- Urine: During the wet mount or Gram stain, if yeast is seen, a SAB plate should be added to the culture. For urine cultures, if yeast is suspected, a SAB plate should be added. A clean-catch or catheterized urine sample should be collected after thorough cleansing of the genitalia prior to urinating to prevent the overgrowth of normal genital flora.
- Vaginal or Uterine Cervix: Yeasts commonly grow on the skin in these sites, but sometimes there is overgrowth of C. albicans, particularly if the individual has recently taken antibiotics, is pregnant, is immunocompromised or immunosuppressed, is taking certain other medications, and may have candidiasis, or a yeast infection. These samples are taken with two sterile swabs, which are placed into transport media (Stuart's or Amie's) and are refrigerated until processed. One swab is used to make a smear and is stained to look for fungal elements. The other swab is used to roll over fungal media. If gonorrhea is suspected or seen on the initial Gram stain, MTM media should be added. For the wet mount, add a drop of potassium KOH and a coverslip and look for any budding yeast cells, pseudohyphae or hyphae.
- Wounds (Lesions):
- Wounds: Aerobic swabs can be used to swab superficial wounds and place them in Amies medium or Stuart's medium. Anaerobic swabs should be placed into anaerobic transport medium and sent to the lab for anaerobic culture.
- Burns: The damaged tissue is necrotic and susceptible to infection. It can become colonized with yeasts and fungal opportunists.
- Deep ulcerations, such as pressure ulcers: Sometimes fungi are responsible for these so the scrapings of the crusted areas should be sent to the lab for analysis from the deep center and edge of active lesions scraped with a sterile scalpel
- Abscesses: Pus, or aspirated materials from needle and syringe can be sent from deep cysts or abscesses
- Granules: Observe any granules microscopically
- Wounds: Aerobic swabs can be used to swab superficial wounds and place them in Amies medium or Stuart's medium. Anaerobic swabs should be placed into anaerobic transport medium and sent to the lab for anaerobic culture.
Techniques:
direct exam:
An initial direct exam is always important, because you need to be able to quickly provide the patient's physician with a preliminary result, so they can proceed with a care plan and initial treatment. For this reason, it is critical that the sample be examined microscopically while you are preparing cultures.
A direct exam enables you to send out a preliminary result to the physician. It also gives you more information about the potential sample, in case you need to add or remove certain culture plates. The direct exam can be life saving, particularly since the physician can begin prophylactic treatment ahead of the long incubation period. Some fungi take 3-4 weeks to grow!
If you do not see a fungus on the initial wet mount, then it can potentially be ruled out, and the physician can avoid prescribing an unneccessary, costly antifungal drug, which may also have side effects, including toxicity, and require lengthy treatment.
A direct exam enables you to send out a preliminary result to the physician. It also gives you more information about the potential sample, in case you need to add or remove certain culture plates. The direct exam can be life saving, particularly since the physician can begin prophylactic treatment ahead of the long incubation period. Some fungi take 3-4 weeks to grow!
If you do not see a fungus on the initial wet mount, then it can potentially be ruled out, and the physician can avoid prescribing an unneccessary, costly antifungal drug, which may also have side effects, including toxicity, and require lengthy treatment.
saline wet mount and potassium koh wet mount/prep:
A saline wet mount can be performed by adding 1 drop of sample, 1 drop of saline, and a cover slip. If you are performing a vaginal wet mount or urine wet mount, use this method to identify and quantitate any epithelial cells, clue cells, white blood cells, red blood cells, yeast cells or other fungal elements, or the presence of Trichomonas vaginalis (dead or alive).
A drop of potassium KOH can also be added to clear proteins and cellular debris, particularly if you are observing a tissue, skin, hair or nail sample. KOH dissolves the keratin protein in these samples to make fungi more visible. It also kills Trichomonas vaginalis. It can be used to perform the "whiff" test because a slide with Trichomonas will have a rancid odor. The condenser should be turned down and the light should be low on the microscope since we are looking at transparent things.
Observe for fungal elements, including:
A drop of potassium KOH can also be added to clear proteins and cellular debris, particularly if you are observing a tissue, skin, hair or nail sample. KOH dissolves the keratin protein in these samples to make fungi more visible. It also kills Trichomonas vaginalis. It can be used to perform the "whiff" test because a slide with Trichomonas will have a rancid odor. The condenser should be turned down and the light should be low on the microscope since we are looking at transparent things.
Observe for fungal elements, including:
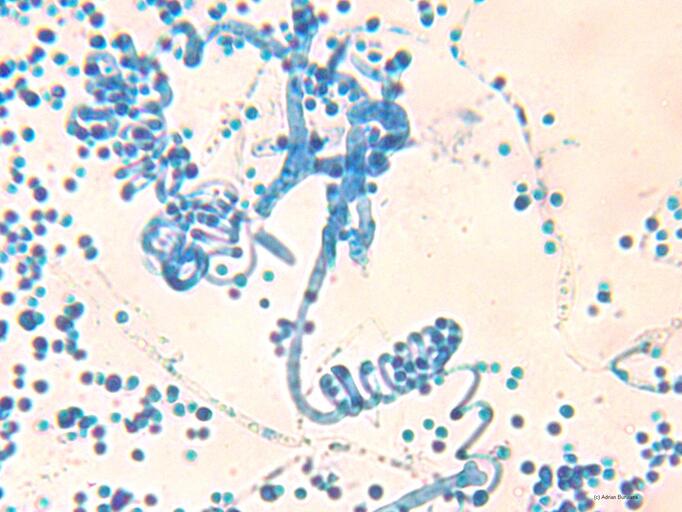
- Budding yeast cells (see the image below)
- Pseudohyphae (see the image below)
- Hyphae
- Conidia
- Thin, branching filaments
- Granules
- Spherules

https://upload.wikimedia.org/wikipedia/commons/thumb/a/ae/Yeasts_of_Cryptococcus_in_saline_wet_mount_Microscopy.jpg/640px-Yeasts_of_Cryptococcus_in_saline_wet_mount_Microscopy.jpg

https://upload.wikimedia.org/wikipedia/commons/thumb/c/c7/Fungal_hyphae_in_Urine_sample.jpg/640px-Fungal_hyphae_in_Urine_sample.jpg
https://upload.wikimedia.org/wikipedia/commons/thumb/b/b5/Fungal_hyphae_and_mycelium.jpg/640px-Fungal_hyphae_and_mycelium.jpg

https://upload.wikimedia.org/wikipedia/commons/thumb/c/c4/Thielaviopsis_basicola_chlamydospores_01.jpg/640px-Thielaviopsis_basicola_chlamydospores_01.jpg
lactophenol cotton blue wet mount (LPCB):
Lactophenol cotton blue stain is a great way to see and identify fungal structures, especially in molds. There are three parts to this stain that have specific roles:
You can make a LPCB slide permanent by rimming the coverslip with clear nail polish or Permamount solution. If using the method below, you can remove the tape first under the biological hood, and replace it with the coverslip on top, then rim the sides with the clear nail polish.
How to prepare a Scotch Tape Prep LPCB slide:
- Phenol: kills any organisms
- Lactic acid: preserves fungal structures so they stay intact
- Cotton blue: stains the chitin in fungal cell walls. Chitin is a polysaccharide (complex carbohydrate sugar) that makes fungi so strong, tough and durable and keeps it held together, intact and upright.
- Cotton blue is a known carcinogen, so always wear PPE, perform good hand hygiene after glove use, and handle slides under the biological hood and with care.
- Place a drop of sample on a clear glass slide and add one drop of LPCB stain.
- Mix well and add a coverslip.
- Observe microscopically with the condenser down and the light turned low for fungal elements.
- See image below of C. neoformans spherules.
You can make a LPCB slide permanent by rimming the coverslip with clear nail polish or Permamount solution. If using the method below, you can remove the tape first under the biological hood, and replace it with the coverslip on top, then rim the sides with the clear nail polish.
How to prepare a Scotch Tape Prep LPCB slide:
- Take a clear (not frosted) piece of Scotch tape and make a loop with it, sticky-side facing out.
- Place a drop of LPCB stain on a clean glass slide.
- Carefully touch the tips of the mold growing on the plate (under the biological hood) to capture the spores and hyphae.
- Gently place the tape sticky-side down across the slide in the LPCB stain. It will serve as a "coverslip".
- Place a long coverslip over the tape for extra protection.
- View microscopically under low light and turn the condenser down.
- See image below of Aspergillus spp conidiophores and conidia.
https://upload.wikimedia.org/wikipedia/commons/thumb/4/46/Cryptococcus_in_LPCB_mount_of_Culture.jpg/640px-Cryptococcus_in_LPCB_mount_of_Culture.jpg
https://upload.wikimedia.org/wikipedia/commons/thumb/7/70/Aspergillus.spp.jpg/640px-Aspergillus.spp.jpg
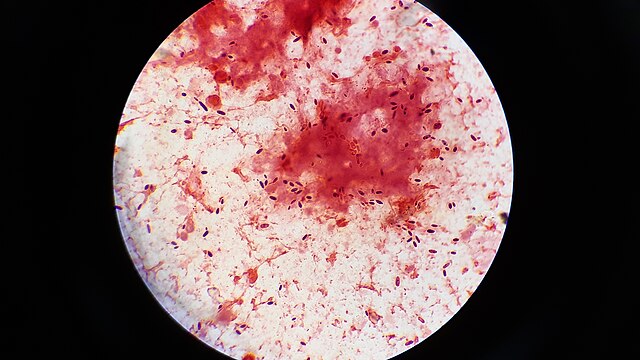
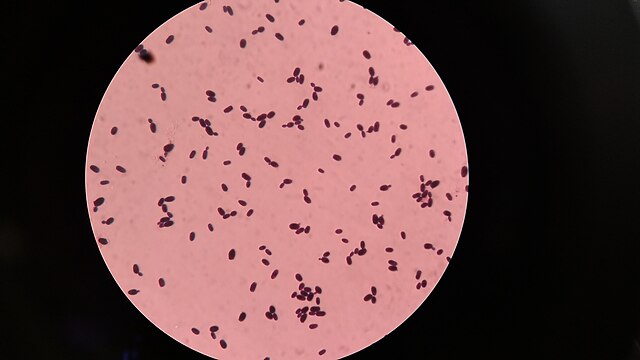
the gram stain:
Gram stains of fungi are particularly helpful. Oftentimes, the initial Gram stain will reveal fungi if they are present, which is part of the direct exam and can be released as a preliminary result. Fungi stain Gram-positive, or purple-blue. Budding yeast cells, as seen in the image below, as well as pseudohyphae, are the most common fungal elements seen in the Gram stain, but spherules, encapsulated yeast cells, and hyphae may also be seen. Yeast cells are about 2-3x larger than bacteria in size. If they are causing a true infection rather than simply colonization, they are almost always budding, and often form pseudohyphae. Hyphae are 2-3x wider in diameter than bacilli, and will appear granular, because they do not stain solid inside.
https://upload.wikimedia.org/wikipedia/commons/thumb/1/14/Yeast_cells_in_Gram_stained_smear_of_sputum.jpg/640px-Yeast_cells_in_Gram_stained_smear_of_sputum.jpg

https://upload.wikimedia.org/wikipedia/commons/thumb/d/db/Candida_albicans_-_Gram_stain.jpg/640px-Candida_albicans_-_Gram_stain.jpg
https://upload.wikimedia.org/wikipedia/commons/thumb/3/39/Yeast_cells_in_Gram_staining_of_Candida_growth_on_SDA.jpg/640px-Yeast_cells_in_Gram_staining_of_Candida_growth_on_SDA.jpg
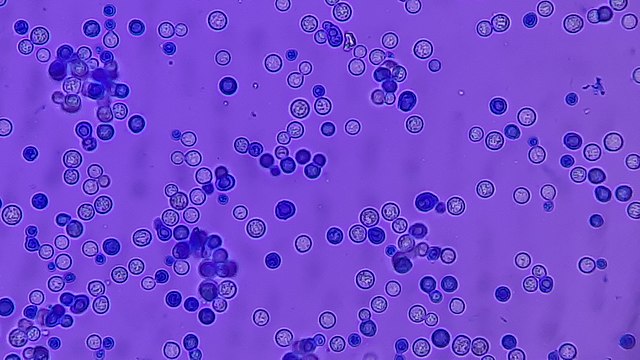
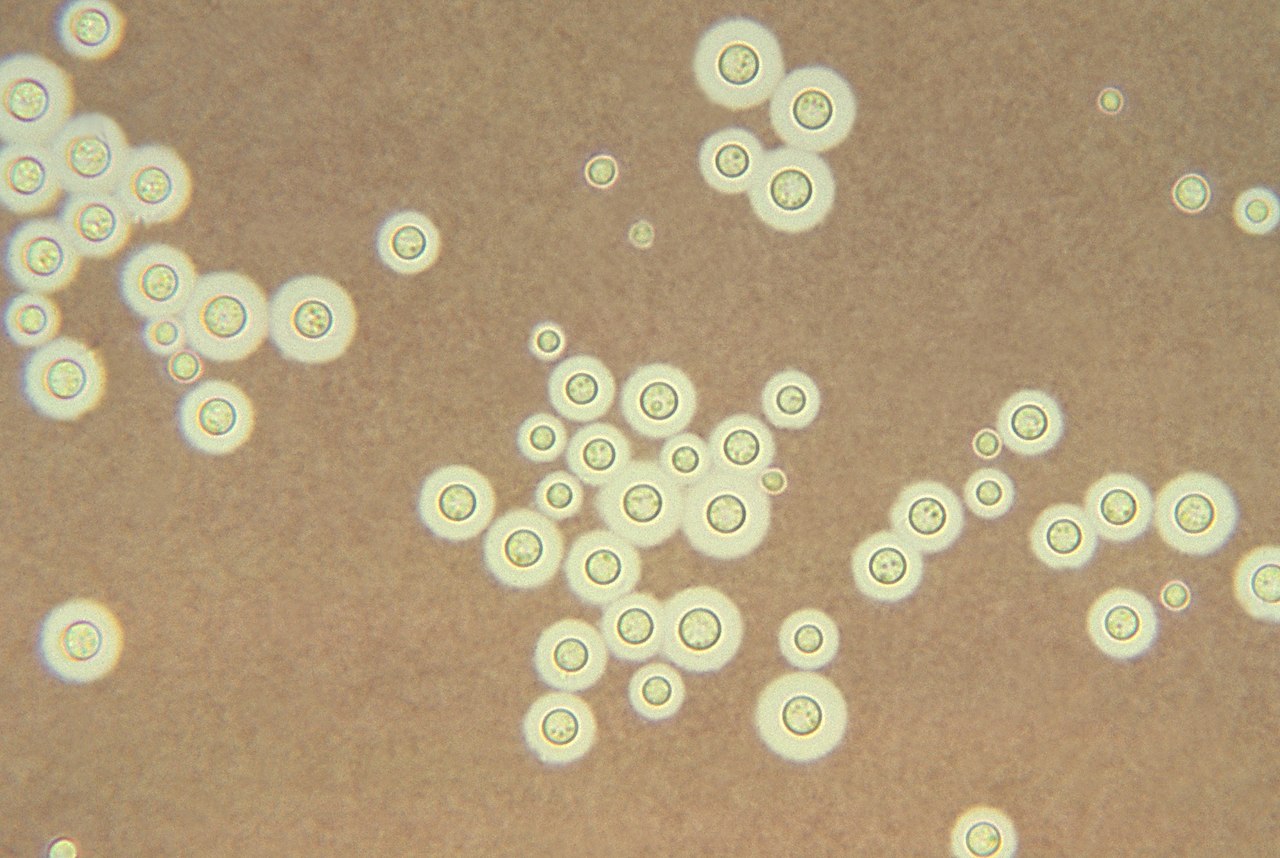
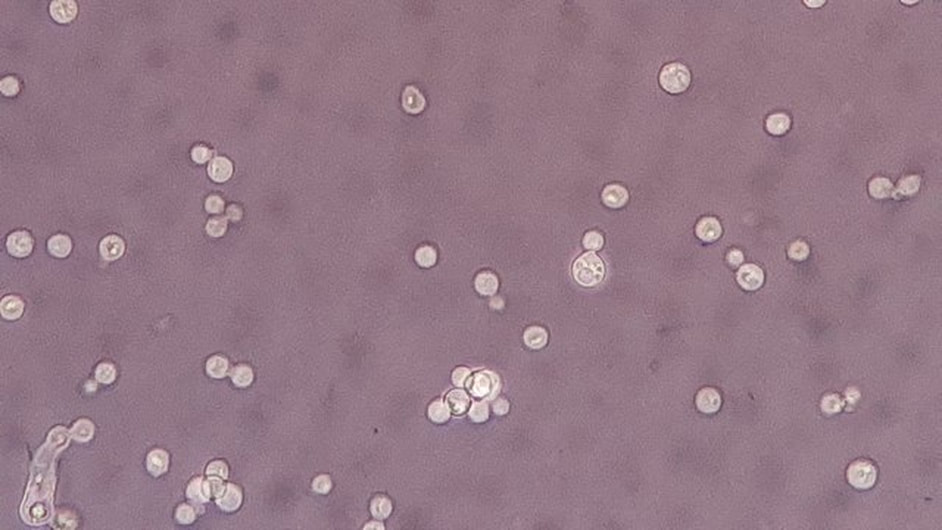
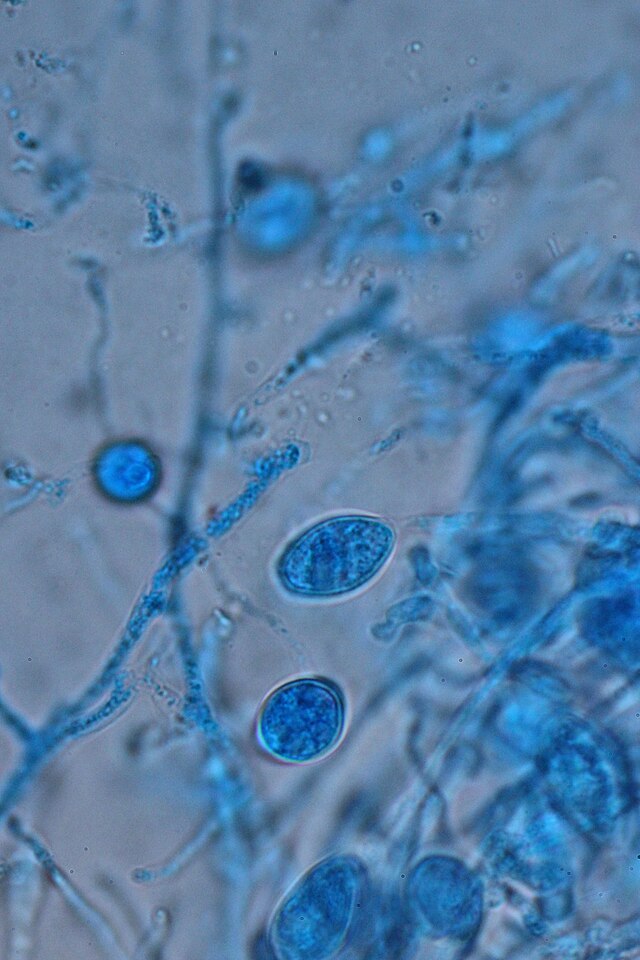
india ink:
India Ink is a procedure that is used to look for encapsulated yeasts such as Cryptococcus neoformans. It is critical to perform a direct exam on CSF and to include the India Ink prep to look at the CSF sediment for this organism.
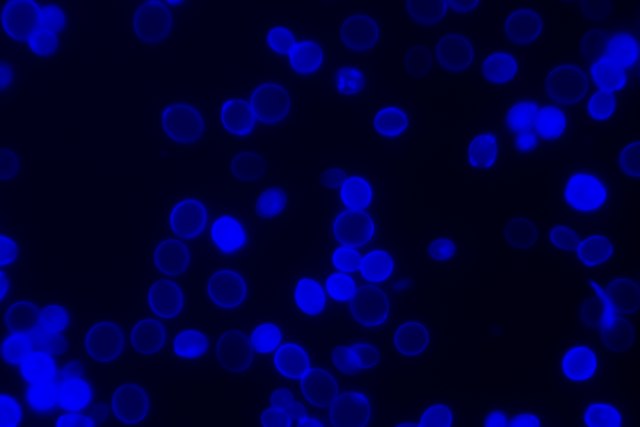
Since most bacteria and fungal organisms and white blood cells will stand out against the black India Ink background (see two images below of Cryptococcus spp and the one at the bottom of Bacillus spp bacteria), it is important to be familiar with the appearance of this particular yeast. The ink will not penetrate the cell wall OR capsule, so look only for the capsules. Yeast cells are larger than bacteria and will be budding.
It is important not to use this test as a definitive identification of this organism, but preliminary results are great. Confirmation tests are required, including culture, cryptococcal antigen testing, PCR, and mass spectrophotometry. If there is a positive, many labs require a titer test from the cryptococcal antigen test for proper treatment and for monitoring effectiveness of the treatment.
Since most bacteria and fungal organisms and white blood cells will stand out against the black India Ink background (see two images below of Cryptococcus spp and the one at the bottom of Bacillus spp bacteria), it is important to be familiar with the appearance of this particular yeast. The ink will not penetrate the cell wall OR capsule, so look only for the capsules. Yeast cells are larger than bacteria and will be budding.
It is important not to use this test as a definitive identification of this organism, but preliminary results are great. Confirmation tests are required, including culture, cryptococcal antigen testing, PCR, and mass spectrophotometry. If there is a positive, many labs require a titer test from the cryptococcal antigen test for proper treatment and for monitoring effectiveness of the treatment.
https://upload.wikimedia.org/wikipedia/commons/thumb/6/6f/Cryptococcus_neoformans_using_a_light_India_ink_staining_preparation_PHIL_3771_lores.jpg/1280px-Cryptococcus_neoformans_using_a_light_India_ink_staining_preparation_PHIL_3771_lores.jpg
https://upload.wikimedia.org/wikipedia/commons/thumb/d/dd/Cryptococcus_neoformans_in_India_Ink_from_culture_Microscopic_Footage.jpg/640px-Cryptococcus_neoformans_in_India_Ink_from_culture_Microscopic_Footage.jpg

https://upload.wikimedia.org/wikipedia/commons/thumb/6/62/Bacillus_anthracis_Indian_Ink_capsule_stain.tif/lossy-page1-640px-Bacillus_anthracis_Indian_Ink_capsule_stain.tif.jpg
Calcofluor White Stain:
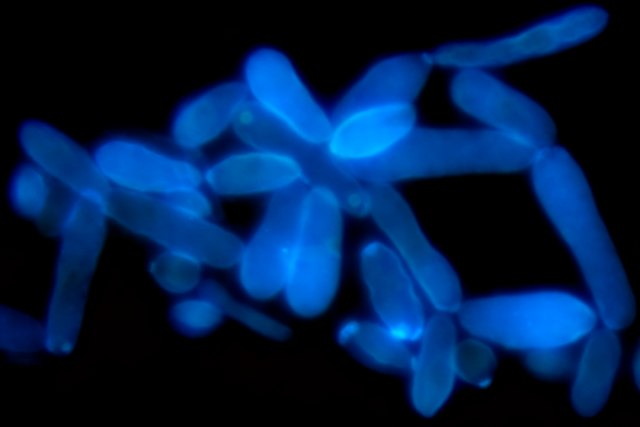
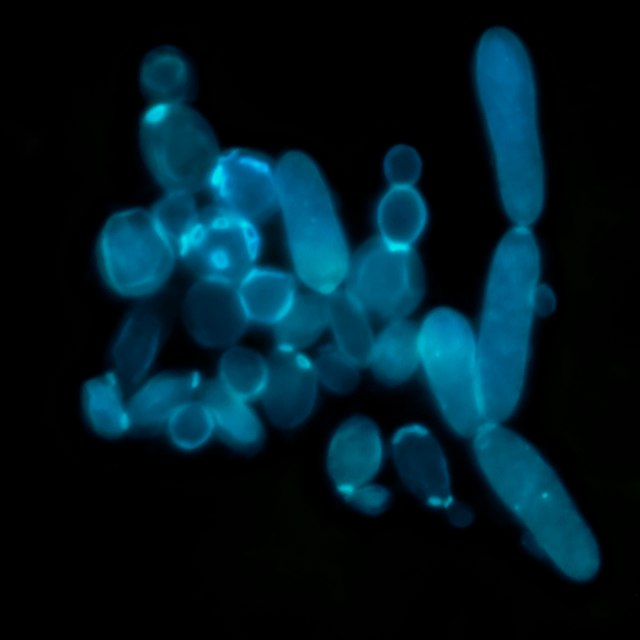
Calcofluor white stain is not used by all laboratories, but this stain can be used with fluorescence microscopy. Calcofluor white is a bleaching agent and it's used in the paper and textile industry. It's in a lot of paper, textiles, toilet paper, and paper towels. This is the reason that so many products containing this stain fluoresce under UV blacklight.
In mycology, calcofluor white is absorbed into the chitin of the fungal cell wall, causing it to produce a chalk-white or apple-green fluorescence depending on the microscope excitation wavelength under the UV microscope. Some laboratories will add a drop of 10% KOH to a nail to dissolve background cellular debris, making it easier for the calcofluor white to penetrate the fungal cell wall.
In mycology, calcofluor white is absorbed into the chitin of the fungal cell wall, causing it to produce a chalk-white or apple-green fluorescence depending on the microscope excitation wavelength under the UV microscope. Some laboratories will add a drop of 10% KOH to a nail to dissolve background cellular debris, making it easier for the calcofluor white to penetrate the fungal cell wall.

https://upload.wikimedia.org/wikipedia/commons/thumb/2/2f/%D0%9D%D0%B8%D1%82%D0%B8_%D0%BF%D0%BB%D0%B5%D1%81%D0%B5%D0%BD%D0%B8%2C_%D1%84%D0%BB%D1%83%D0%BE%D1%80%D0%B5%D1%81%D1%86%D0%B5%D0%BD%D1%86%D0%B8%D1%8F%2C_%D0%BA%D0%B0%D0%BB%D1%8C%D0%BA%D0%BE%D1%84%D0%BB%D1%8E%D0%BE%D1%80_%D0%B1%D0%B5%D0%BB%D1%8B%D0%B9.tif/lossy-page1-640px-%D0%9D%D0%B8%D1%82%D0%B8_%D0%BF%D0%BB%D0%B5%D1%81%D0%B5%D0%BD%D0%B8%2C_%D1%84%D0%BB%D1%83%D0%BE%D1%80%D0%B5%D1%81%D1%86%D0%B5%D0%BD%D1%86%D0%B8%D1%8F%2C_%D0%BA%D0%B0%D0%BB%D1%8C%D0%BA%D0%BE%D1%84%D0%BB%D1%8E%D0%BE%D1%80_%D0%B1%D0%B5%D0%BB%D1%8B%D0%B9.tif.jpg
|
https://upload.wikimedia.org/wikipedia/commons/thumb/4/40/%D0%94%D1%80%D0%BE%D0%B6%D0%B6%D0%B8%2C_%D0%BE%D0%BA%D1%80%D0%B0%D1%81%D0%BA%D0%B0_%D0%BA%D0%B0%D0%BB%D1%8C%D0%BA%D0%BE%D1%84%D0%BB%D1%8E%D0%B0%D1%80_%D0%B1%D0%B5%D0%BB%D1%8B%D0%B9_1.tif/lossy-page1-640px-%D0%94%D1%80%D0%BE%D0%B6%D0%B6%D0%B8%2C_%D0%BE%D0%BA%D1%80%D0%B0%D1%81%D0%BA%D0%B0_%D0%BA%D0%B0%D0%BB%D1%8C%D0%BA%D0%BE%D1%84%D0%BB%D1%8E%D0%B0%D1%80_%D0%B1%D0%B5%D0%BB%D1%8B%D0%B9_1.tif.jpg
|
https://upload.wikimedia.org/wikipedia/commons/thumb/1/19/%D0%9A%D0%BB%D0%B5%D1%82%D0%BA%D0%B8_%D0%B4%D1%80%D0%BE%D0%B6%D0%B6%D0%B5%D0%B9_%D0%B8%D0%B7_%D0%BD%D0%B0%D0%BF%D0%B8%D1%82%D0%BA%D0%B0_%D0%BA%D0%BE%D0%BC%D0%B1%D1%83%D1%87%D0%B0_3.tif/lossy-page1-640px-%D0%9A%D0%BB%D0%B5%D1%82%D0%BA%D0%B8_%D0%B4%D1%80%D0%BE%D0%B6%D0%B6%D0%B5%D0%B9_%D0%B8%D0%B7_%D0%BD%D0%B0%D0%BF%D0%B8%D1%82%D0%BA%D0%B0_%D0%BA%D0%BE%D0%BC%D0%B1%D1%83%D1%87%D0%B0_3.tif.jpg
|
https://upload.wikimedia.org/wikipedia/commons/thumb/5/5a/%D0%9A%D0%BB%D0%B5%D1%82%D0%BA%D0%B8_%D0%B4%D1%80%D0%BE%D0%B6%D0%B6%D0%B5%D0%B9_%D0%B8%D0%B7_%D0%BD%D0%B0%D0%BF%D0%B8%D1%82%D0%BA%D0%B0_%D0%BA%D0%BE%D0%BC%D0%B1%D1%83%D1%87%D0%B0.tif/lossy-page1-640px-%D0%9A%D0%BB%D0%B5%D1%82%D0%BA%D0%B8_%D0%B4%D1%80%D0%BE%D0%B6%D0%B6%D0%B5%D0%B9_%D0%B8%D0%B7_%D0%BD%D0%B0%D0%BF%D0%B8%D1%82%D0%BA%D0%B0_%D0%BA%D0%BE%D0%BC%D0%B1%D1%83%D1%87%D0%B0.tif.jpg
|
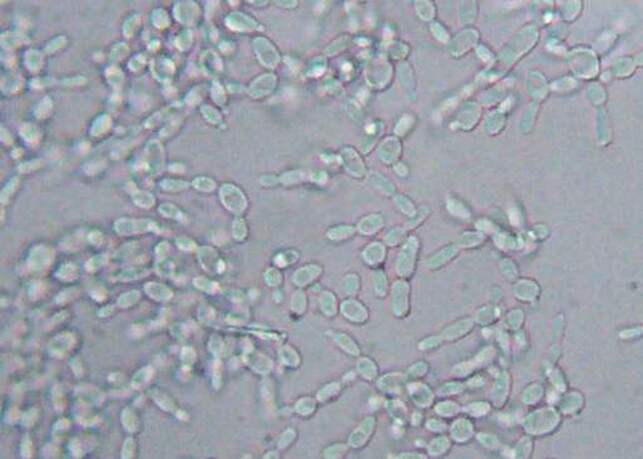
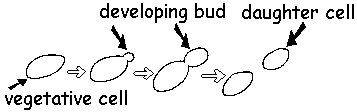
Yeasts (budding):
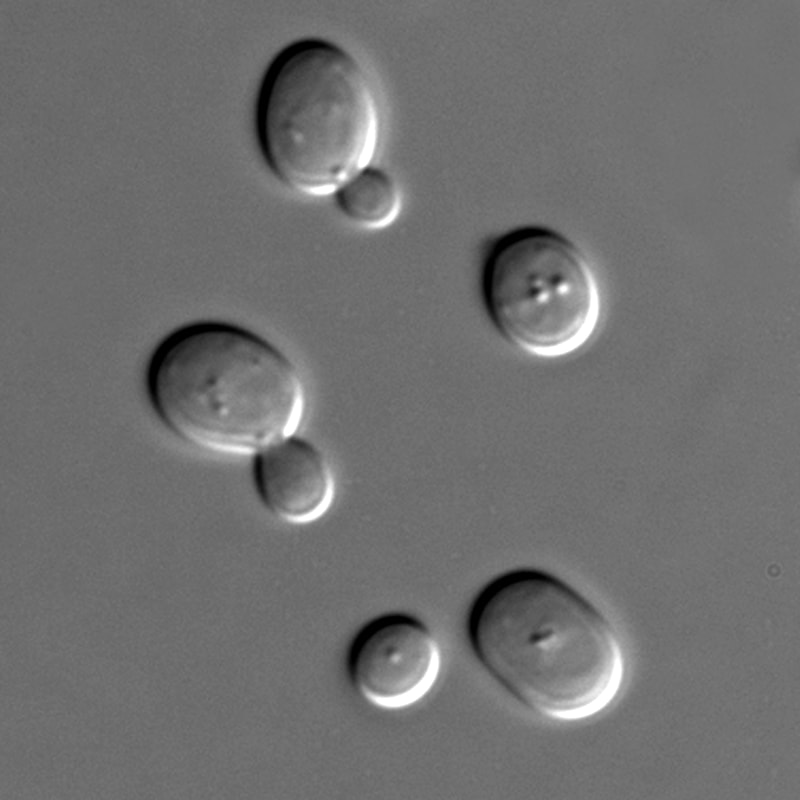
Budding yeast Saccharomyces cerevesiae (known as "Baker's Yeast"); Image By Masur - Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=1069017
|
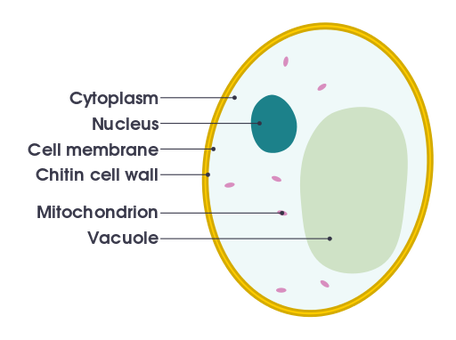
The structure and morphology of a unicellular yeast cell: cell membrane surrounding cytoplasm with organelles, cell wall made out of the carbohydrate chitin surrounds the cell membrane, and it is oval-shaped;By domdomegg (Own work) [CC BY 4.0 (http://creativecommons.org/licenses/by/4.0)], via Wikimedia Commons
|
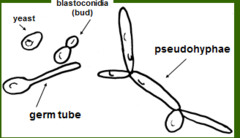
Yeast cells, spores, and pseudohyphae;By Y tambe - Y tambe's file, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=233284
|
By Y tambe - Y tambe's file, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=233284
|

Hyphae of a mold called Penicillium;By Y_tambe - Y_tambe's file, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=1527577
|
Mycelium;By Bob Blaylock - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=11194179
|
Fungal morphology:
It is important to understand fungal morphology (shape, color, and characteristics) in order to understand their virulence factors, how to recognize microscopic and macroscopic features for identification, and which parts of the fungi serve as targets for antifungal therapy. Morphology includes the microscopic and the macroscopic characteristics of the fungi of interest. The morphology of fungi includes:
- The Cell Membrane
- Bilayer lipid membrane
- The innermost layer
- Surrounds the cytoplasm and protects it and serves as a barrier for protection
- Contains the polysaccharide chitin, which gives it strength
- Contains sterols, particularly ergosterol
- Antifungals/fungicides in the polyene category, such as amphotericin B and nystatin, bind to this sterol and poke holes in the cell membrane to damage it. They are amphiphilic, change the temperature, turning the cell membrane into a more crystal rather than fluid state. The change in density causes the electrolytes and salts to leak out of the cell, causing it to die. Human cells do not contain ergosterol, however, they contain similar cholesterol, so there is some risk to human cells when given some of these fungicides. Amphotericin B carries a risk of nephrotoxicity with it (damage to the kidneys) when administered by IV for a systemic infection, however, the benefits may outweigh the risks.
- The Azole category of antifungals prevent the precursor lanosterol from converting into ergosterol. For example, Ketoconazole blocks ergosterol synthesis.
- Thiazoles
- Allylamines block an enzyme needed for ergosterol synthesis.
- Echinocandins block production of glucan needed for the cell wall. These include the fungins (Caspofungin, Micafungin, Anadulafungin). These are for resistant Candida infections.
- Other antifungals include balsam fir, tea tree oil,neem oil, rosemary oil, jojoba oil, citronella oil, oregano oil, charcoal, zinc, sulfur, selenium disulfide, coal tar, copper II sulfate, iodide, aloe, benzoic acid, and the stains used in Microbiology, such as Carbolfuchsin and Crystal Violet. Any prescribed antifungal has a risk of causing an allergic reaction. Also, many antifungals have known drug interactions. All of this must be carefully monitored in patients.
- The Cell Wall
- Surrounds the cell membrane
- Thick
- Made up of carbohydrate and protein
- Antigens to the human immune system
- Capsule
- A polysaccharide coating that goes around the cell wall
- Antiphagocytic to "hide" from the immune system
- Virulence factor
- Found in yeast like Cryptococcus neoformans
- Can be stained with India Ink stain
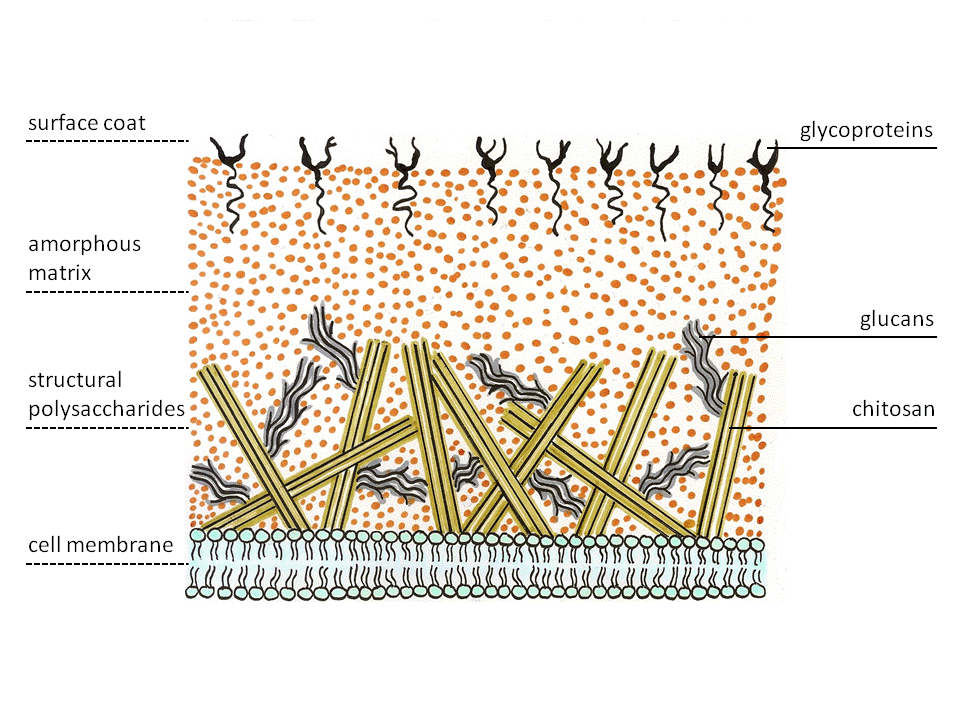
By Maya and Rike (Own work) [CC BY 3.0 (http://creativecommons.org/licenses/by/3.0)], via Wikimedia Commons
fungal infections: MYCOSES
Pathogenic fungal infections to humans ranges from superficial to deep and systemic. Some are easy to treat, whereas others can be deadly. Types of infections include the following:
- Superficial Fungal Infections (Skin)
- Superficial fungal infections include pityriasis versicolor and tinea nigra, which produce pigments that change the color of the skin. Pityriasis versicolor, or tine versicolor, causes a chronic superficial fungal infection. The skin becomes either hyperpigmented (too much pigment) or hypopigmented (too little), resulting in patches on the skin. If exposed to the UV rays from the sun, these patches will appear white against the tanned skin. Fungi like Malassezia furfur can cause such infections. Tinea nigra results in dark brown-to-black appearing patches on the hands or feet. These patches are caused by fungi like Exophialia werneckii.
- Cutaneous Fungal Infections (Skin, Hair, Nails)
- Cutaneous fungal infections are caused by the dermatophytes, a group of >30 species of fungi that cause opportunistic infections by feeding of of the dead keratin layer of the skin, hair and nails
- Dermatophytes secrete keratinase, an enzyme that breaks down keratin, the primary structural protein found in skin, hair and nails
- Infections result in scaling or peeling of the skin, hair loss, or breaking and crumbling of the nails
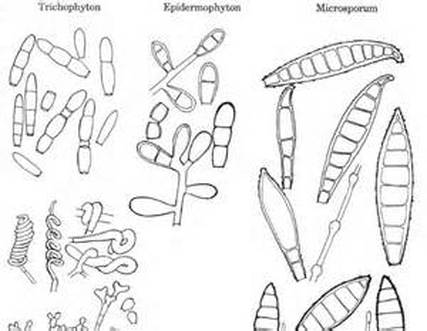
- The most common dermatophytes include:
- Trichophyton species
- Epidermophyton species
- Microsporum species
- Types of Infections:
- Tinea corporis (body) or ringworm
- Results in annular lesions with irregular borders
- There may be more than one lesion
- Inflamed, itchy and red
- Prominent hair follicles
- Fungi involved include: E. floccosum, T. rubrum, M. canis, T. verrucosum, T. mentagrophytes, T. erinacei, M. versicolor, M. equinum, T. equinum, M. gypseum
- Tinea cruris, or jock itch
- Scaling in the groin extending to the upper surface of the thigh and around the perineum, often with a raised margin
- Mainly affects adult men
- Tends to be bilateral
- Results in redness, itching, scaling, rash
- Fungi involved include T. rubrum, T. interdigitale, E. floccosum
- Tinea pedis, or Athlete's foot
- This is the most frequently occurring dermatophyte infection
- Caused by T. rubric, T. mentagrophytes, T. interdigital, E. floccosum
- Scaling, itching, chronic dry scaly rash or blisters or secondary bacterial infection with greenish discharge
- Tinea capitis, or scalp infection
- Scalp ringworm
- Usually affects kids with patches of scalp hair loss and scaling
- Erythema background with crusting and suppuration
- Fungi: Microsporum spp, Trichophyton schoenleinii or T. tonsurans or T. verrucosum
- Tinea manuum
- Dry dermatophytosis affecting the palms and some foot infections and causing scaling and itching
- Caused by T. rubrum
- Tinha unguium, or nail infection (onychomycosis)
- Onychomycosis
- Infection of the nail plate, producing thickened, discolored and broken nails
- Occurs more frequently in the toenails and surrounding skin
- Rare in children
- Caused by T. rubrum or T. interdigitale
- Tinea facei
- Ringworm of the face
- Erythema, scaling, soreness
- Sunlight causes it to flare up
- Tinea barbae
- Affects the neck and beard
- Very inflammatory and painful
- T. verrucosum
- Tinea incognito
- Occurs after application of a potent corticosteroid cream
- Loss of scaling and annular rim, formation of prominent pustules or papules
- Tinea imbricata
- An exotic infection caused by T. concentricum
- Concentric scales on the skin
- Majocchi's Granuloma
- Late stage hair shaft invasion
- Persistent granuloma remains in the skin
- T. rubrum
- Tinea corporis (body) or ringworm
- Diagnosis of Infection:
- Skin scrapings are sent to the lab to be dissolved in KOH, or potassium hydroxide, which dissolves the keratin, then observed microscopically with calcofluor white stain to reveal branched hyphae
- Hair and skin samples can be directly examined with a UV Wood's lamp for a bright green fluorescence of certain fungi
- Treatment:
- Topical imidazole or oral griseofulvin
- Keep skin dry, free of moisture, out of the sun
- Subcutaneous Fungal Infections (Below the Skin)
- These infections have gained access to the body after trauma to the skin, such as a cut or puncture wound.
- Infections are typically localized to the subcutaneous tissue.
- Infection can spread via the lymphatics to local lymph nodes.
- These fungi normally reside in the soil and only cause opportunistic infections when at the right place at the right time in the right conditions.
- Infections include sporotrichosis or chromoblastomycosis.
- Fungi that cause these infections are things like Sporothrix schenckii or Phialophora or Cladosporium species.
- Identification of the fungi is the same as above.
- Treatment includes itraconazole and excision.
- Systemic Fungal Infections (Disseminated)
- These type of infections occur if the patient is immunocompromised and/or if the fungi spread through the lymphatic system to other parts of the body or through the bloodstream.
- Infections include things like histoplasmosis, blastomycosis, or coccidiomycosis.
- Dimorphic fungi play a role in human infection and release spores that are typically inhaled by humans, growing as yeast cells inside the body.
- Fungi: Histoplasma species, Blastomyces species, Coccidiodes immitis, Paracoccidiodes species
- Other Infections: Otomycosis (Ear Infection)
- Otomycosis is a superficial infection of the ear canal. It can be chronic or acute or subacute.
- Symptoms: pain, inflammation, redness, scaling, itching, loss of hearing or muffled hearing due to the blockage of the ear by hyphae or debris
- Typically caused by Aspergillus niger, Aspergillus fumigatus, Aspergillus terreus
- Rarely caused by Scopulariopsis, Paecilomyces, Mucor, Rhizopus, Candida or the dermatophytes
- Other Infections: Keratitis (Eye Infection)
- Mycotic keratitis manifests as a corneal ulcer, hypopyon or even both. This is caused by corneal trauma, corneal disease or glaucoma, which may predispose the individual to infection.
- Can be caused by many different types of fungi, but the most common include Fusarium solani, Fusarium spp, Aspergillus fumigatus, other Aspergillus spp, C. albicans, Curvularia lunata, Penicillium spp, Phialophora verrucosa, Macrophoma spp, Trichosporon
- Candidiasis
- C. glabrata, C. auris are the strains of most concern, though any species of Candida can result in this type of infection.
- C. glabrata and C. auris are of low virulence, however, are a cause of secondary infection in patients with underlying immunocompromisation due to other illnesses such as cancer, diabetes mellitus, or certain types of treatments and medications (antibiotics, steroids, chemotherapy, radiation, immunosuppressants, etc...)
- Kidneys, lungs, bladder, blood, skin, other organs can be infected
- Macroscopic appearance on agar: C. glabrata and C. auris are identical in both macroscopic and microscopic examinations. They produce cream-colored, smooth, glistening colonies but some strains become brownish-gray as they age. Microscopically: budding yeast cells without pseudohyphae, measuring 2.5-3 x 4 microns, oval, round and elongated cells; Ferment glucose and trehalose
Clinical Mycology Basics:
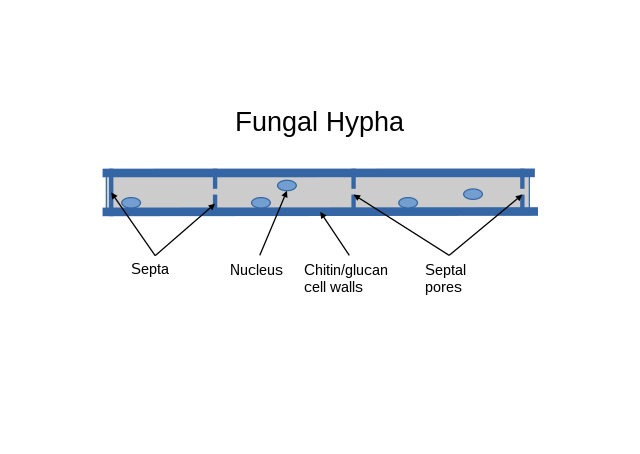
Mycology is the study of fungi. Fungi are eukaryotic microbes, meaning that they contain a "true nucleus", they do not contain chlorophyll, and they absorb all their nutrients from their surrounding environment, particularly from dead and decaying organic material. Fungi are observe both microscopically and macroscopically (as colonies growing on agar plates). Fungi consist of both mold forms and yeast forms. Microscopically, fungal cells are seen as either molds in the form of hyphae or as yeasts. Hyphae are either aseptate (containing no cross walls) or septate (containing cross walls). Most of the Zygomycota are aseptate. Ascomycota, Basidiomycota and Deuteromycota have septate hyphae.
The major features by which molds are routinely identified include: mode of sporulation, morphology and the arrangement of spores. To confirm that an unknown mold is one of the pathogenic dimorphic fungi, you can perform a culture conversion from the mold form to the yeast form.
The major features by which molds are routinely identified include: mode of sporulation, morphology and the arrangement of spores. To confirm that an unknown mold is one of the pathogenic dimorphic fungi, you can perform a culture conversion from the mold form to the yeast form.
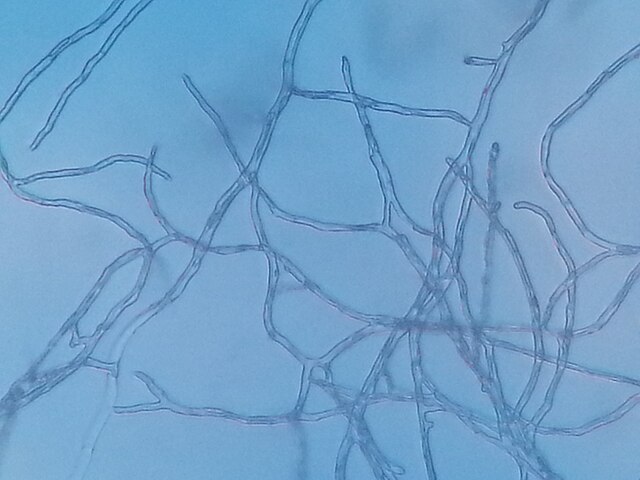
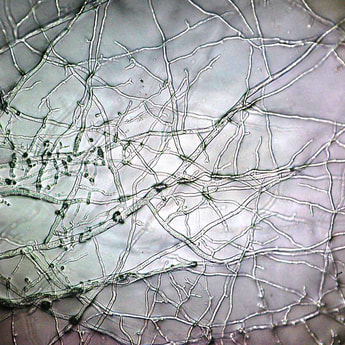
Hyphae morphology:
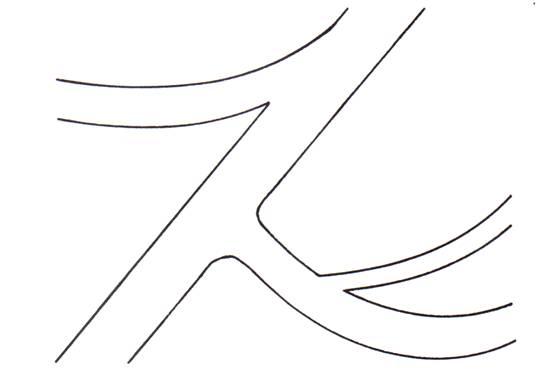
Aseptate hyphae.
Image courtesy studyblue.com
|
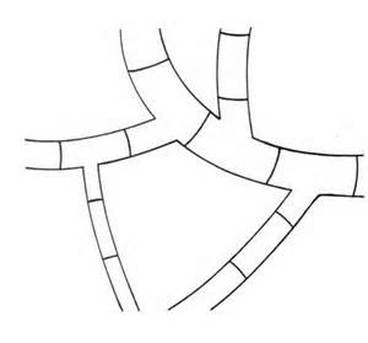
Septate hyphae, containing cross walls. Image courtesy studyblue.com
|
Rhizopus mucor is in the zygomycete class of fungi, and it has wide, ribbon-like, smooth, aseptate hyphae without any cross walls. https://upload.wikimedia.org/wikipedia/commons/thumb/f/fa/Mucor_in_LPCB_tease_mount.jpg/640px-Mucor_in_LPCB_tease_mount.jpg

This is an image of septate hyphae. You can visibly see the cross walls. https://upload.wikimedia.org/wikipedia/commons/thumb/f/f0/Fungal_hyphae.jpg/640px-Fungal_hyphae.jpg
Hyphae are either vegetative (food-absorbing portion of hyphae mycelium under the agar surface), or aerial (extending above the surface of the agar). Aerial hyphae may support other structures, such as conidia, which are reproductive structures. The aerial hyphae are responsible for the distinct characteristics, color and texture of the front side of the colony, whereas the vegetative hyphae are responsible for the characteristics on the reverse side. Both aid in identification and speciation. This is why it is important to observe BOTH sides of the plate for mold growth and characteristics.
Aerial hyphae above the surface of the agar, and vegetative hyphae below the surface of the agar
|

Aerial hyphae and conidia above the surface of the agar, and vegetative hyphae below the surface of the agar are shown here from the mold Aspergillus Niger. https://upload.wikimedia.org/wikipedia/commons/thumb/c/c7/Aspergillus_niger_hyphae.jpg/640px-Aspergillus_niger_hyphae.jpg
|
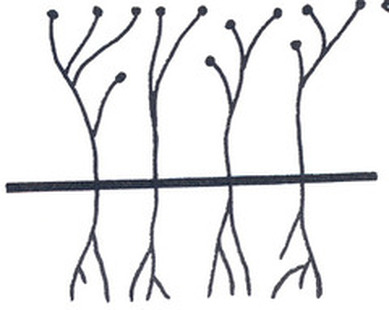
Favic Chandeliers are another fungal structure that resemble the antlers of a buck deer or moose. The ends of the hyphae are blunt, rounded, and branched and aid in the identification of Trichophyton schoenleinii, causative agent of ringworm of the skin, hair or nails.
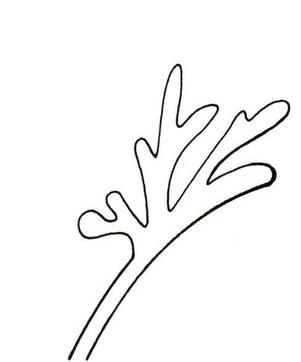
Favic chandeliers resemble buck deer or moose antlers and aid in the diagnosis of T. schoenleinii.
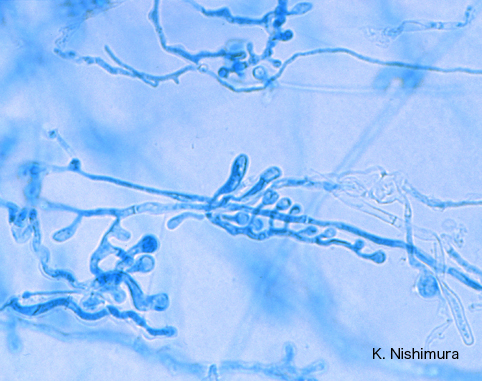
Trichophyton schoenleinii by K. Nishimura. https://external-content.duckduckgo.com/iu/?u=http%3A%2F%2Fwww.pf.chiba-u.jp%2Fgallery%2Fimg%2Ffungi%2Ft%2FTrichophyton_schoenleinii_microscopy.jpg&f=1&nofb=1&ipt=fcd5a4b02f571bca4a6ebc69e782ee09bc0ba356b4ee578a034e4a88ba538fdb&ipo=images
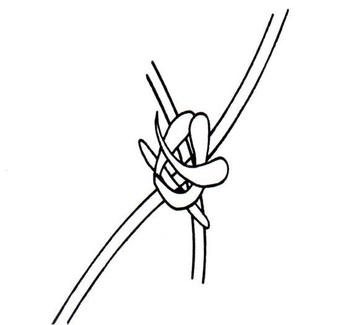
Nodular Organs are another fungal characteristic that include knotted and twisted hyphae.
Other fungal characteristics include raquet hyphae, in which hyphae look like tennis racquets or badminton racquets stacked on top of one another.

Alternaria species mold is shown here, and you can see the repeating, alternating racquet hyphae. https://upload.wikimedia.org/wikipedia/commons/thumb/6/67/Chain_of_conidia_of_a_Alternaria_sp._fungus_PHIL_3962_lores.jpg/640px-Chain_of_conidia_of_a_Alternaria_sp._fungus_PHIL_3962_lores.jpg
Spiral hyphae are not as common, but may be seen in older cultures, and may be flat and curved or more spiral-shaped like a corkscrew.
This image is a lactophenol cotton blue scotch tape wet mount of Fusarium spp, but you can see an example of spiral hyphae; Image taken by Jeanette Sprute, M-ASCP, MT-AMT, MS-Biology, Microbiologist at a hospital laboratory
On this lactophenol cotton blue scotch tape prep mount of a mold, observe the spiral hyphae example in the middle; Image taken by Jeanette Sprute, M-ASCP, MT-AMT, MS-Biology, Microbiologist at a hospital laboratory
https://external-content.duckduckgo.com/iu/?u=http%3A%2F%2Fwww.tgw1916.net%2Fimages%2Fm_Trichophyton_mentagrophytes.jpg&f=1&nofb=1&ipt=4426522faf04385454093415a13b6b6439ed9e5431c8db94ccb64d9927b5ac45&ipo=images
Yeasts are observed as single cells, oval-to-round, which may or may not exhibit budding and/or pseudohyphae. Many fungi are either a mold or a yeast in form, however, there are a few that can exhibit both characteristics depending upon the temperature, moisture level, and environment. This is referred to as dimorphism. If the fungus is incubated at room temperature, which is about 25 or 30 degrees Celsius, it will grow as a mold. If the fungus is incubated at body temperature, or 37 degrees Celsius, it will convert to a yeast form. Often times, if the mycologist converts the fungus from one form to another, this is one of the primary aids in the identification of the organism, which is critical since most of these types of fungi cause serious, even fatal illnesses.
These budding yeast cells are also referred to as "blastoconidia" or "blastospores"
|
|
reproduction and conidiogenesis:
Reproduction of fungi is either asexual or sexual. Asexual reproduction occurs by binary fission (mitosis), with nuclear and cytoplasmic division. This is also known as conidiogenesis, or the formation of conidia. Conidia are either formed by budding from a parent cell into a daughter cell, from which point it separates (blastic) or a septum forms first and then the growing point ahead of it becomes the daughter cells, as seen in arthroconidia or in racquet hyphae. Sexual reproduction occurs via the joining of two nuclei into a single zygote.
Conidia Formation: Conidiogenesis:
Conidiogenesis is conidia formation asexually. This is the anamorph stage. Conidia may form either blastically or thallically. Blastically means that the conidiogeneous (parent) cell gets bigger first, then a septum then forms and separates the enlarged portion from the daughter cell, which breaks off on its own when mature. When conidia form thallically, the septum forms first. The growing point in front of it becomes the new daughter cell.
There are a few prefixes that are important in terms of how the cell wall layers develop:
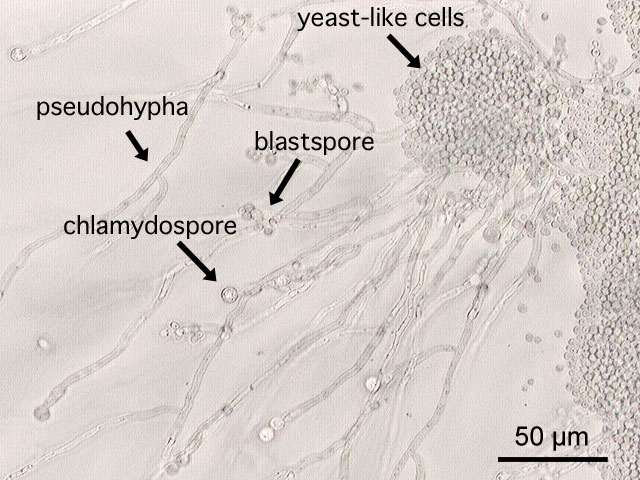
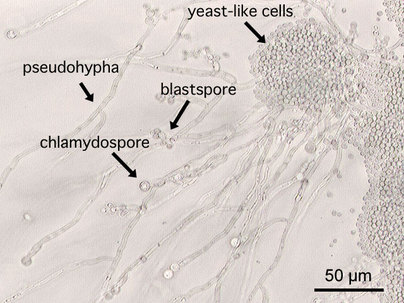
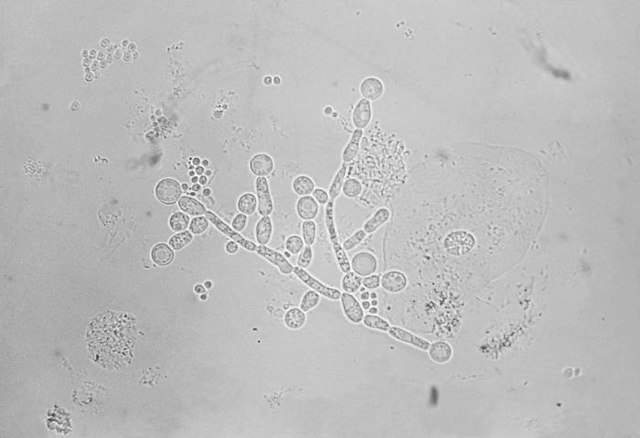
Blastoconidia (blastospores) are produced by budding, as seen in yeasts like Candida spp, or in molds like Cladosporium. Candida albicans' blastoconidia elongate and form pseudohyphae, which are constricted at the points where they attach. This differentiates them from true hyphae, which may or may not have septations or cross walls.
Conidia Formation: Conidiogenesis:
Conidiogenesis is conidia formation asexually. This is the anamorph stage. Conidia may form either blastically or thallically. Blastically means that the conidiogeneous (parent) cell gets bigger first, then a septum then forms and separates the enlarged portion from the daughter cell, which breaks off on its own when mature. When conidia form thallically, the septum forms first. The growing point in front of it becomes the new daughter cell.
There are a few prefixes that are important in terms of how the cell wall layers develop:
- Holo: means that ALL cell wall layers of the parent cell are involved in the daughter cell development
- Entero: means that just the inner cell wall layers are involved in the daughter cell development
- Arthric: means that the daughter cells fragment and break off within the hyphal strand, then they are dispersed
Blastoconidia (blastospores) are produced by budding, as seen in yeasts like Candida spp, or in molds like Cladosporium. Candida albicans' blastoconidia elongate and form pseudohyphae, which are constricted at the points where they attach. This differentiates them from true hyphae, which may or may not have septations or cross walls.
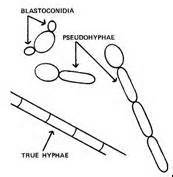
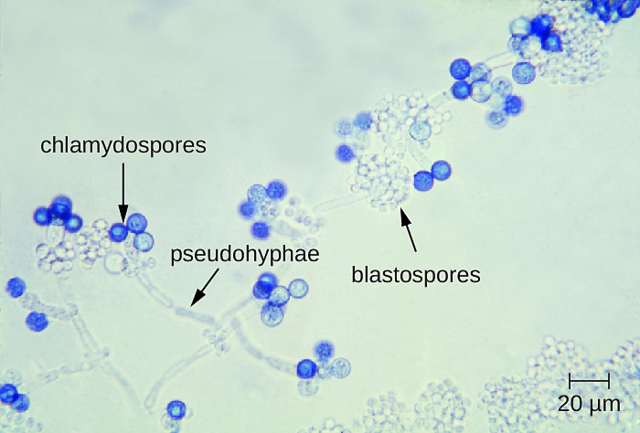
https://upload.wikimedia.org/wikipedia/commons/thumb/d/df/Candida_pseudohyphae%2C_chlamydospores%2C_blastospores.png/640px-Candida_pseudohyphae%2C_chlamydospores%2C_blastospores.png
Candida albicans is observed here with budding and pseudohyphae
|
Cladosporium
|
https://upload.wikimedia.org/wikipedia/commons/thumb/7/75/Fungal_hypha.svg/640px-Fungal_hypha.svg.png
Poroconidia are formed when the daughter cell pushes through a tiny hole or pore at the top of the parent cell, which may be in a conidiophore (a long stalk-like structure), or a specialized conidiogenous (parent) cell. Bipolaris spp is an example of this.
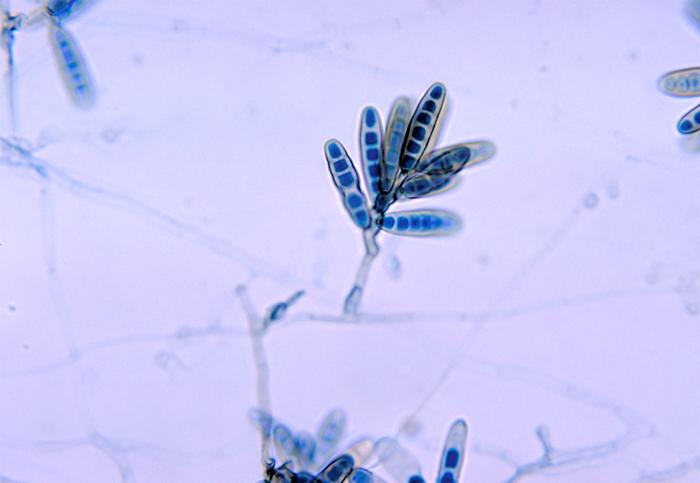
Bipolaris spp; https://upload.wikimedia.org/wikipedia/commons/thumb/a/a1/Conidiophore_of_the_fungus_Bipolaris_hawaiiensis_PHIL_4338_lores.jpg/640px-Conidiophore_of_the_fungus_Bipolaris_hawaiiensis_PHIL_4338_lores.jpg
|
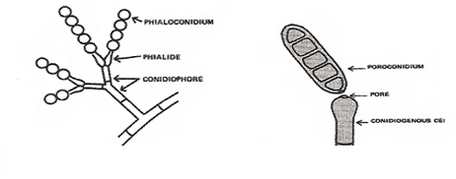
Poroconidia formation
|
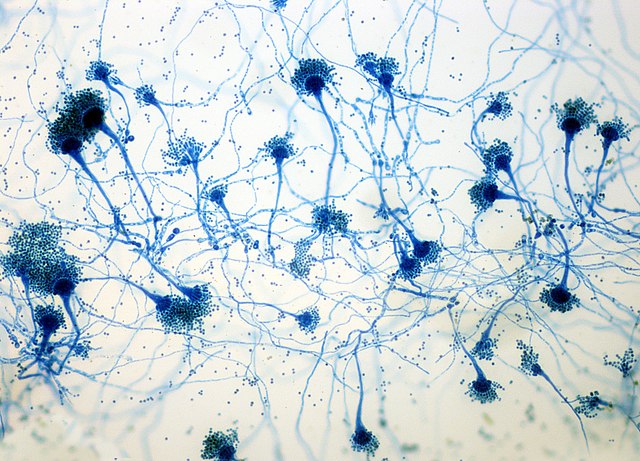
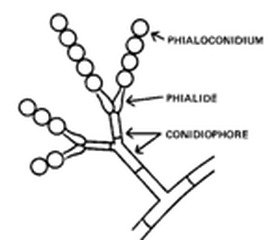
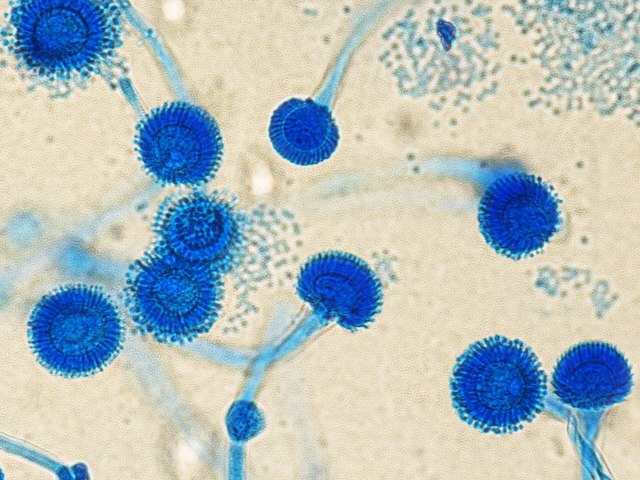
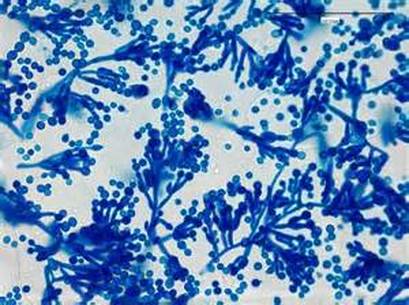
Phialoconidia are structures that are formed from a phialide, which is a vase-shaped or flask-shaped structure at the end of a conidiophore (supporting stalk). Penicillium spp and Aspergillus spp are examples of this. The terminal "cup-shaped" structure at the end of the phialide is referred to as a collarette. The structure of Penicillium spp phialides and strings of phialoconidia resemble a "witch's broom" or a "skeleton's hand". That is the best way to remember this one.
|
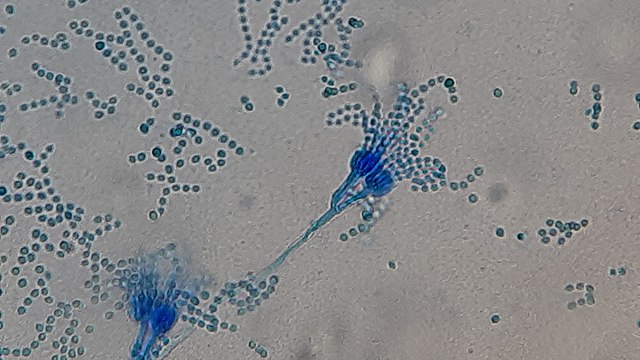
Penicillium spp (resembles a "skeleton hand" or a "witch's broom"; https://upload.wikimedia.org/wikipedia/commons/thumb/8/87/Penicillium_in_LPCB_Tease_Mount_Microscopy.jpg/640px-Penicillium_in_LPCB_Tease_Mount_Microscopy.jpg
|
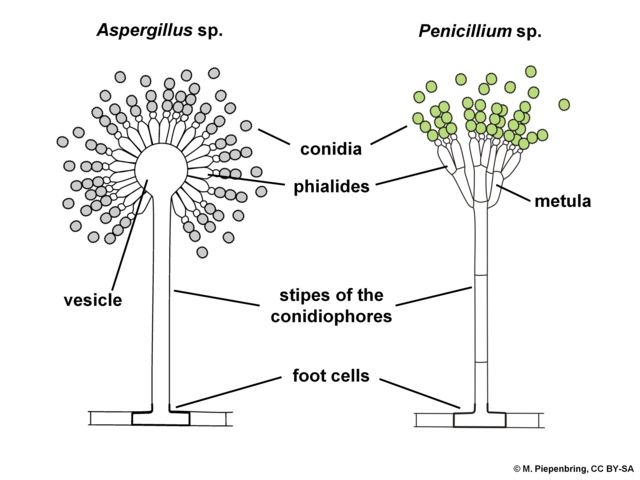
https://upload.wikimedia.org/wikipedia/commons/thumb/3/35/04_03_21_conidiophores%2C_Aspergillus%2C_Penicillium%2C_Eurotiales%2C_Ascomycota_%28M._Piepenbring%29.png/640px-04_03_21_conidiophores%2C_Aspergillus%2C_Penicillium%2C_Eurotiales%2C_Ascomycota_%28M._Piepenbring%29.png
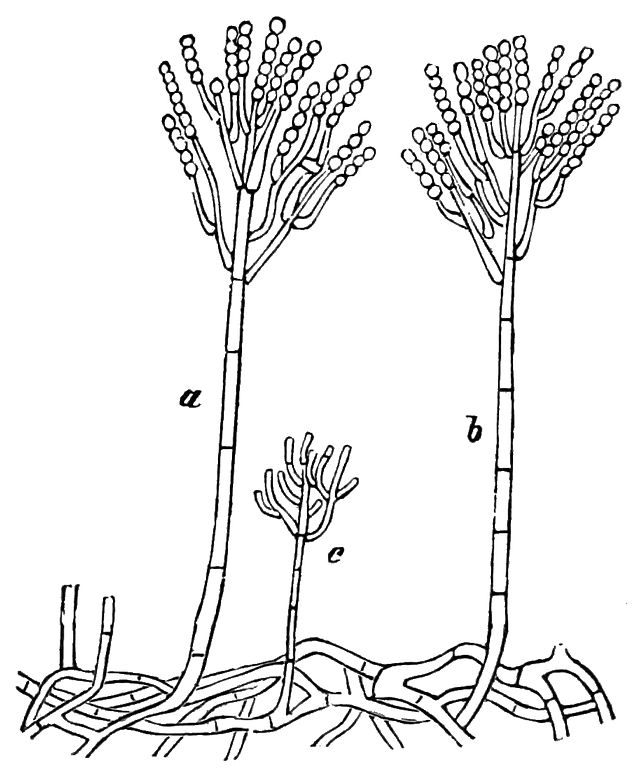
https://upload.wikimedia.org/wikipedia/commons/thumb/4/49/PSM_V09_D428_Penicillium_crustaceum.jpg/640px-PSM_V09_D428_Penicillium_crustaceum.jpg

https://upload.wikimedia.org/wikipedia/commons/thumb/f/f9/9A_400x.jpg/640px-9A_400x.jpg
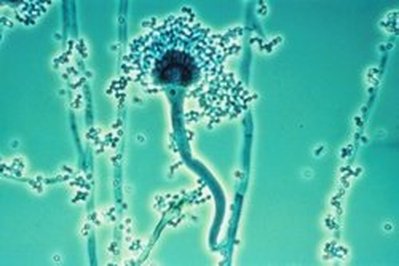
Aspergillus spp; Resembles a "fan"
|
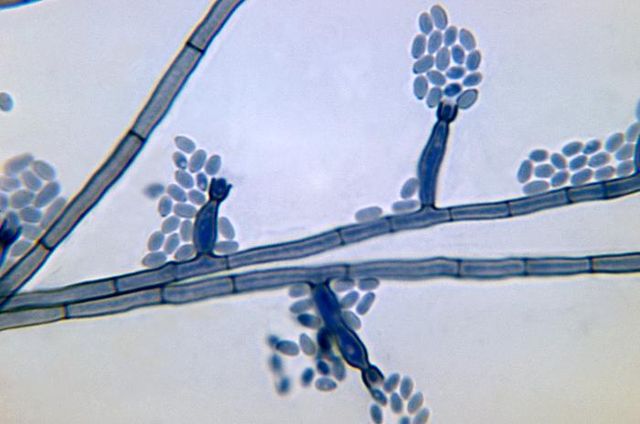
Phialophora verrucosa is a mold with septate hyphae bearing phialides that are "vase-shaped", supported phialoconidia that are oval-shaped
|
https://upload.wikimedia.org/wikipedia/commons/thumb/a/a3/Antonio_e_Biagio_e_Cesare_Arrigo_Aspergillus_fumigatus_01.jpg/640px-Antonio_e_Biagio_e_Cesare_Arrigo_Aspergillus_fumigatus_01.jpg
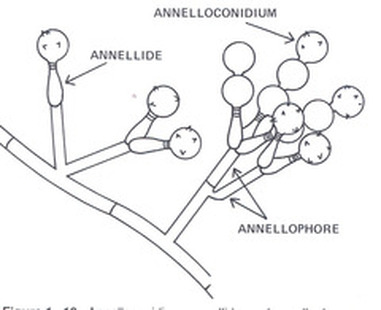
Annelloconidia are formed from inside a vase-shaped or bowling-pin shaped annellide, supported by an annellophore (stalk). Annelloconidia are "bumpy" and have a "saw-tooth" appearance. Scopulariopsis spp is an example of this.
Scopulariopsis spp
|
|

https://upload.wikimedia.org/wikipedia/commons/thumb/5/5c/Scopulariopsis_brevicaulis.jpg/640px-Scopulariopsis_brevicaulis.jpg
Macroconidia formation occurs when a whole hyphal element converts into a multicelled conidium. Remember that "macro" is "large". Microconidia formation occurs the same way, however, it remains aseptate. Remember that "micro" is "small". Macroconidia may be club-shaped, oval, elongated, curved, have a thick or thin wall, be smooth or spiny, or form on the side of the condiophore (sessile). Sometimes they are seen as one individual and somtimes they are found in clusters. Microconidia are single-celled and are typically round-to-oval or club-shaped. They, too, may be sessile, single, or found in clusters.
HINT: "MACRO" is LARGE and "micro" is small
HINT: "MACRO" is LARGE and "micro" is small
|
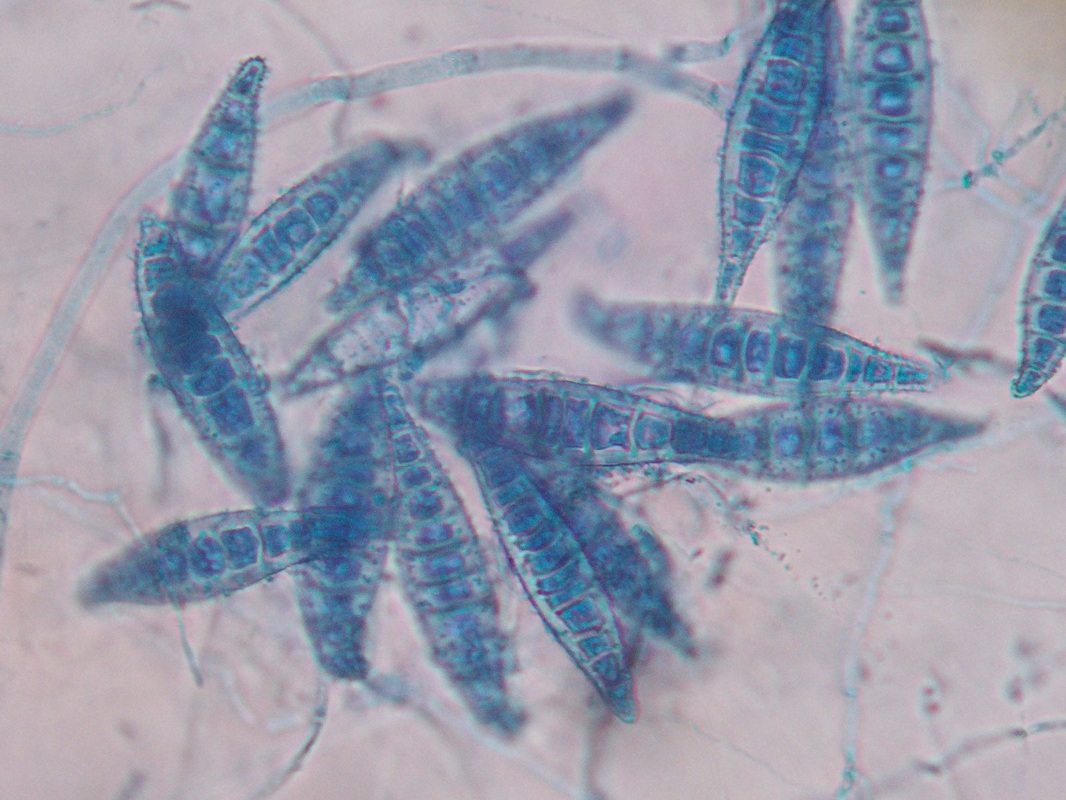
Microsporum spp; https://upload.wikimedia.org/wikipedia/commons/thumb/b/b0/Macroconidia_Microsporum_canis.JPG/640px-Macroconidia_Microsporum_canis.JPG
|

Trichophyton tonsurans species has both macroconidia and microconidia, as seen in this image; https://upload.wikimedia.org/wikipedia/commons/thumb/5/5c/Trichophyton_mentagrophytes_PHIL22306.png/640px-Trichophyton_mentagrophytes_PHIL22306.png
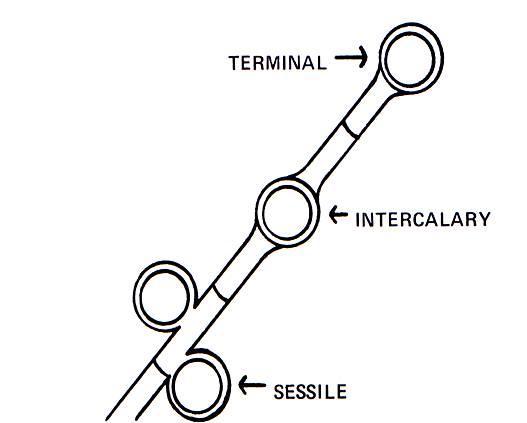
Chlamydoconidia are survival conidia that have thick walls and they form during harsh or extreme environmental conditions (extremes of temperature, pH, moisture levels, etc...). They will germinate and produce more conidia when the conditions are just right, becoming vegetative cells again. You will see them at the hyphal tip (terminal), inside the hyphal strand (intercalary), or forming on the sides (sessile). Note that these are different from the chlamydospores formed in yeasts like Candida albicans.
|
Gliocladium spp
|
Intercalary and terminal chlamydoconidia of Microsporum aoudouinii
|
Sessile chlamyoconidia; https://upload.wikimedia.org/wikipedia/commons/thumb/3/3a/G._sessile_chlamydospores.jpg/640px-G._sessile_chlamydospores.jpg
|
Terminal chlamydoconidia are formed by Candida albicans yeast and are seen in a sputum sample here. https://upload.wikimedia.org/wikipedia/commons/thumb/5/54/Candida_albicans_%28sputum%29.jpg/640px-Candida_albicans_%28sputum%29.jpg
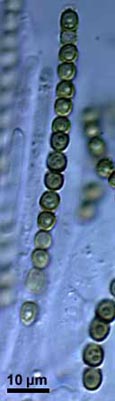
Arthroconidia are structures that fragment or break off from the hyphae through septation points that separate inside the parent hyphal strand prior to dispersing on their own. They may form next to each other inside the hyphae, or become separated by empty disjunctor cells (alternating empty spaces). Speciation is aided by the observer's ability to distinguish between arthroconidia that are adjacent or alternate. Coccidioides immitis is distinguished by its formation of disjunctor cells (fragmented). Older cells become thick-walled and they are shaped like wine barrels or rectangles.
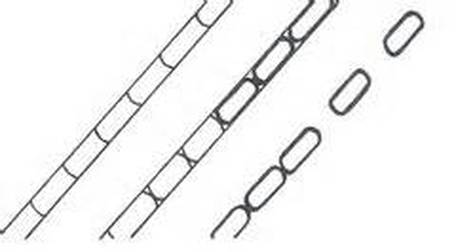
Immature, septate arthroconidia (left), disjunctor cells (middle) and mature, fragmenting arthroconidia (right)
|
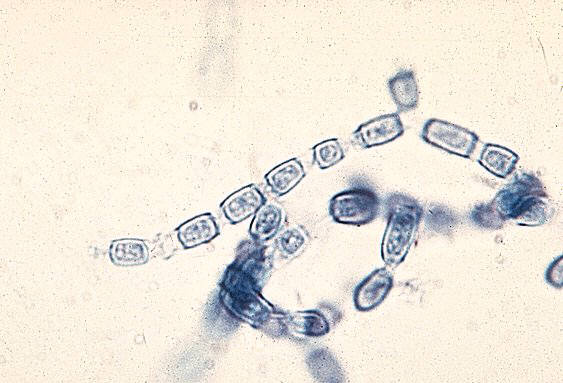
Arthroconidia of Coccidioides immitis with disjunctor cells.By http://phil.cdc.gov/PHIL_Images/11121998/00004/39G0040_lores.jpg, Public Domain, https://commons.wikimedia.org/w/index.php?curid=759647
|
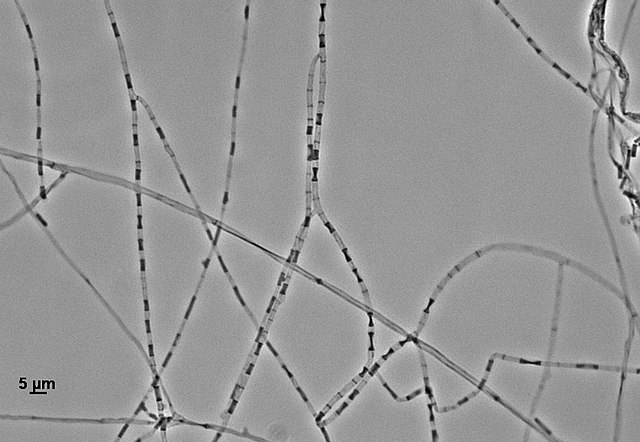
https://upload.wikimedia.org/wikipedia/commons/thumb/1/1d/10244_sc_36d_PH_arthroconidia.jpg/640px-10244_sc_36d_PH_arthroconidia.jpg
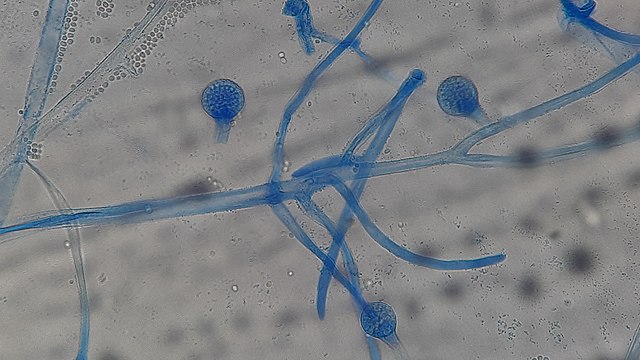
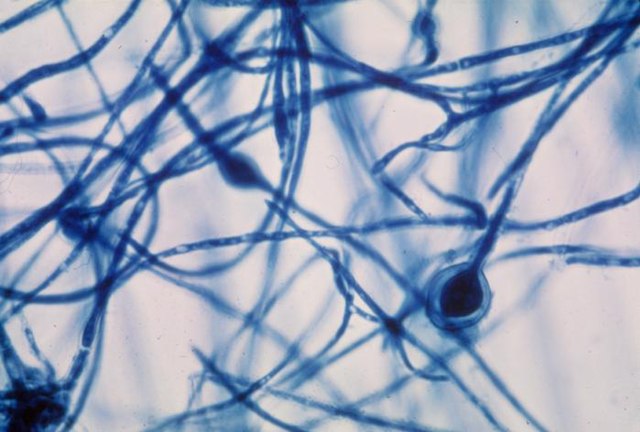
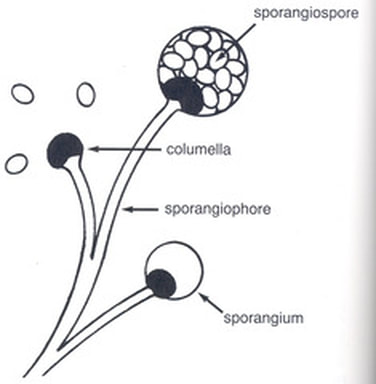
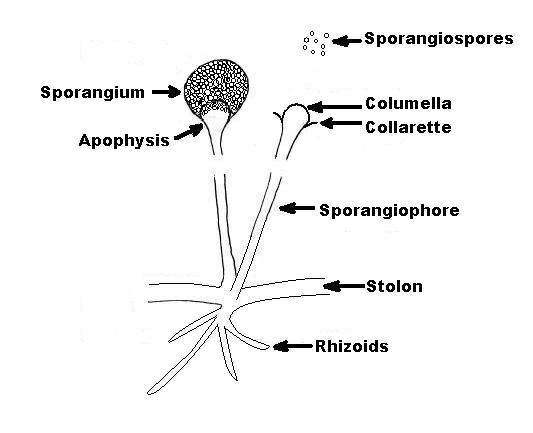
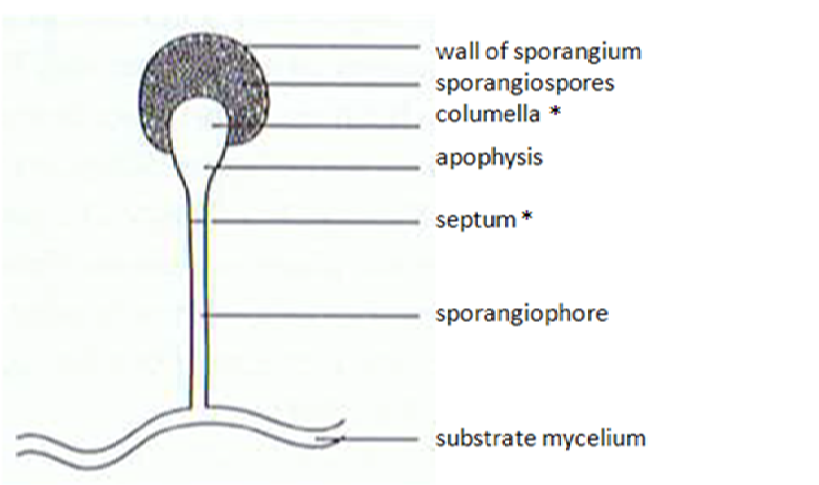
Sporangiospores are formed in aseptate fungi and are considered separate from conidia, which only form in septate fungi. Sporangiospores develop inside a specialized sac called a sporangium/sporangia, which is supported by a base (columnella) supported by a stalk (sporangiophore).
Brand new sporangia may be empty because sporangiospores may not have formed yet. Older sporangia are filled with sporangiospores. Once the sporangium dissipates, dissolves or is damaged, its contents are released and the spores are dispersed into the surrounding environment, but the columnella remains. Sporangiospores are only seen in the phylum Zygomycota.
Brand new sporangia may be empty because sporangiospores may not have formed yet. Older sporangia are filled with sporangiospores. Once the sporangium dissipates, dissolves or is damaged, its contents are released and the spores are dispersed into the surrounding environment, but the columnella remains. Sporangiospores are only seen in the phylum Zygomycota.
|
Public Domain, https://commons.wikimedia.org/w/index.php?curid=1454395
|
By Muslihfsu - Own work, CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=25465499
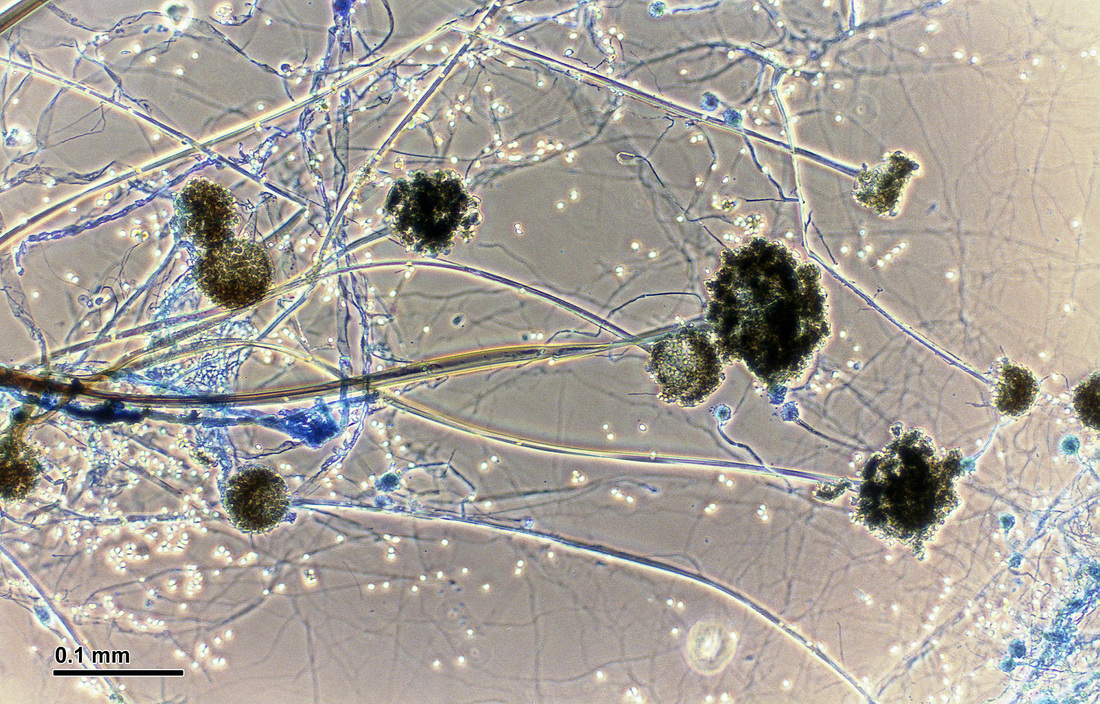
Mucor spp,By Doc. RNDr. Josef Reischig, CSc. - Author's archive, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=31556385
|

Rhizopus spp,By Curtis Clark - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=19865605
|

By Moon Jin Kim, M.D., Pil-Whan Park, M.D., Jeong-Yeal Ahn, M.D., Kyung-Hee Kim, M.D., Ja Young Seo, M.D., Ji-Hun Jeong, M.D., Mi-Jung Park, M.D., Jin-Woo Jung, M.D., Yiel-Hea Seo, M.D. [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons

Absidia spp,https://upload.wikimedia.org/wikipedia/commons/f/f7/Absidia_corymbifera.jpg
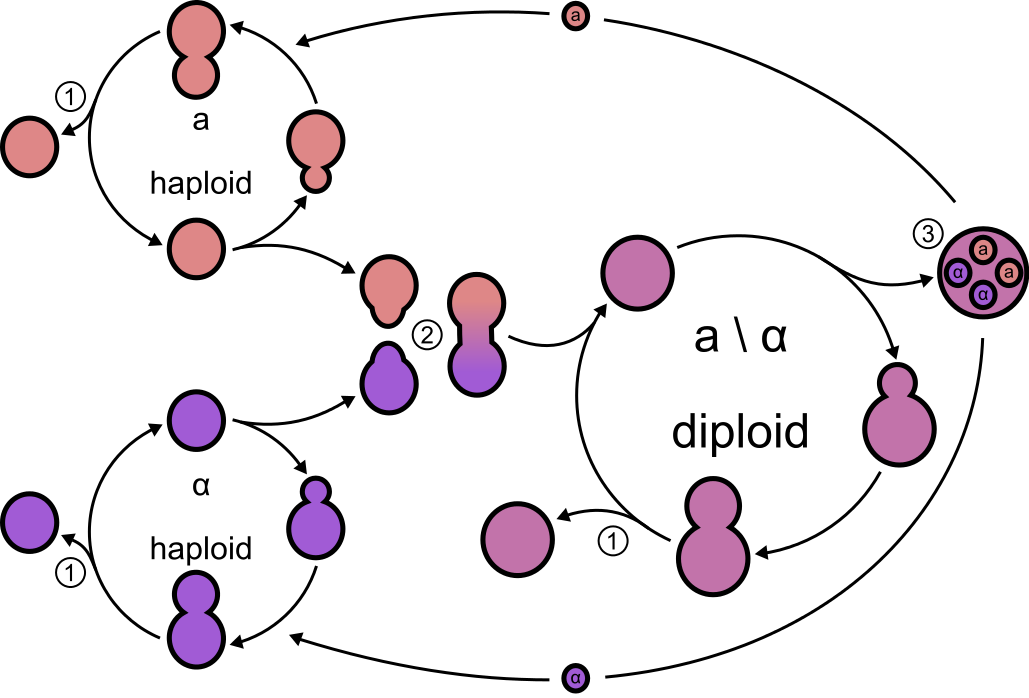
Sexual Reproduction:
Fungi that have a teleomorph or sexual stage are referred to as Perfect Fungi. Those that do not have a teleomorph or sexual stage are referred to as Imperfect Fungi and are referred to as anamorphs .
Ascospores are formed when an antheridium (a nucleus from a male cell) passes through a bridge into the ascogonium (female cell). Either the male and female cells may exist from the same colony or they may be from two different colonies. Once the male and female nuclei mate and fuse and form a zygote, the cell is then referred to as an ascus/asci. The zygote is diploid and it divides via meisois (sexual reproduction), forming 4 haploid nuclei. Those 4 nuclei then divide by mitosis to form 8 nuclei, etc...Finally, each nucleus becomes walled off and forms an ascospore. Sometimes ascospores are protected within a sac-like structure called an ascocarp (ascus). In clinically important/relevant fungi, the ascocarp is actually totally enclosed by a structure known as a cleistothecium. An example of this is the mold Pseudallescheria boydii. Some ascomycetous fungi, such as the yeast Saccharomyces cerevisiae, contain unprotected, unwalled asci.
Fungi that have a teleomorph or sexual stage are referred to as Perfect Fungi. Those that do not have a teleomorph or sexual stage are referred to as Imperfect Fungi and are referred to as anamorphs .
Ascospores are formed when an antheridium (a nucleus from a male cell) passes through a bridge into the ascogonium (female cell). Either the male and female cells may exist from the same colony or they may be from two different colonies. Once the male and female nuclei mate and fuse and form a zygote, the cell is then referred to as an ascus/asci. The zygote is diploid and it divides via meisois (sexual reproduction), forming 4 haploid nuclei. Those 4 nuclei then divide by mitosis to form 8 nuclei, etc...Finally, each nucleus becomes walled off and forms an ascospore. Sometimes ascospores are protected within a sac-like structure called an ascocarp (ascus). In clinically important/relevant fungi, the ascocarp is actually totally enclosed by a structure known as a cleistothecium. An example of this is the mold Pseudallescheria boydii. Some ascomycetous fungi, such as the yeast Saccharomyces cerevisiae, contain unprotected, unwalled asci.

A Cleistothecium; https://upload.wikimedia.org/wikipedia/commons/thumb/2/20/Uncinula_%28Oidium%29_cleistothecium_40X_%282%29.png/640px-Uncinula_%28Oidium%29_cleistothecium_40X_%282%29.png
|
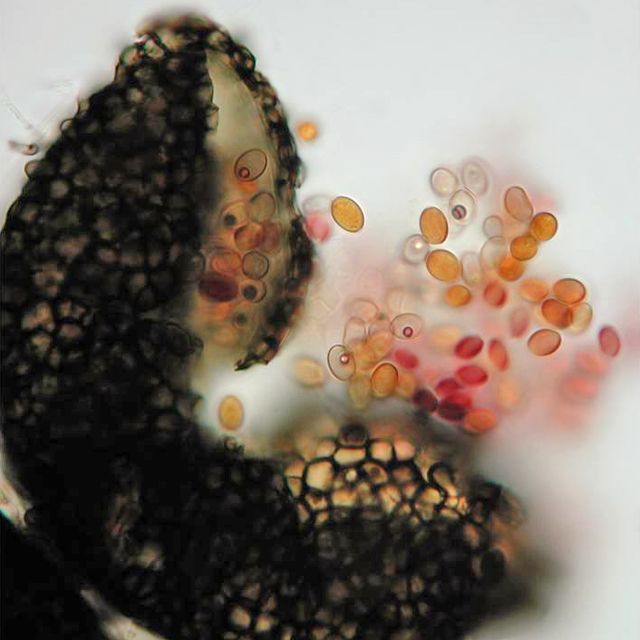
Pseudallescheria boydii (this is the sexual reproductive fruiting body of the Scedosporium apiospermum spp); https://upload.wikimedia.org/wikipedia/commons/thumb/e/ea/Pseudallescheria_boydii.jpg/640px-Pseudallescheria_boydii.jpg
|
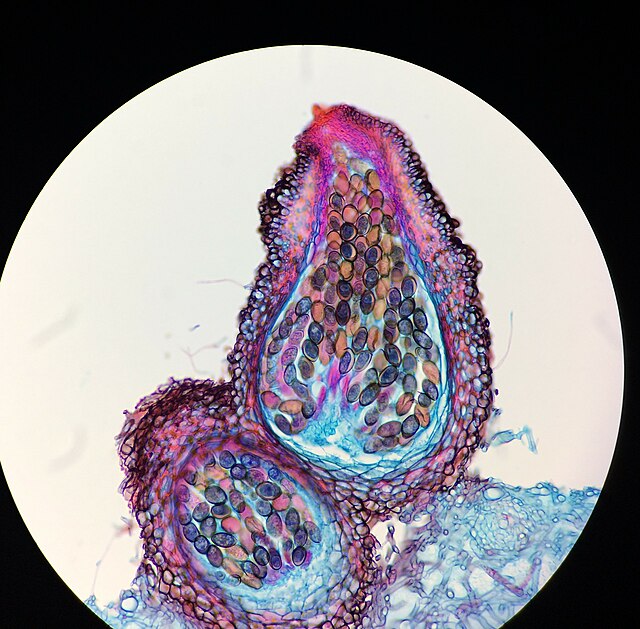
Ascocarps with ascospores; https://upload.wikimedia.org/wikipedia/commons/thumb/0/0c/Sordaria.jpg/640px-Sordaria.jpg
Basidiospores are unique structures that form at the terminal end of a basidium. A binucleate (containing 2 nuclei) mycelium (stalk) is formed when 2 compatible hyphae or yeast cells fuse together with a clamp connection.
The bulb-shaped terminal end of the mycelium becomes a club-shaped structure called the basidium. Inside the basidium lies 2 nuclei that join together to form a zygote, which undergoes meiosis and produces 4 haploid nuclei. This results in the protrusion of 4 small basiospores on the bulb-shaped end of the basidium (denticles). There is one single important Basidiomycete that is of medical importance, and that is Filobasidiella neoformans, which is the sexual stage of Cryptococcus neoformans.
The bulb-shaped terminal end of the mycelium becomes a club-shaped structure called the basidium. Inside the basidium lies 2 nuclei that join together to form a zygote, which undergoes meiosis and produces 4 haploid nuclei. This results in the protrusion of 4 small basiospores on the bulb-shaped end of the basidium (denticles). There is one single important Basidiomycete that is of medical importance, and that is Filobasidiella neoformans, which is the sexual stage of Cryptococcus neoformans.
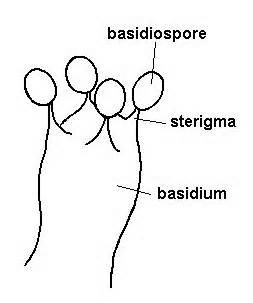
|
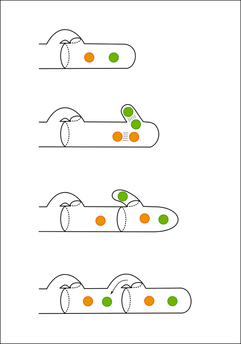
Clamp connections
|
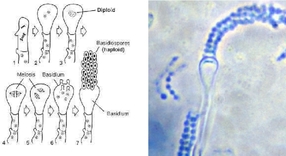
Filobasidiella neoformans, the sexual stage of Cryptococcus neoformans
|

Filobasidiella neformans, the sexual stage of Cryptococcus neoformans
|

Cryptococcus neoformans
|
Zygospores are structures that are formed when two compatible hyphae each form a supportive "arm" called a zygophore, reaching out toward the other, which meet and join to form a zygosporangium, a thick-wallled protective structure in which a zygospore develops.
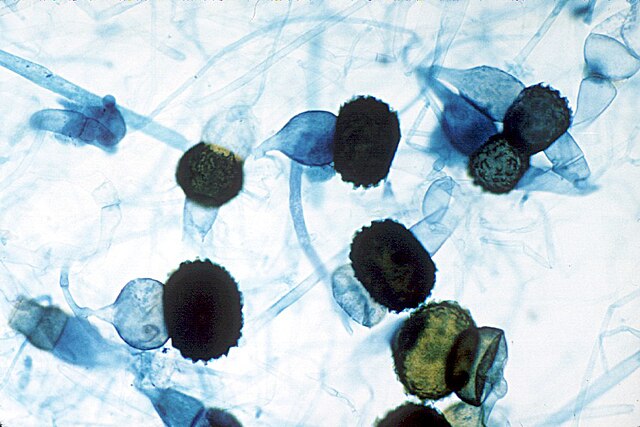
Fusion of 2 zygophores within which a zygospore develops; https://upload.wikimedia.org/wikipedia/commons/thumb/5/5e/Rhizopus_zygospores2.jpg/640px-Rhizopus_zygospores2.jpg
fungal colony descriptions:
|
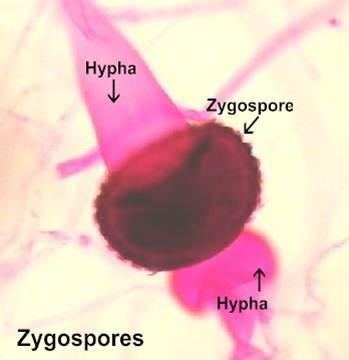
Zygorhynchus
|
Colony Textures and morphology/topography:

Cottony Texture (A. niger)
|

Velvety Texture (Left) (A. nidulans), Woolly Texture (Right) (Rhizopus Mucor)
|

Powdery Texture (T. mentagrophytes)
|
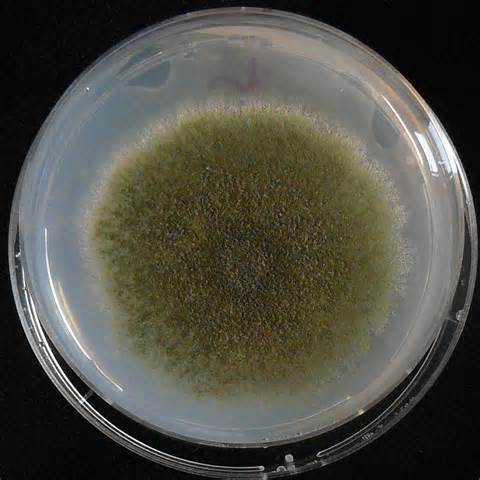
Granular Texture (A. nidulans)
|
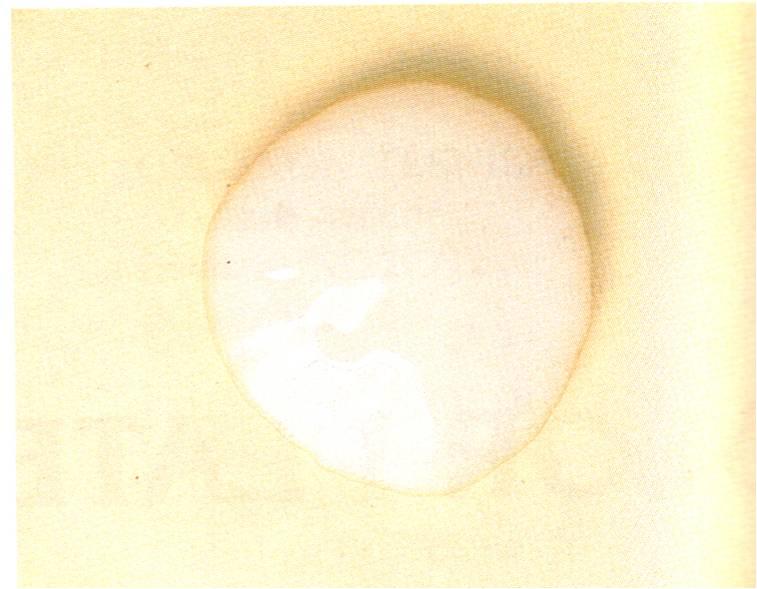
Glabrous/Waxy Texture (most yeasts have this texture on SAB Agar) (C. albicans)
|

Buttery/Creamy/Wrinkled/Leathery Texture (Yeast Form of S. schenckii)
|
MORPHOLOGY AND PIGMENTATION:
COLONY TEXTURE:
Colony texture basically describes the height of the aerial hyphae (what you can see above the surface of the agar). This is what makes molds appear "fuzzy". Colonies may be described as the following:
Cottony/Woolly/Fluffy/Hairy (Looks like Cotton Candy or Sheep's Wool)
- Velvety/Suede-like (Looks Soft Like Velvet or Velour): short aerial hyphae
- Powdery (Soft Like Flour or Talcum Powder)
- Granular/Sugary (Gritty, Course, Like Sand or Sugar); may contain granules
- Glabrous/Waxy (Smooth and/or Shiny or Matte, Leathery, Wax-Like Texture, Creamy, Moist, Buttery)
- Dry/Wrinkled/Lacy
Cottony/Woolly-This describes colonies with very high, dense aerial mycelium that appear like sheep's wool, "fluffy", "cottony", "cotton-candy-like". Colonies are fluffy, and sometimes quickly fill the plate if they are rapid growers.
Velvety-This describes colonies whose aerial hyphae are lower and resemble velvet or velour fabrics.
Granular/Sugary-This describes colonies that are grainy like granulated sugar or powder, and whose aerial hyphae are flat, dry, rough, crumbly, or flour-like. Sometimes these colonies contain granules.
Glabrous/Waxy-This describes colonies that are shiny and wax-like, mucoid, with a smooth surface. No aerial hyphae are observed. Yeasts typically fall into this category. They are moist, creamy, buttery, and some have a "bread-like" odor.
COLONY MORPHOLOGY:
Colony morphology includes the topagraphy or structure and shape of the fungal colonies on the agar surface and reverse, as well as the color of the colonies. It is best to be as specific as possible when describing colonies.
- Colony Topography: Rugose, Verrucose, Umbonate (like a button/snap), Flat, Heaped, Folded, Striated, Wrinkled, Lacy
- Color: Be Specific (Brown, Black, Light Green, Olive Green, Dark Green, Pink, White, Cream, Off-White, Beige, Tan, Yellow, Green With White Fringe, Reddish, Red-Brown, Black and White, Red, Gray, Dark Gray)
- Note any diffusion of pigment into the agar and its color
- Note the color of the reverse as well when needed for specificity
- Surface: top of agar
- Reverse: bottom/underside of agar
This describes colonies that are wrinkled or folded in appearance and striated. They resemble a volcano or mountain with a peak in the middle and "valleys" (furrows).
Verrucose Colonies:
This describes colonies that are mountainous, wrinkled or convoluted in appearance and striated. They sometimes resemble warts.
Umbonate Colonies:
This describes colonies that come to a peak or slight point/elevation in the middle and are button-like (heaped). There may also be deep rugose furrows surrounding the button as well.
COLORS:
Colors may be described as the following: brown, beige, tan, khaki, cream, off-white, mahogany, cinnamon, deep red, pink, olive green, grass green, light gray, dark gray, black, white, salt-and-pepper, light yellow, deep yellow, orange, pink, lavender, salmon.
Also, describe borders (white border, "frilly", apron, rough edges, spreading, "feet"), and if the colony is easily moved across the agar, pits the agar, is mucoid, etc...
Taxonomy:
Taxonomy is classification. Fungi are classified by their sexual (teleomorph) stage, but if they have no known sexual (teleomorph) stage, they are classified under the phylum Deuteromycota and represent the asexual (anamorph) stage.
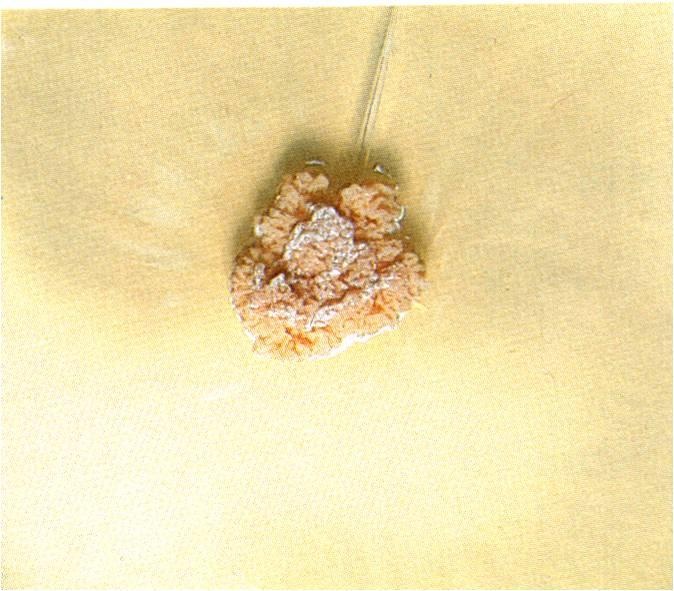
This would be described as verrucose
|
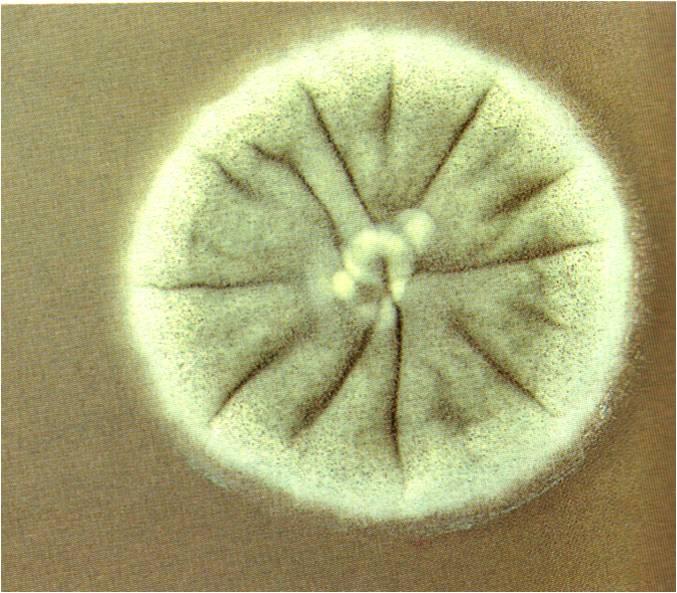
This would be described as rugose and umbonate, wrinkled, heaped, striated, because it is like a mountain with a heaped and button-like center
|

This would be described as rugose
|
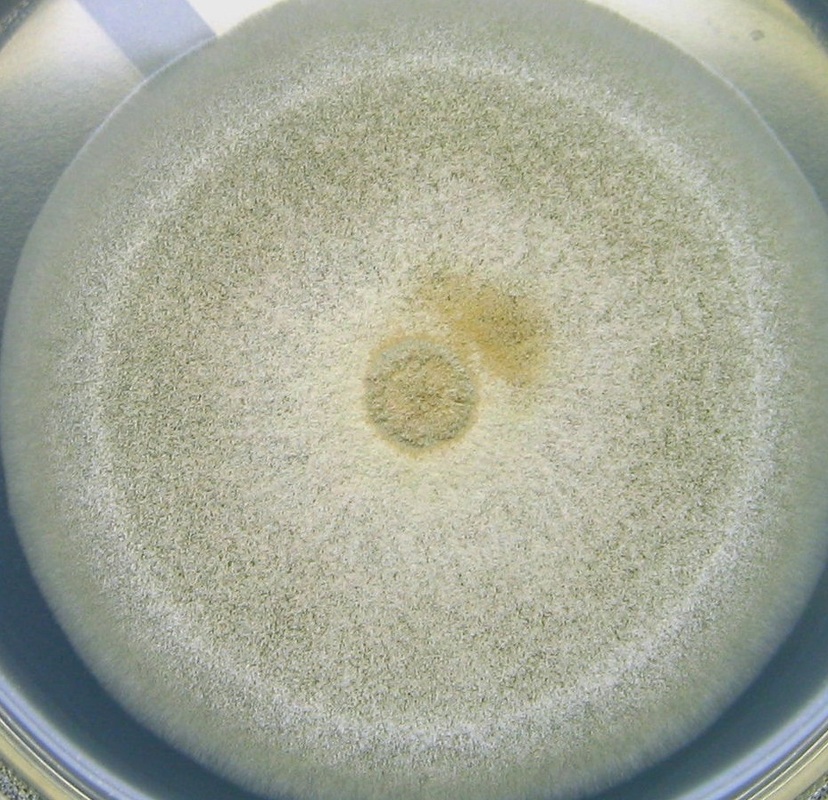
This would be described as flat and umbonate
|
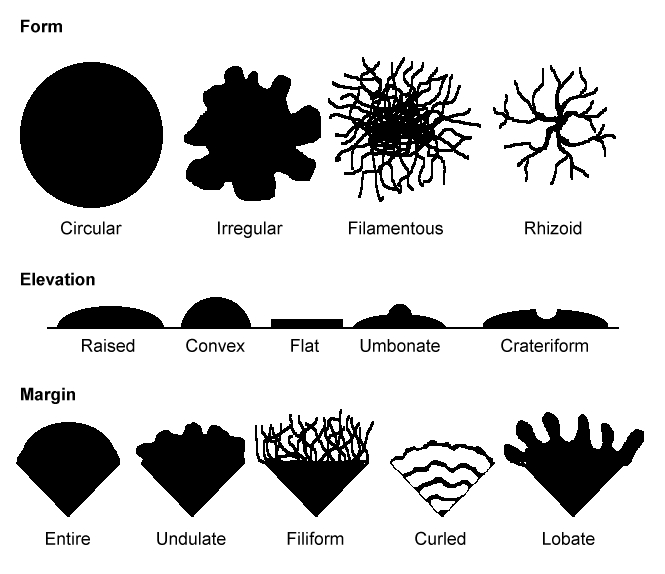
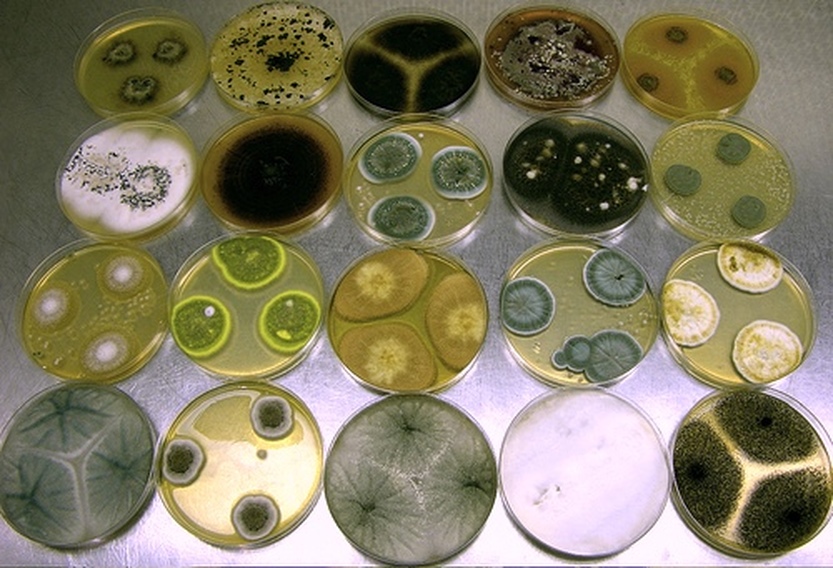
Various Aspergillus and Penicillium colonies displaying a variety of textures, colors and topographies.
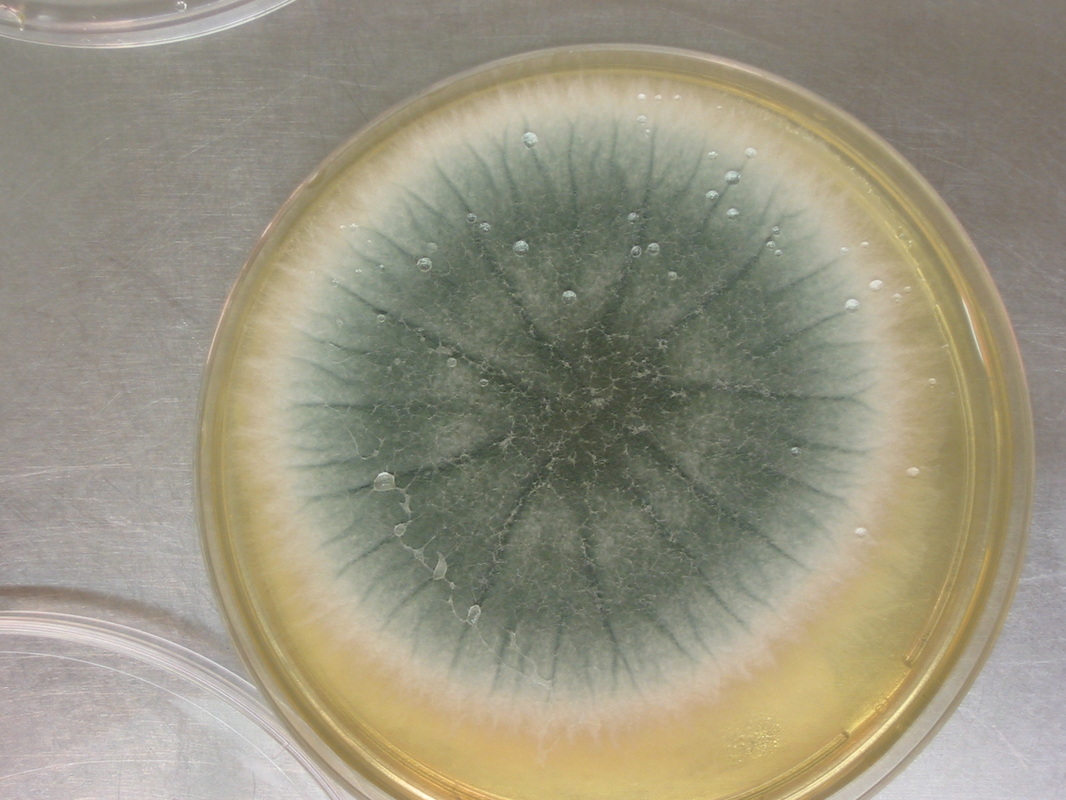
Aspergillus: Velvety, olive green, rugose colonies with toxin production (see the droplets forming at the top of the aerial hyphae)
|
Fusarium: Velvety, light pink and white umbonate colony with a deep yellow center
|

Aspergillus nidulans: Cottony/Woolly, white colony with "salt-and-pepper" appearance, umbonate with a deep yellow/light gray button
|
mycoses (fungal illnesses/diseases)
Mycoses are classified according to the body sites and/or tissues that are invaded by specific types of fungi.
Superficial Mycoses:
Superficial Mycoses are those that affect just the outer layer of the 5 layers of skin and hair (epidermis only). These include the following: otomycosis (fungal ear infections), black and white piedra (hair), pityriasis versicolor and tinea nigra (both affect skin pigmentation). Superficial mycoses are spread person-to-person via direct or indirect contact by fomates (towels, linens, socks, brushes/combs, showers in the gym, gym equipment, saunas, whirlpools, nail clippers, hair clippers, nail salon foot baths, etc...).
Cutaneous Mycoses:
The cutaneous mycoses actually cause destruction of the keratin layers of the skin, hair and nails (epidermis and dermis). Rarely, they spread to invade deeper tissues. These are caused mostly by the Dermatophytes, such as Microsporum, Trichophyton, Epidermophyton, Candida spp. These are spread the same way as superficial mycoses most of the time, but can also be caused by one's own microflora overgrowth (yeasts).
Subcutaneous Mycoses:
The subcutaneous mycoses go a little deeper and invade the skin, fascia, muscle and connective tissue just below the skin (hypodermis). Rarely, they invade deeper tissues. Included are chromoblastomycosis, sporotrichosis, and mycetoma. These are often caused by traumatic inoculation (thorns, stickers, etc...) with the fungus.
Systemic Mycoses:
Systemic mycoses invade the deeper tissues and spread throughout the body and bloodstream into the organs of the body, such as the liver, lungs, and brain. If the disease is disseminated, then the other areas may be involved as well (cutaneous, subcutaneous). These include more serious diseases such as histoplasmosis, blastomycosis, coccidioidomycosis, and paracoccidioidomycosis. These typically affect patients who have underlying illnesses or who are immunocompromised or immunosuppressed.
Superficial Mycoses:
Superficial Mycoses are those that affect just the outer layer of the 5 layers of skin and hair (epidermis only). These include the following: otomycosis (fungal ear infections), black and white piedra (hair), pityriasis versicolor and tinea nigra (both affect skin pigmentation). Superficial mycoses are spread person-to-person via direct or indirect contact by fomates (towels, linens, socks, brushes/combs, showers in the gym, gym equipment, saunas, whirlpools, nail clippers, hair clippers, nail salon foot baths, etc...).
Cutaneous Mycoses:
The cutaneous mycoses actually cause destruction of the keratin layers of the skin, hair and nails (epidermis and dermis). Rarely, they spread to invade deeper tissues. These are caused mostly by the Dermatophytes, such as Microsporum, Trichophyton, Epidermophyton, Candida spp. These are spread the same way as superficial mycoses most of the time, but can also be caused by one's own microflora overgrowth (yeasts).
Subcutaneous Mycoses:
The subcutaneous mycoses go a little deeper and invade the skin, fascia, muscle and connective tissue just below the skin (hypodermis). Rarely, they invade deeper tissues. Included are chromoblastomycosis, sporotrichosis, and mycetoma. These are often caused by traumatic inoculation (thorns, stickers, etc...) with the fungus.
Systemic Mycoses:
Systemic mycoses invade the deeper tissues and spread throughout the body and bloodstream into the organs of the body, such as the liver, lungs, and brain. If the disease is disseminated, then the other areas may be involved as well (cutaneous, subcutaneous). These include more serious diseases such as histoplasmosis, blastomycosis, coccidioidomycosis, and paracoccidioidomycosis. These typically affect patients who have underlying illnesses or who are immunocompromised or immunosuppressed.
the layers of skin: epidermis (superficial), dermis (deep), hypodermis/subcutaneous tissue (very deep, systemic if it gets into the bloodstream and travels)
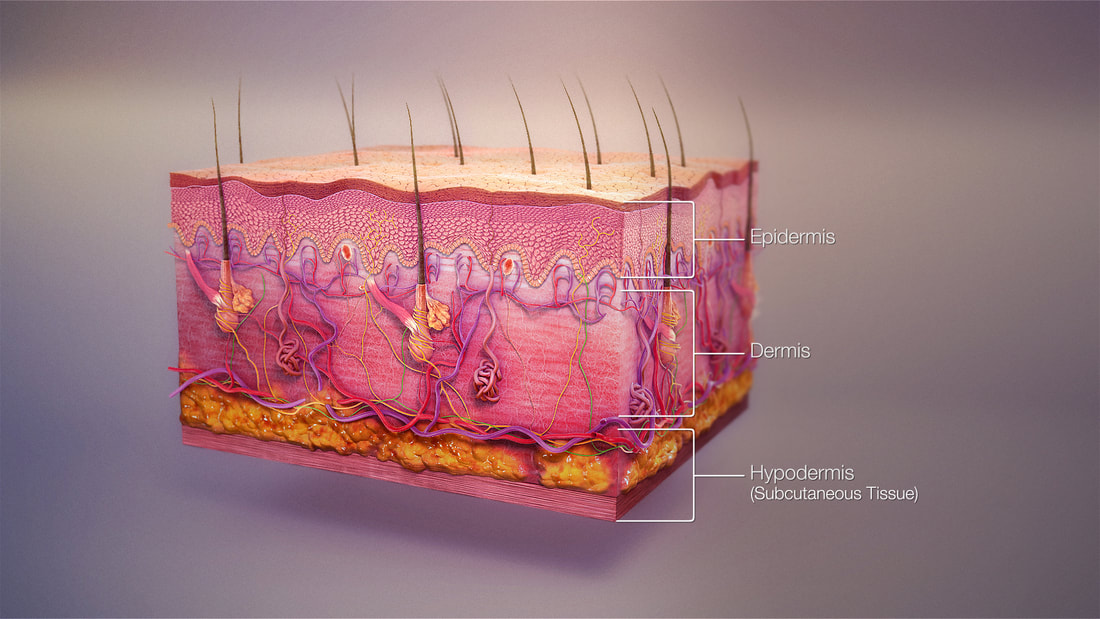
https://upload.wikimedia.org/wikipedia/commons/thumb/f/f0/3D_medical_animation_skin_layers.jpg/640px-3D_medical_animation_skin_layers.jpg
the sublayers of epidermis (top layer of skin):
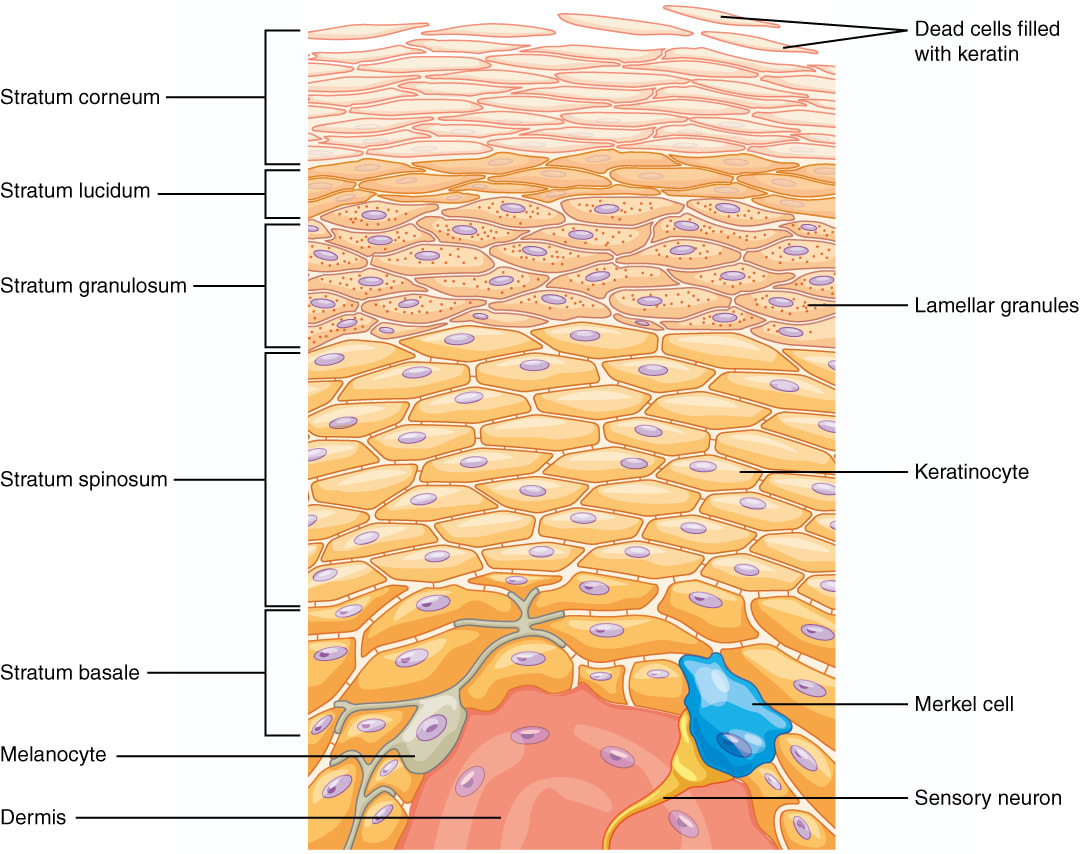
https://upload.wikimedia.org/wikipedia/commons/thumb/f/f9/502_Layers_of_epidermis.jpg/640px-502_Layers_of_epidermis.jpg
Mycology Laboratory procedures:
SPECIMEN COLLECTION AND PROCESSING:
In mycology, it is important to make sure that the specimen is collected from the area that is most likely to be affected, make sure that the amount is adequate and delivered to the laboratory promptly, that it is quickly processed, that it is properly labelled, and that the mycologist utilizes strict aseptic and sterile technique when handling these types of specimens, being careful not to contaminate the environment or themselves.
Specimens that may be sent for analyzation may include blood and bone marrow, skin, hair, nails, corneal scrapings, cerebrospinal fluid (CSF), bronchial washings, sputum, transtracheal aspirates, throat cultures, lavage, tissue, biopsies, urine, vaginal, cervix or urethral discharges, and deep or superficial wound specimens.
In mycology, each specimen is to be examined microscopically before and/or concurrently with culturing. Special media may be inoculated to isolate and specifically identify an organism. Direct examination may save a patient's life through early and accurate detection and treatment. Some pathogenic fungi require a long incubation period (3-4 weeks) for growth. At the same time, if a fungi is not seen on a direct wet mount, the doctor can avoid administering antifungal drugs, which are often potent and have side effects, some potentially toxic and require long treatment. Mycology practices require that you be extremely careful and very thorough with the direct examination and multiple types of wet mounts may be required.
WORKUPS (Means we need to do something with the culture to rule out a pathogenic fungi or infection or determine if it needs to be further identified, sent out for identification and/or susceptibility testing, or discarded as a contaminant)
MICROSCOPE/SLIDE TECHNIQUES:
Saline Wet Mount:
A saline wet mount may be performed to look for budding yeasts, fungal elements (hyphae, pseudohyphae, conidia), or fungus-like bacteria (thin, branching filaments). This involves placing a drop of specimen on a glass slide with the addition of a drop of saline, placing a coverslip on it, and viewing the specimen under both low and high power using low light or phase contrast microscopy. This can be accomplished by lowering the condenser.
In mycology, it is important to make sure that the specimen is collected from the area that is most likely to be affected, make sure that the amount is adequate and delivered to the laboratory promptly, that it is quickly processed, that it is properly labelled, and that the mycologist utilizes strict aseptic and sterile technique when handling these types of specimens, being careful not to contaminate the environment or themselves.
Specimens that may be sent for analyzation may include blood and bone marrow, skin, hair, nails, corneal scrapings, cerebrospinal fluid (CSF), bronchial washings, sputum, transtracheal aspirates, throat cultures, lavage, tissue, biopsies, urine, vaginal, cervix or urethral discharges, and deep or superficial wound specimens.
In mycology, each specimen is to be examined microscopically before and/or concurrently with culturing. Special media may be inoculated to isolate and specifically identify an organism. Direct examination may save a patient's life through early and accurate detection and treatment. Some pathogenic fungi require a long incubation period (3-4 weeks) for growth. At the same time, if a fungi is not seen on a direct wet mount, the doctor can avoid administering antifungal drugs, which are often potent and have side effects, some potentially toxic and require long treatment. Mycology practices require that you be extremely careful and very thorough with the direct examination and multiple types of wet mounts may be required.
WORKUPS (Means we need to do something with the culture to rule out a pathogenic fungi or infection or determine if it needs to be further identified, sent out for identification and/or susceptibility testing, or discarded as a contaminant)
MICROSCOPE/SLIDE TECHNIQUES:
Saline Wet Mount:
A saline wet mount may be performed to look for budding yeasts, fungal elements (hyphae, pseudohyphae, conidia), or fungus-like bacteria (thin, branching filaments). This involves placing a drop of specimen on a glass slide with the addition of a drop of saline, placing a coverslip on it, and viewing the specimen under both low and high power using low light or phase contrast microscopy. This can be accomplished by lowering the condenser.
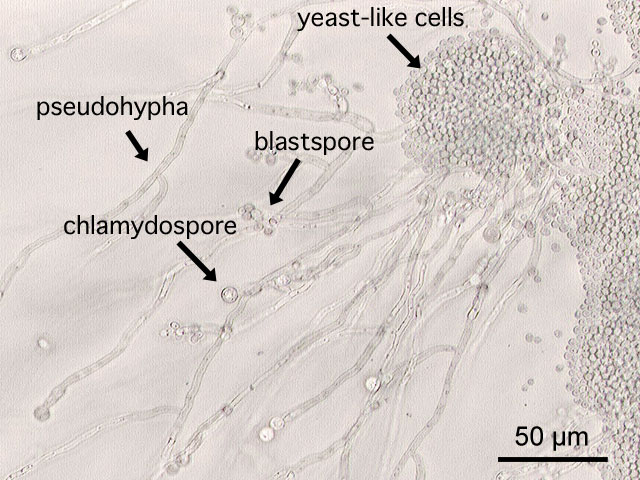
Candida albicans structures seen on a saline wet mount
Lactophenol Cotton Blue:
Instead of a saline wet mount, a lactophenol cotton blue wet mount (LPCB) may be performed. The same structures can be observed, but the cotton blue will stain the chitin in the fungal cell walls, enabling them to stand out more, and the phenol in the stain will kill any fungal organisms. This can be accomplished by placing a drop of stain on a clean glass slide and a touch prep with Scotch tape to the specimen then placing the tape on the slide over the drop of LPCB. Add another drop of LPCB then a cover slip, and observe under low and high power. To make the slide permanent, you can rim the cover slip with permamount or clear fingernail polish and let it dry. Lactic acid serves as a clearing agent that aids in clearing cellular debris, phenol kills any viable cells, and cotton blue stains the fungal elements so they can be seen clearly under the microscope.
Instead of a saline wet mount, a lactophenol cotton blue wet mount (LPCB) may be performed. The same structures can be observed, but the cotton blue will stain the chitin in the fungal cell walls, enabling them to stand out more, and the phenol in the stain will kill any fungal organisms. This can be accomplished by placing a drop of stain on a clean glass slide and a touch prep with Scotch tape to the specimen then placing the tape on the slide over the drop of LPCB. Add another drop of LPCB then a cover slip, and observe under low and high power. To make the slide permanent, you can rim the cover slip with permamount or clear fingernail polish and let it dry. Lactic acid serves as a clearing agent that aids in clearing cellular debris, phenol kills any viable cells, and cotton blue stains the fungal elements so they can be seen clearly under the microscope.
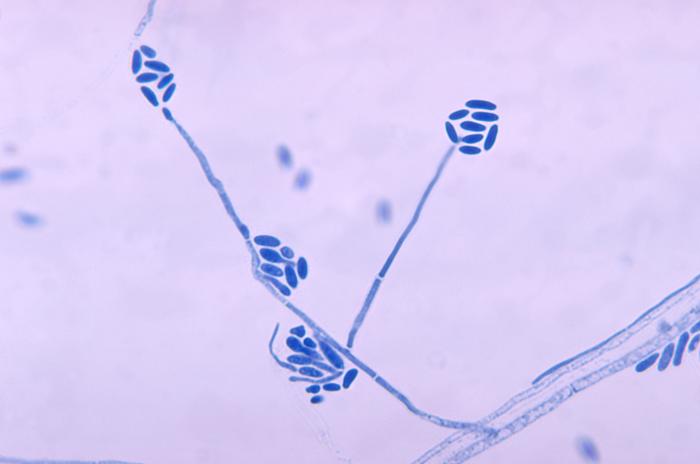
Acremonium spp stained with LPCB and observed under high power
Potassium Hydroxide (KOH) Preparation:
If you receive a skin, hair or nail specimen, KOH preparation aids in dissolving the background cellular debris, leaving only fungal elements to be observed. Potassium hydroxide dissolves keratin in these specimens so any fungal elements will become more visible. This slide is not used to quantitate, however, so in addition to this slide, if fungal elements are observed, a saline wet mount should be performed to quantitate epithelial cells and white blood cells and to include the presence of Trichomonas vaginalis in vaginal specimens. This can be accomplished by thinly smearing some specimen on a glass slide. Add one drop of 10% KOH, add a cover slip, and gently heat the specimen by passing it through a flame 2-3x or by setting it on a heat block. Allow the slide to sit for 20 minutes before viewing, to enable the cellular debris to clear. Observe the specimen under both low and high power. If you are observing a hair specimen, look both at the outside of the hair and inside the hair shaft to see what type of invasion, if any, has occurred. Ectothrix invasion means the fungus has invaded the outside of the hair shaft, whereas endothrix invasion means that it has invaded the inside of the hair shaft. Observation under low light or phase contrast microscopy is best.
If you receive a skin, hair or nail specimen, KOH preparation aids in dissolving the background cellular debris, leaving only fungal elements to be observed. Potassium hydroxide dissolves keratin in these specimens so any fungal elements will become more visible. This slide is not used to quantitate, however, so in addition to this slide, if fungal elements are observed, a saline wet mount should be performed to quantitate epithelial cells and white blood cells and to include the presence of Trichomonas vaginalis in vaginal specimens. This can be accomplished by thinly smearing some specimen on a glass slide. Add one drop of 10% KOH, add a cover slip, and gently heat the specimen by passing it through a flame 2-3x or by setting it on a heat block. Allow the slide to sit for 20 minutes before viewing, to enable the cellular debris to clear. Observe the specimen under both low and high power. If you are observing a hair specimen, look both at the outside of the hair and inside the hair shaft to see what type of invasion, if any, has occurred. Ectothrix invasion means the fungus has invaded the outside of the hair shaft, whereas endothrix invasion means that it has invaded the inside of the hair shaft. Observation under low light or phase contrast microscopy is best.
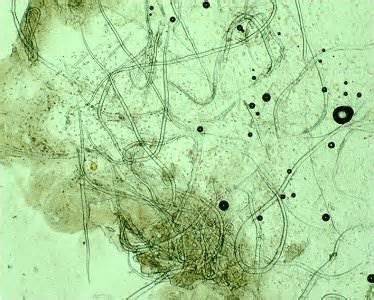
KOH wet mount with fungal hyphae observed
|

KOH Trichogram showing ectothrix invasion of the hair shaft (outside)
|
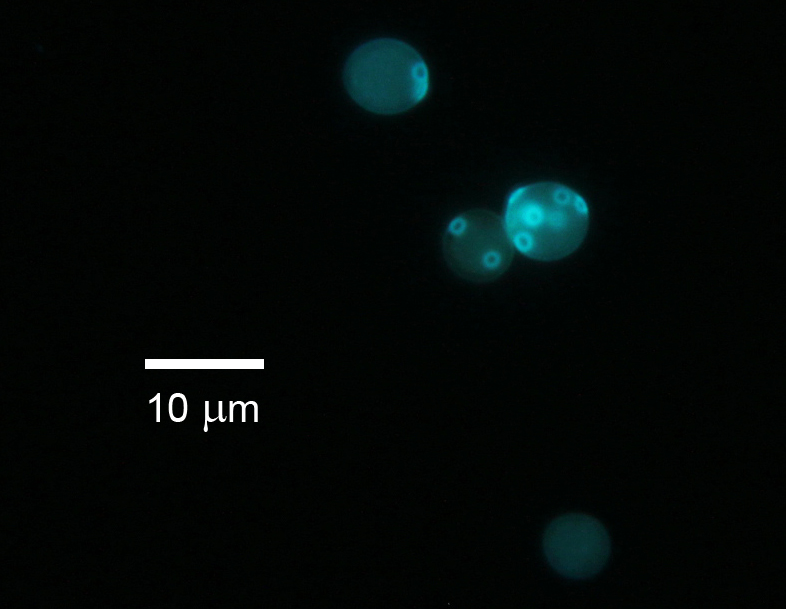
Potassium hydroxide (10%) KOH and calcofluor white stain
|
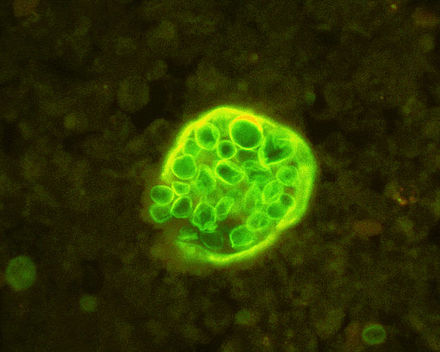
Calcofluor white stain
|
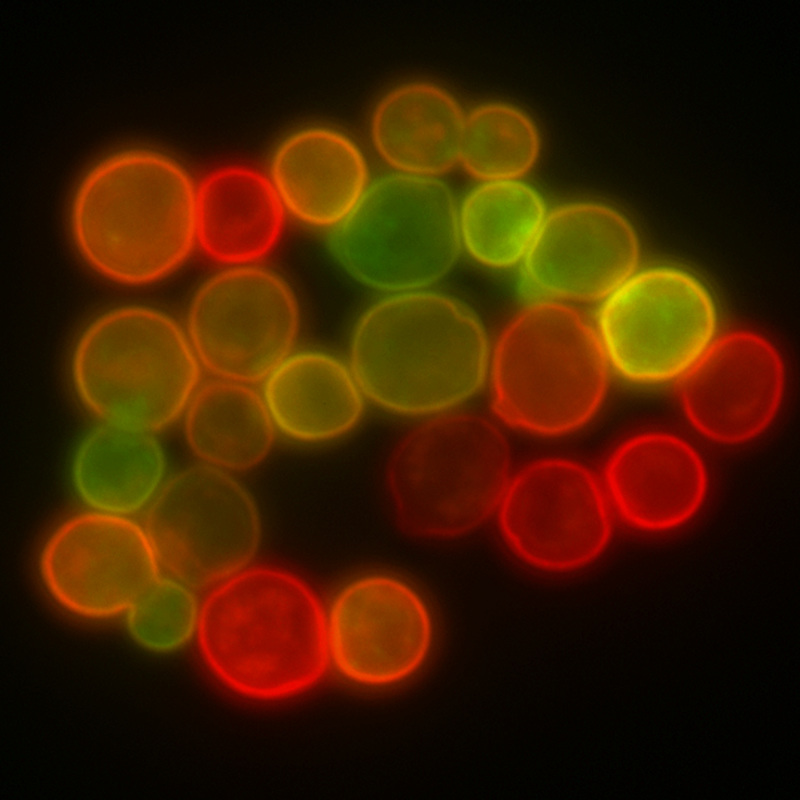
Auramine stain
|
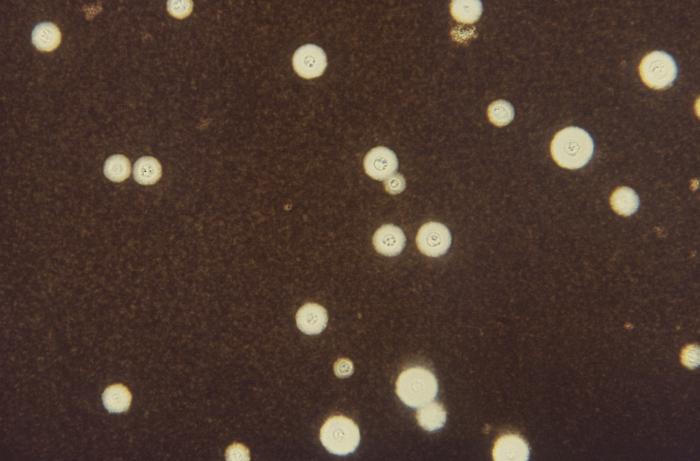
India Ink Stain showing capsules of Cryptococcus neoformans
|
Gram Stain:
A Gram stain may reveal oval-shaped and budding yeast cells and pseudohyphae of the Candida spp or the capsule around Cryptococcus neoformans.
A Gram stain may reveal oval-shaped and budding yeast cells and pseudohyphae of the Candida spp or the capsule around Cryptococcus neoformans.
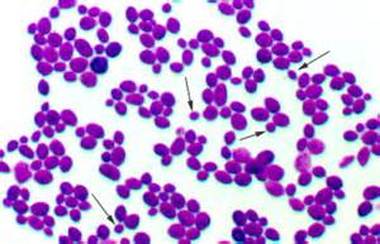
Gram-stained Candida albicans budding yeasts
Kinyoun Modified Acid-Fast Stain:
Nocardia asteroides and Actinomycetes/Actinomycetes are funguslike bacteria that are partially acid-fast and appear red against a blue background. It is important to differentiate these from Mycobacterium spp. See your lab's procedure as this procedure can vary slightly between laboratories.
Nocardia asteroides and Actinomycetes/Actinomycetes are funguslike bacteria that are partially acid-fast and appear red against a blue background. It is important to differentiate these from Mycobacterium spp. See your lab's procedure as this procedure can vary slightly between laboratories.
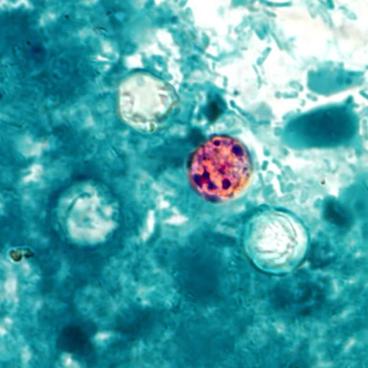
A modified acid-fast stain
|
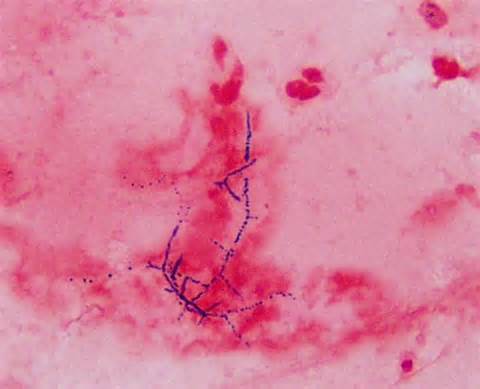
Nocardia asteroides, a fungus-like bacterium that is partially acid-fast
|
India-Ink Preparation:
This procedure is used to look for capsules surrounding yeasts, particularly Cryptococcus neoformans in CSF fluid sediment. Slides are made by mixing a tiny little drop of India Ink or nigrosin with one drop of specimen sediment. Add a cover slip and allow the slide to sit for 10 minutes to allow the yeast cells to settle into one plane of focus. Observe this slide with the condenser fully open and up to allow for maximum amount of light to observe capsules around budding yeasts.
This procedure is used to look for capsules surrounding yeasts, particularly Cryptococcus neoformans in CSF fluid sediment. Slides are made by mixing a tiny little drop of India Ink or nigrosin with one drop of specimen sediment. Add a cover slip and allow the slide to sit for 10 minutes to allow the yeast cells to settle into one plane of focus. Observe this slide with the condenser fully open and up to allow for maximum amount of light to observe capsules around budding yeasts.
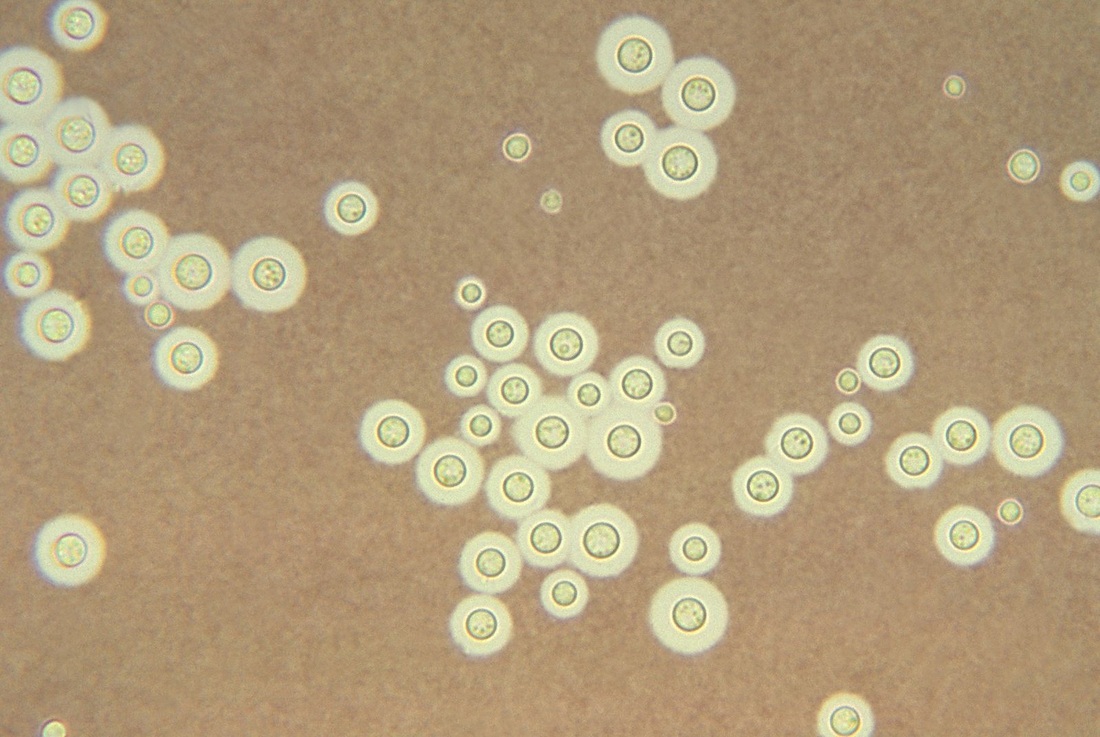
C. neoformans stained with India Ink and the capsules surrounding the yeasts (notice the huge zone of clearing around the cells)
Calcofluor White Stain:
Calcofluor white is actually a bleaching agent used in the paper industry. It is a stain that is taken up into the chitin of the cell wall, producing a chalk-white or apple-green fluorescence under fluorescence microscopy. If observing a nail specimen, calcofluor white may be mixed with 10% KOH just before use in order to dissolve the background material first. Slides are made by adding 1 drop of calcofluor white and 1 drop of 10% KOH on a glass slide. Mix the specimen with the solution, cover slip and examine under the UV (fluorescence) microscope under high power (use filter 2 or 3). Fungal elements will fluoresce.
Calcofluor white is actually a bleaching agent used in the paper industry. It is a stain that is taken up into the chitin of the cell wall, producing a chalk-white or apple-green fluorescence under fluorescence microscopy. If observing a nail specimen, calcofluor white may be mixed with 10% KOH just before use in order to dissolve the background material first. Slides are made by adding 1 drop of calcofluor white and 1 drop of 10% KOH on a glass slide. Mix the specimen with the solution, cover slip and examine under the UV (fluorescence) microscope under high power (use filter 2 or 3). Fungal elements will fluoresce.
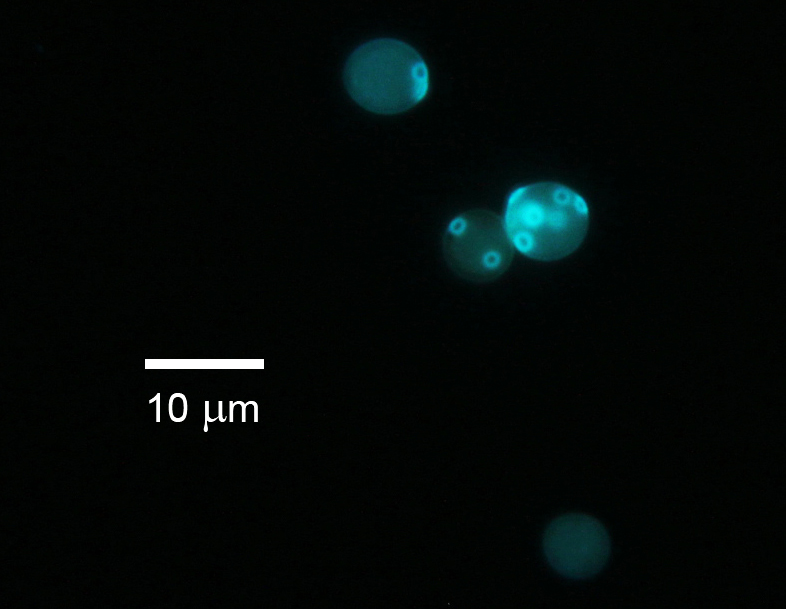
Yeasts fluorescing under UV microscopy after being stained with calcofluor white
OTHER:
Hair Perforation Test:
Hair Perforation Test:
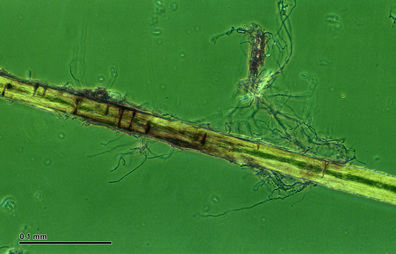
Ectothrix invasion (outside the hair shaft)
|
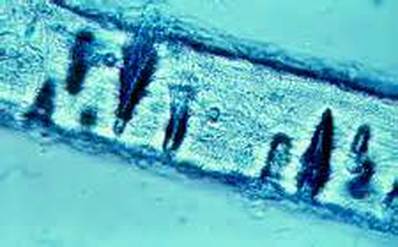
Endothrix invasion (inside the hair shaft)
|
Gomori methenamine silver (GMS) stain:
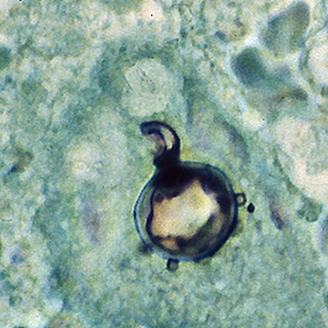
Paracoccidioides brasiliensis stained with GMS stain
|
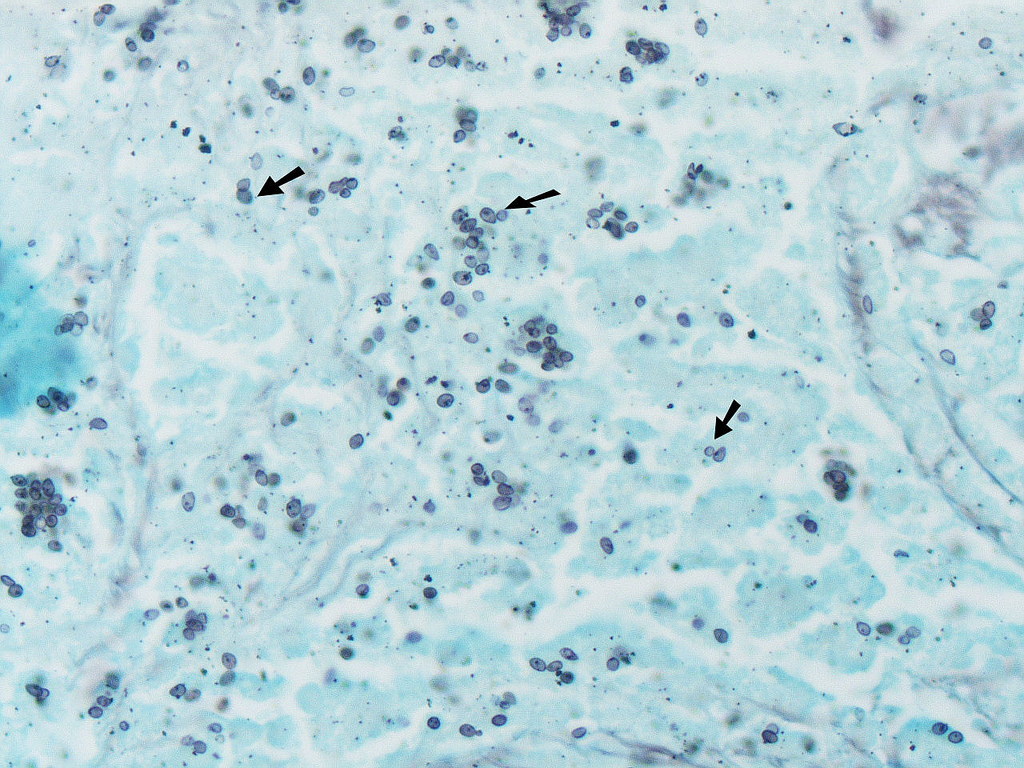
Histoplasma capsulatum stained with GMS stain
|
Periodic Acid-Schiff Stain (PAS):
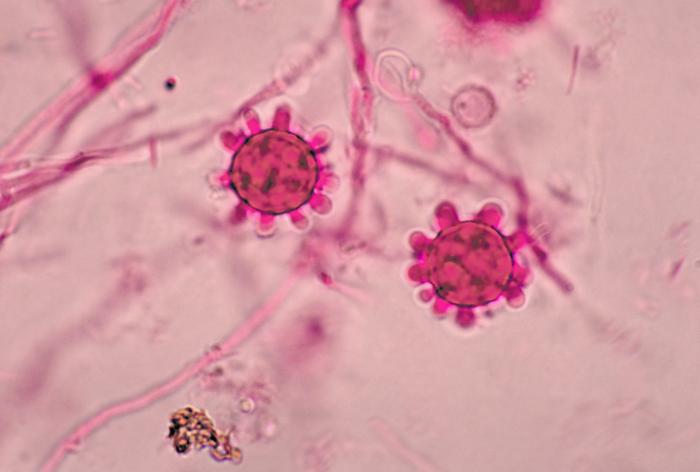
Paracoccidioides in PAS stain
|
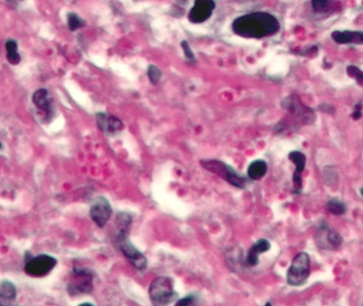
Histoplasma capsulatum in PAS stain
|
Hematoxyin and Eosin Stain (H&E):
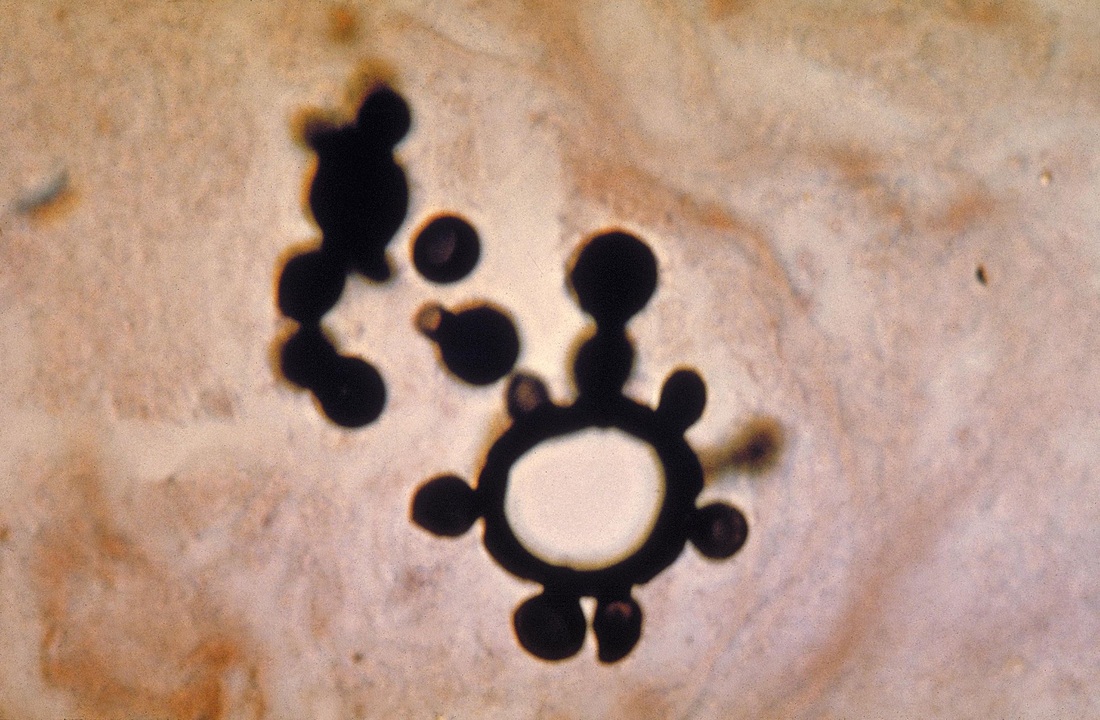
Paracoccidioides in H&E stain
WRIGHT'S STAIN OR GIEMSA STAIN:
Links to videos that show mycology techniques:
Slide Culture: https://www.youtube.com/watch?v=0RJKvTngF5s
Tease Mount: https://www.youtube.com/watch?v=OMIF1Elr9i4
Scotch Tape Prep/Lactophenol Cotton Blue: https://www.youtube.com/watch?v=ktENJEkopXI
Tease Mount: https://www.youtube.com/watch?v=OMIF1Elr9i4
Scotch Tape Prep/Lactophenol Cotton Blue: https://www.youtube.com/watch?v=ktENJEkopXI
primary fungal media:
In addition to direct examination via direct wet mount, specific fungal media are used to plate and culture and isolate fungal organisms. Tubed media are ideal because they stay moist longer and they do not dry out during long incubation periods. They also save space and you can store more of them side-by-side in racks. This is a safer method for the mycologist, as fungal reproductive elements are less likely to become airborne and contaminate the laboratory and its workers. ALWAYS use tubed media when Coccidioides immitis is suspected because this fungus is extremely infectious and if aerosols are produced, they may become inhaled, causing infection.
It is crucial that the mycologist always work under a biological hood to prevent contamination, always wear a lab coat, gloves and mask, autoclave specimens and inoculated media upon finishing or completing work with the specimen, and disinfect the work area daily or multiple times throughout the work day.
NONSELECTIVE MEDIA:
Sabouraud Brain Heart Infusion Agar (SABHI)-This is often the medium of choice for initial isolation because it is richer in nutrients than Sabouraud Dextrose Agar (SDA) and supports the growth of a wider variety of fungi. It allows bacteria, the fungal opportunists, yeasts, dermatophytes, subcutaneous pathogens, and most systemic pathogens to grow, however, some of the fastidious organisms like H. capsulatum or B. dermatiditis will not grow on this media.
This media is stored in the refrigerator and must be brought to room temperature prior to inoculation. Swab the whole surface of the agar slant and push the specimen lightly into the agar. Because agar contains no antibiotics, inoculate this one first before inoculating media containing antibiotics to prevent carryover. Loosen the cap and incubate at 30 degrees Celsius for up to 1 month before discarding it and concluding that it is negative for growth.
Brain Heart Infusion Agar With Blood (BHIB):
This media is richer in nutrients than SABHI. It is used to inoculate specimens from normally sterile sites or for suspect anaerobic actinomycetes.
Sabouraud Dextrose Agar (SDA):
This media is not nutritionally rich, and has an acid pH of 5.6. This media inhibits the growth of many bacteria. Fungal opportunists and pathogenic fungi grow well, however, all with the exception of H. capsulatum and many strains of N. asteroides. The media should be treated exactly like SABHI agar. This is a great, nonspecific agar used to grow a variety of fungi.
*If Nocardia is suspected, then paraffin may be added to the nonselective fungal medium to block the overgrowth of bacteria and to enhance the growth of Nocardia.
SELECTIVE MEDIA WITH ANTIBIOTICS:
Inhibitory Mold Agar (IMA):
This media contains gentamicin and sometimes chloramphenicol antibiotics, which block the growth of bacteria but allow the growth of yeasts, fungal opportunists, and pathogenic fungi, including pathogenic fungi (dermatophytes, some H. capsulatum). This is often one of the first initial media types that suspected fungi are plated onto for growth. This is sometimes referred to as Mycosel Agar. Mycosel formulation usually contains cycloheximide.
Brain Heart Infusion Agar (BHI) with Blood, Gentamicin, Chloramphenicol, Cycloheximide :
This agar is great for the recovery of fastidious fungal pathogens because it blocks the growth of fungal opportunists, bacteria, and actinomycetes. Media containing cycloheximide may inhibit some strains of Cryptococcus neoformans. There is also a broth version of the media (BHI broth). This enriched type of media is essential for the conversion of the dimorphic molds to yeast (tissue) phase, which is necessary for their identification.
Dermatophyte Test Medium (DTM):
This media type contains both antibiotics and a phenol red indicator so that when a dermatophyte grows, it will change the color of the agar from yellow to red. This media type is commonly used in dermatology offices.
Niger (Birdseed) Agar (Caffeic Acid): (Selective)
The sputum from immunocompromised or AIDS patients with suspected C. neoformans may be plated on Niger (Birdseed) Agar (caffeic acid) because it is selective for this organism. It prevents bacterial overgrowth, and will grow dark brown (other yeasts will grow as beige or white). The caffeic acid disk test can also be used for this purpose and is specific for Cryptococcus neoformans, which will turn the disk to a pasty brown color if positive for this organism.
Potato Flake Agar: (Selective)
This medium is used to encourage mold sporulation in addition to fungal hyphae, which can be observed microscopically with a lactophenol cotton blue scotch tape preparation test. It also enhances the pigment production of molds.
Cornmeal Agar: (Selective)
This medium is used to encourage the rapid growth of yeasts and to enhance and induce the production of blastoconidia and/or chlamydospores and pseudohyphae and yeast pigment to aid in the identification process. This agar is observed under the microscope for the pattern and arrangement of blastoconidia, chlamydoconidia/chlamydospores, and whether or not pseudohyphae are present.
It is crucial that the mycologist always work under a biological hood to prevent contamination, always wear a lab coat, gloves and mask, autoclave specimens and inoculated media upon finishing or completing work with the specimen, and disinfect the work area daily or multiple times throughout the work day.
NONSELECTIVE MEDIA:
Sabouraud Brain Heart Infusion Agar (SABHI)-This is often the medium of choice for initial isolation because it is richer in nutrients than Sabouraud Dextrose Agar (SDA) and supports the growth of a wider variety of fungi. It allows bacteria, the fungal opportunists, yeasts, dermatophytes, subcutaneous pathogens, and most systemic pathogens to grow, however, some of the fastidious organisms like H. capsulatum or B. dermatiditis will not grow on this media.
This media is stored in the refrigerator and must be brought to room temperature prior to inoculation. Swab the whole surface of the agar slant and push the specimen lightly into the agar. Because agar contains no antibiotics, inoculate this one first before inoculating media containing antibiotics to prevent carryover. Loosen the cap and incubate at 30 degrees Celsius for up to 1 month before discarding it and concluding that it is negative for growth.
Brain Heart Infusion Agar With Blood (BHIB):
This media is richer in nutrients than SABHI. It is used to inoculate specimens from normally sterile sites or for suspect anaerobic actinomycetes.
Sabouraud Dextrose Agar (SDA):
This media is not nutritionally rich, and has an acid pH of 5.6. This media inhibits the growth of many bacteria. Fungal opportunists and pathogenic fungi grow well, however, all with the exception of H. capsulatum and many strains of N. asteroides. The media should be treated exactly like SABHI agar. This is a great, nonspecific agar used to grow a variety of fungi.
*If Nocardia is suspected, then paraffin may be added to the nonselective fungal medium to block the overgrowth of bacteria and to enhance the growth of Nocardia.
SELECTIVE MEDIA WITH ANTIBIOTICS:
Inhibitory Mold Agar (IMA):
This media contains gentamicin and sometimes chloramphenicol antibiotics, which block the growth of bacteria but allow the growth of yeasts, fungal opportunists, and pathogenic fungi, including pathogenic fungi (dermatophytes, some H. capsulatum). This is often one of the first initial media types that suspected fungi are plated onto for growth. This is sometimes referred to as Mycosel Agar. Mycosel formulation usually contains cycloheximide.
Brain Heart Infusion Agar (BHI) with Blood, Gentamicin, Chloramphenicol, Cycloheximide :
This agar is great for the recovery of fastidious fungal pathogens because it blocks the growth of fungal opportunists, bacteria, and actinomycetes. Media containing cycloheximide may inhibit some strains of Cryptococcus neoformans. There is also a broth version of the media (BHI broth). This enriched type of media is essential for the conversion of the dimorphic molds to yeast (tissue) phase, which is necessary for their identification.
Dermatophyte Test Medium (DTM):
This media type contains both antibiotics and a phenol red indicator so that when a dermatophyte grows, it will change the color of the agar from yellow to red. This media type is commonly used in dermatology offices.
Niger (Birdseed) Agar (Caffeic Acid): (Selective)
The sputum from immunocompromised or AIDS patients with suspected C. neoformans may be plated on Niger (Birdseed) Agar (caffeic acid) because it is selective for this organism. It prevents bacterial overgrowth, and will grow dark brown (other yeasts will grow as beige or white). The caffeic acid disk test can also be used for this purpose and is specific for Cryptococcus neoformans, which will turn the disk to a pasty brown color if positive for this organism.
Potato Flake Agar: (Selective)
This medium is used to encourage mold sporulation in addition to fungal hyphae, which can be observed microscopically with a lactophenol cotton blue scotch tape preparation test. It also enhances the pigment production of molds.
Cornmeal Agar: (Selective)
This medium is used to encourage the rapid growth of yeasts and to enhance and induce the production of blastoconidia and/or chlamydospores and pseudohyphae and yeast pigment to aid in the identification process. This agar is observed under the microscope for the pattern and arrangement of blastoconidia, chlamydoconidia/chlamydospores, and whether or not pseudohyphae are present.
Image by Jeanette Sprute, MT-AMT, M-ASCP (cm), 2015, own work
|
Image by Jeanette Sprute, MT-AMT, M-ASCP (cm), 2015, own work
|
Image by Jeanette Sprute, MT-AMT, M-ASCP (cm), 2015, own work
|
Image by Jeanette Sprute, MT-AMT, M-ASCP (cm), 2015, own work
|
Image by Jeanette Sprute, MT-AMT, M-ASCP (cm), 2015, own work
|
Image by Jeanette Sprute, MT-AMT, M-ASCP (cm), 2015, own work
|
Cryptococcus neoformans growing on Niger (Birdseed) Agar as small, dark brown colonies. Other yeasts growing on this plate are white.
|

The "lollipop" arrangement of terminal chlamydospores unique to C. albicans yeast, seen microscopically on cornmeal agar.
|
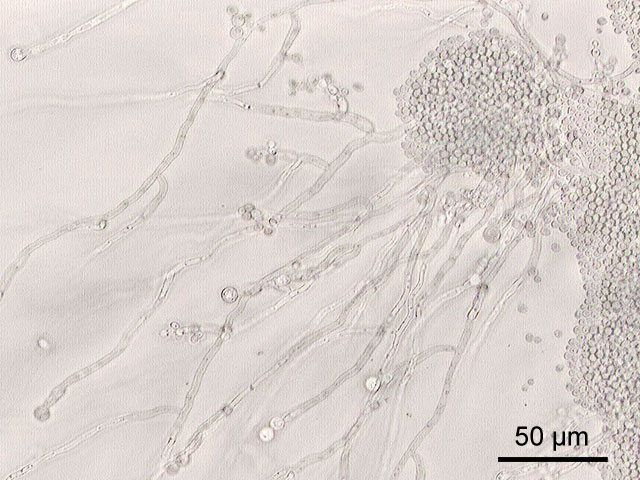
Candida albicans viewed microscopically and directly on cornmeal agar.
Aspergillus spp on potato dextrose agar
|
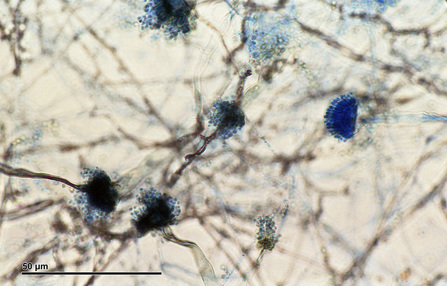
Example of a lactophenol cotton blue scotch tape preparation made off of the potato dextrose agar
|

Sabouraud Dextrose Agar
|

BHI Broth
|

Inhibitory Mold Agar (IMA)
|
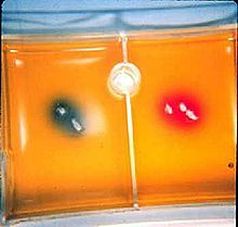
Dermatophyte Test Medium Agar (DTM)
|
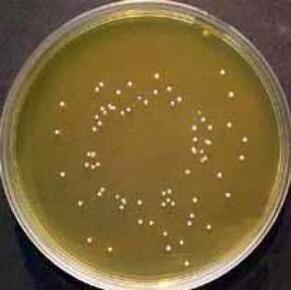
BHI Agar Without Blood
|

BHI With Blood Agar
|

Trichophyton on Trichophyton Agars 1, 2, 3 & 4 and on urea agar. Thiamine is vitamin B1.
|

Cornmeal agar
|
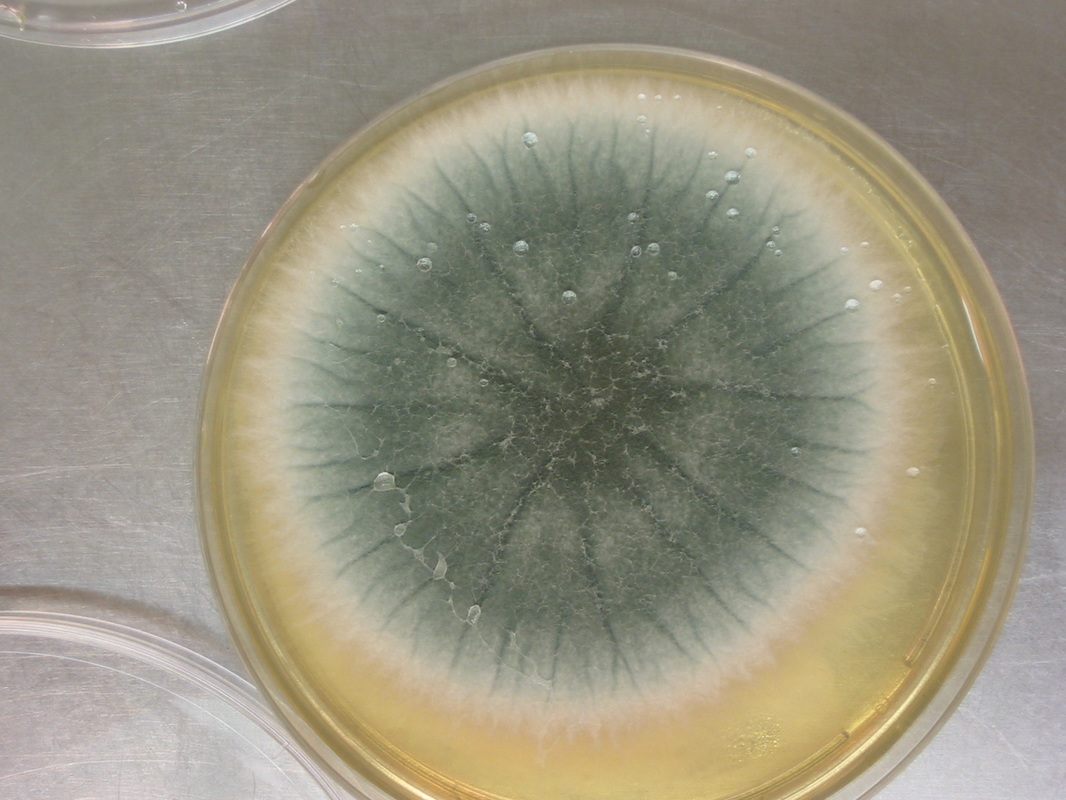
Aspergillus spp on Potato Flake Agar (PFA)

https://upload.wikimedia.org/wikipedia/commons/thumb/b/b8/Working_at_Biological_Safety_Cabinet_%286166411754%29.jpg/640px-Working_at_Biological_Safety_Cabinet_%286166411754%29.jpg
CULTURING AND TECHNIQUE:
Following inoculation and sealing with parafilm or shrink seal, fungal cultures are typically incubated at 30 degrees Celsius, though room temperature incubation is often acceptable as well, though slower growth may occur. It is preferable to first isolate dermatophytes in the mold phase (room temperature or 30 degrees Celsius), then convert them to the yeast phase at 37 degrees Celsius. Note that some organisms do grow better at 37 degrees Celsius, and you can always do a temperature challenge if unsure.
Cryptococcus neoformans tends to grow best at 37 degrees Celsius. Aspergillus spp grows well at 30, 37 and 45 degrees Celsius. In general, incubation time ranges from 3-4 days to up to 12 weeks, therefore, it is important to check fungal cultures at least once a week, more if time permits. Some fungi mature quickly, whereas others require a longer incubation time.
It is important to maintain a moist environment (40-50% humidity) when culturing organisms to keep them from drying out and to enhance fungal growth. For this reason, most labs have a pan that is filled up with or topped off with sterile, deionized, or distilled water that is kept at the bottom of each incubator. It should be dumped out and cleaned and refilled at least once a week. Levels should be monitored and recorded regularly. At the same time, cultures perform better if moisture is wiped from the the new plate lids prior to inoculating them and sealing them, storing them in the dark, and making sure they are refrigerated during storage but allowed to come to room temperature prior to inoculation.
Once again, it is also critical to seal the plates with parafilm or air-permeable tape to prevent contamination with fungal spores. When culturing slants, keep all caps screwed loosely upon incubation, tightening them after a day or so.
Once fungi have initially grown on primary media, it is important to frequently subculture them to fresh media for complete isolation and to promote sporulation and identification. Yeasts are subcultured to SDA (Emmon's modification), which has lower levels of glucose and a neutral pH or to birdseed agar for rapid identification of C. neoformans. Yeasts are also subcultured to cornmeal agar to promote formation of blastoconidia and chlamydospores. Molds are subcultured to potato dextrose agar (PDA), because it promotes sporulation and pigmentation of colonies.
Most mycology labs hold cultures for 28-30 days to make sure there is enough time for slow-growers to be identified. Rapid-growers will form mature colonies in 5 days or less, and include most fungal opportunists, yeasts, some dimorphic molds, and fungus-like bacteria. Intermediate-growers will form mature colonies in about a week (6-10 days), and include the dermatophytes, C. immitis, Scedosporium apiospermum, H. capsulatum. Slow-glowers form mature colonies in 11-21 days but some may take a little longer and need to be subcultured. These include the dermatophytes Microsporum audouinii, T. rubrum, T. schoenleinii, T. tonsurans, T. verrucosum. T. violaceum, the dematiaceous molds (dark molds), ad most of the systemic molds. The dimorphic mold Paracoccidioides brasiliensis is also a slow-grower.
Following inoculation and sealing with parafilm or shrink seal, fungal cultures are typically incubated at 30 degrees Celsius, though room temperature incubation is often acceptable as well, though slower growth may occur. It is preferable to first isolate dermatophytes in the mold phase (room temperature or 30 degrees Celsius), then convert them to the yeast phase at 37 degrees Celsius. Note that some organisms do grow better at 37 degrees Celsius, and you can always do a temperature challenge if unsure.
Cryptococcus neoformans tends to grow best at 37 degrees Celsius. Aspergillus spp grows well at 30, 37 and 45 degrees Celsius. In general, incubation time ranges from 3-4 days to up to 12 weeks, therefore, it is important to check fungal cultures at least once a week, more if time permits. Some fungi mature quickly, whereas others require a longer incubation time.
It is important to maintain a moist environment (40-50% humidity) when culturing organisms to keep them from drying out and to enhance fungal growth. For this reason, most labs have a pan that is filled up with or topped off with sterile, deionized, or distilled water that is kept at the bottom of each incubator. It should be dumped out and cleaned and refilled at least once a week. Levels should be monitored and recorded regularly. At the same time, cultures perform better if moisture is wiped from the the new plate lids prior to inoculating them and sealing them, storing them in the dark, and making sure they are refrigerated during storage but allowed to come to room temperature prior to inoculation.
Once again, it is also critical to seal the plates with parafilm or air-permeable tape to prevent contamination with fungal spores. When culturing slants, keep all caps screwed loosely upon incubation, tightening them after a day or so.
Once fungi have initially grown on primary media, it is important to frequently subculture them to fresh media for complete isolation and to promote sporulation and identification. Yeasts are subcultured to SDA (Emmon's modification), which has lower levels of glucose and a neutral pH or to birdseed agar for rapid identification of C. neoformans. Yeasts are also subcultured to cornmeal agar to promote formation of blastoconidia and chlamydospores. Molds are subcultured to potato dextrose agar (PDA), because it promotes sporulation and pigmentation of colonies.
Most mycology labs hold cultures for 28-30 days to make sure there is enough time for slow-growers to be identified. Rapid-growers will form mature colonies in 5 days or less, and include most fungal opportunists, yeasts, some dimorphic molds, and fungus-like bacteria. Intermediate-growers will form mature colonies in about a week (6-10 days), and include the dermatophytes, C. immitis, Scedosporium apiospermum, H. capsulatum. Slow-glowers form mature colonies in 11-21 days but some may take a little longer and need to be subcultured. These include the dermatophytes Microsporum audouinii, T. rubrum, T. schoenleinii, T. tonsurans, T. verrucosum. T. violaceum, the dematiaceous molds (dark molds), ad most of the systemic molds. The dimorphic mold Paracoccidioides brasiliensis is also a slow-grower.

https://upload.wikimedia.org/wikipedia/commons/thumb/b/b6/Parafilm_Products.jpg/640px-Parafilm_Products.jpg
|

Aspergillus niger mold is growing on potato dextrose agar (PDA), which promotes both sporulation and pigmentation of colonies
|

https://upload.wikimedia.org/wikipedia/commons/thumb/9/9a/CO2_Incubator_in_Microbiology.jpg/640px-CO2_Incubator_in_Microbiology.jpg
|
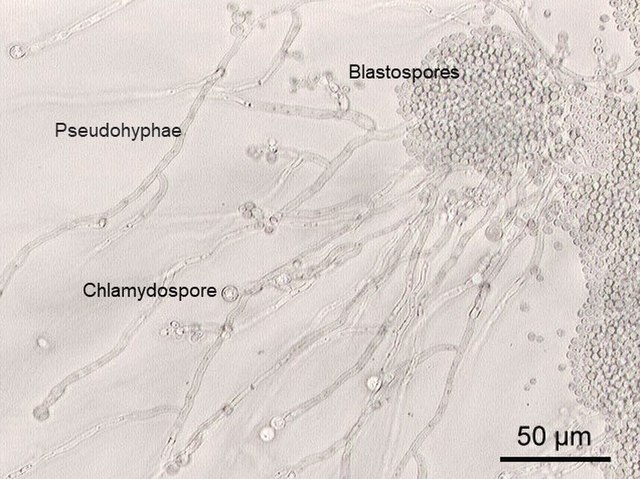
https://upload.wikimedia.org/wikipedia/commons/thumb/f/f5/C_albicans_en.jpg/640px-C_albicans_en.jpg
|
direct examination of cultures From plate growth:
MACROSCOPIC EXAMINATION:
A macroscopic examination should be performed once a mature colony has formed, and the texture, color, and topography should be noted. The following procedures may be performed to aid in identification:
THE TEASE MOUNT METHOD:
This method can be performed immediately after the fungal colony matures on the primary isolation agar plate. Careful teasing apart of hyphae should be performed so as not to disturb the position of the conidia or disrupt the fungal elements. Rough action should be avoided when performing the tease mount.
Place one drop of LPCB stain on a glass slide. Using 1 or 2 flamed and cooled stiff wire inoculating needles, pick up a small area of the fungal colony, being careful not to disrupt the elements. Carefully cut through the aerial hyphae and the vegetative mycelium, but avoid taking from the center or edge of the colony.
Place the fungal portion in the LPCB stain on the slide. Using a second sterile needle, gently tease apart the hyphae so that they form a thin layer on the slide, cover them with a cover slip, and press down to spread out the fungus. Examine under low and high power for reproductive structures. If you would like to make the slide permanent, simply rim the outer edge of the cover slip with Permamount or clear nail polish.
A macroscopic examination should be performed once a mature colony has formed, and the texture, color, and topography should be noted. The following procedures may be performed to aid in identification:
THE TEASE MOUNT METHOD:
This method can be performed immediately after the fungal colony matures on the primary isolation agar plate. Careful teasing apart of hyphae should be performed so as not to disturb the position of the conidia or disrupt the fungal elements. Rough action should be avoided when performing the tease mount.
Place one drop of LPCB stain on a glass slide. Using 1 or 2 flamed and cooled stiff wire inoculating needles, pick up a small area of the fungal colony, being careful not to disrupt the elements. Carefully cut through the aerial hyphae and the vegetative mycelium, but avoid taking from the center or edge of the colony.
Place the fungal portion in the LPCB stain on the slide. Using a second sterile needle, gently tease apart the hyphae so that they form a thin layer on the slide, cover them with a cover slip, and press down to spread out the fungus. Examine under low and high power for reproductive structures. If you would like to make the slide permanent, simply rim the outer edge of the cover slip with Permamount or clear nail polish.
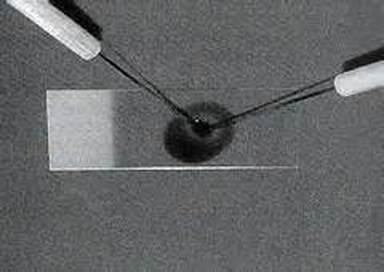
Tease apart fungal hyphae gently in the tease mount method

https://upload.wikimedia.org/wikipedia/commons/thumb/e/ef/Fungal_elements_in_LPCB_Tease_Mount.jpg/640px-Fungal_elements_in_LPCB_Tease_Mount.jpg
CELLOPHANE/SCOTCH TAPE METHOD:
Perform this technique with mature fungal colonies growing on plates under the biological hood using aseptic technique. Prepare a glass slide with a drop of lactophenol cotton blue (LPCB) stain and set the slide aside. Take a 2" piece of transparent (clear) cellophane tape, roll it, and hold it between your fingers with the sticky side facing outward. Touch the sticky side of the tape to the top of the fungal colony (aerial hyphae). The sporulation structures should be stuck to the tape. Place the tape, sticky side down, carefully on the slide over the LPCB. Stretch the tape across the slide and press both ends to attach it firmly to the slide. There is no need to add a cover slip because the tape serves as a temporary cover slip. Examine the slide under low and high power for fruiting structures. The cellophane tape method cannot be used to make a permanent slide for permanent storage with the tape, however, you can remove it and replace it with a coverslip, seal it with clear nail polish or permamount, then you will be able to seal it permanently for future use.
Perform this technique with mature fungal colonies growing on plates under the biological hood using aseptic technique. Prepare a glass slide with a drop of lactophenol cotton blue (LPCB) stain and set the slide aside. Take a 2" piece of transparent (clear) cellophane tape, roll it, and hold it between your fingers with the sticky side facing outward. Touch the sticky side of the tape to the top of the fungal colony (aerial hyphae). The sporulation structures should be stuck to the tape. Place the tape, sticky side down, carefully on the slide over the LPCB. Stretch the tape across the slide and press both ends to attach it firmly to the slide. There is no need to add a cover slip because the tape serves as a temporary cover slip. Examine the slide under low and high power for fruiting structures. The cellophane tape method cannot be used to make a permanent slide for permanent storage with the tape, however, you can remove it and replace it with a coverslip, seal it with clear nail polish or permamount, then you will be able to seal it permanently for future use.
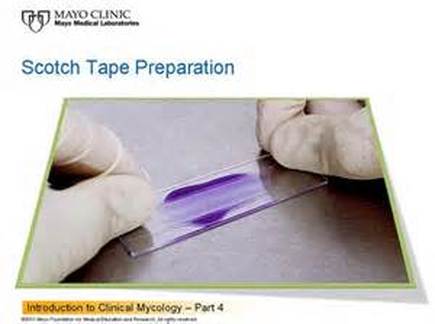
Cellophane Tape Method
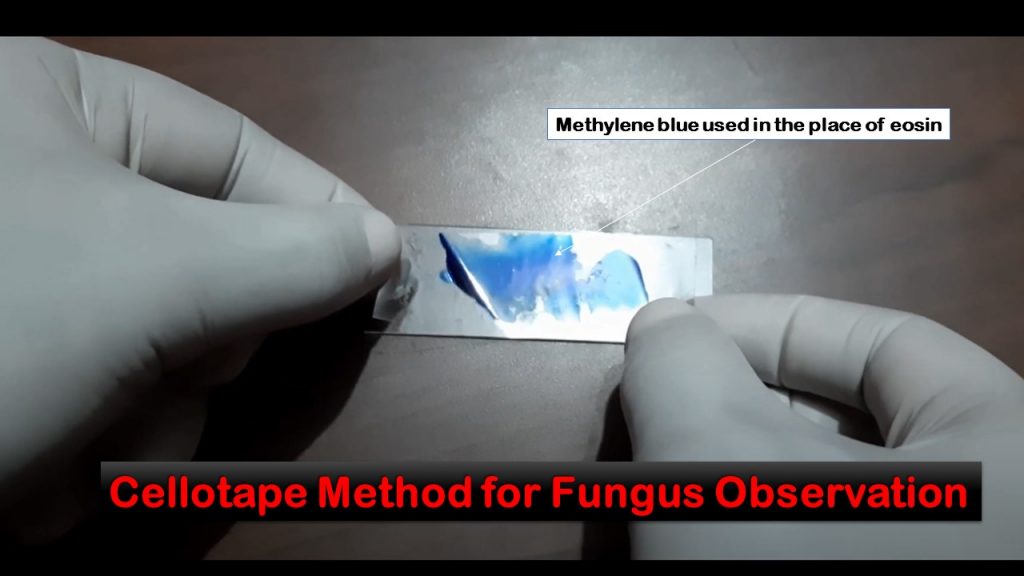
https://external-content.duckduckgo.com/iu/?u=https%3A%2F%2Funiverse84a.com%2Fwp-content%2Fuploads%2F2021%2F09%2FCellotape-Method-for-Fungus-Observation-Introduction-Test-Requirements-Test-Procedure-and-Result-Interpretation-1024x576.jpg&f=1&nofb=1&ipt=fa52352d1e47dfaec7b3f928c9ee2ff58bcfe8e2d79f623bbb348bb27811e4ae&ipo=images
Slide Culture Method and Modified Slide Culture Method:

|
|
COVERSLIP SANDWICH TECHNIQUE:
In this method, streaks of fungus on PDA are sandwiched with cover slips to enhance rapid growth. Cover slips are inserted directly onto the agar surface into streaks at 45-degree angles. When the colonies are mature, cover slips are removed. The cover slip is placed on a glass slide with LPCB stain. A second, larger cover slip is sandwiched with LPCB stain over the top of the first cover slip and then observed microscopically under low and high power. There should be fungal growth on both sides of the cover slip.
In this method, streaks of fungus on PDA are sandwiched with cover slips to enhance rapid growth. Cover slips are inserted directly onto the agar surface into streaks at 45-degree angles. When the colonies are mature, cover slips are removed. The cover slip is placed on a glass slide with LPCB stain. A second, larger cover slip is sandwiched with LPCB stain over the top of the first cover slip and then observed microscopically under low and high power. There should be fungal growth on both sides of the cover slip.
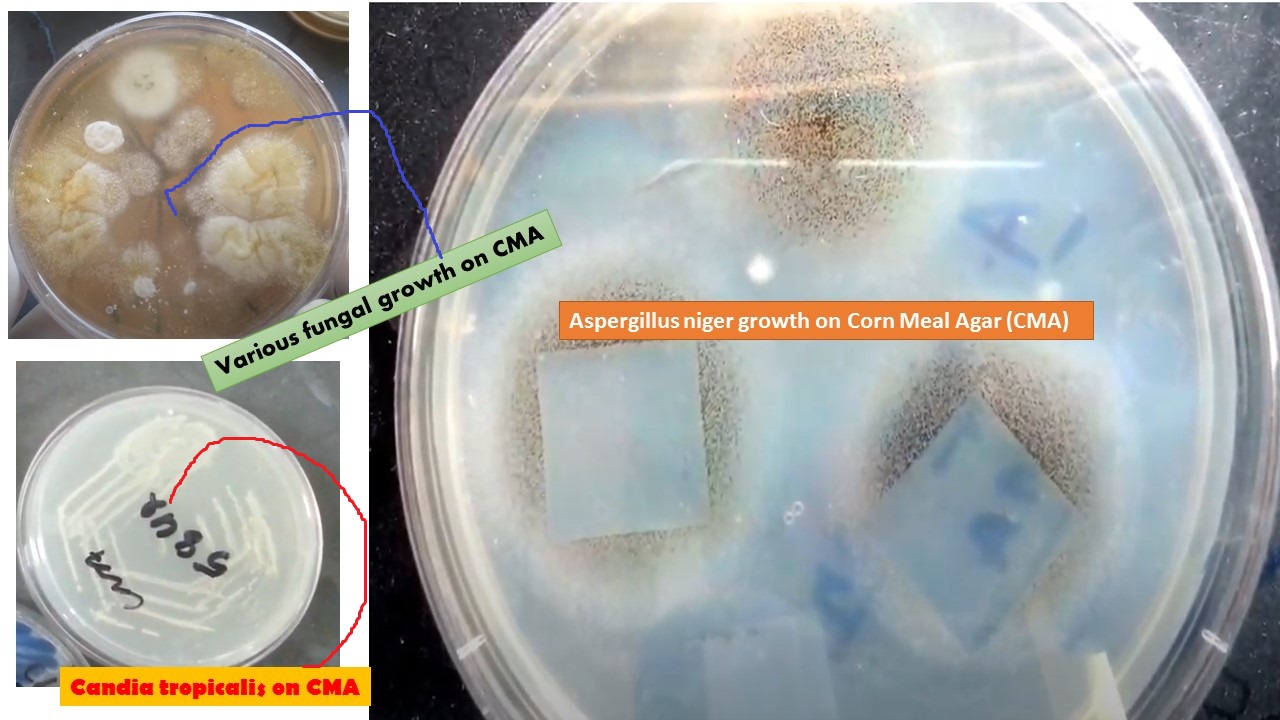
https://external-content.duckduckgo.com/iu/?u=https%3A%2F%2Funiverse84a.com%2Fwp-content%2Fuploads%2F2020%2F09%2FCorn-Meal-Agar-CMA-Introduction-Principle-Composition-Test-Procedure-Colony-Characteristics-and-Uses.jpg&f=1&nofb=1&ipt=6b1e5324bf738b70f8aa6b2bca403f9d1a6efc74e4248934fe8732615296763b&ipo=images (Dalmau Method)
other testing:
1. Vitek Yeast Card
2. MALDI-TOF Mass Spectrophotometry Identification (Yeasts, Molds)
3. Biofire Microfilmarray PCR or other PCR method (molecular)
Polymerase chain reaction (PCR) is great because it is rapid, accurate and sensitive. It can detect just one single strand of DNA in a sample. It amplifies DNA a millionfold!
2. MALDI-TOF Mass Spectrophotometry Identification (Yeasts, Molds)
3. Biofire Microfilmarray PCR or other PCR method (molecular)
Polymerase chain reaction (PCR) is great because it is rapid, accurate and sensitive. It can detect just one single strand of DNA in a sample. It amplifies DNA a millionfold!
how do you preserve a culture?
One of the questions I get asked a lot is how to preserve a fungal culture. This is something that is not done as frequently as it was years ago, but the methods are still the same.
- You can simply use distilled or sterile water. Once you have growth and sporulation of a mold on a solid medium, such as SAB or PDA, add 2-3 mL of sterile distilled water over the culture on the Petri dish. You can then use sterile inoculating needles or spatulas to scrape the sporulating fungal elements into the water, then use a sterile wire loop or sterile pipette tip to aspirate the water and trasnfer it to a sterile screw-capped tube. Tighten the cap and store it at room temperature. Label it with the name of the organism, the date prepared, and any other pertinent information required by your facility. Cultures will stay preserved anywhere from 5-20 years.
- Cryoprecipitate beads can be used to freeze the fungi, but you will need to thaw, replate, and refreeze them annually. The beads come in a small vial of cryoprecipitate (glycerol-based). Using sterile technique, carefully use a sterile loop to scrape some of the mold or yeast and roll it around in the vial of beads until you feel they are all inoculated. Label, place in a rack, and freeze. Make sure you include the date frozen. Annually, plate one bead onto a SAB dextrose plate to create a fresh culture, grow it, let it sporulate, and perform this method again. It is helpful to keep a log or spreadsheet of your inventory.
- Lyophilization (freeze-drying)
- Oil overlay is another method you can use. First, sterilize mineral oil by placing it in a glass vial or tube and autoclave it. Allow it to cool. Perform the same technique as in #1, but use oil instead of sterile water. This will preserve molds for years.With any of these methods, it is highly important to parafilm the caps of all samples.
the common fungal opportunists:
This section discusses and shows images of common fungal opportunists that you may encounter in the mycology laboratory. These are often seen in routine fungal cultures so it is important to be able to differentiate them from the regularly pathogenic (disease-causing) fungi. Opportunists are found everywhere and pose no harm much of time, but if they are in the right place at the right time under the right conditions (opportunity), they can cause an opportunistic infection.
FACTS ABOUT FUNGAL OPPORTUNISTS:
ASEPTATE OPPORTUNISTIC PATHOGENS: ZYGOMYCETES
These are fungi whose hyphae is free of cross-walls and fall into the phylum Zygomycota (Zygomycetes). The hyphae are wide and ribbon-like.
Phylum Zygomycota come from the Greek word "zygos", which means "joining" or "yoke". There are approximately 1,060 known species. Some of these molds are plant, insect or small animal parasites, whereas others are plant symbionts, living in symbiosis with them.
Reproduction is both sexual and asexual, and the dormant spores lie dormant hours-to-years. They have a low rate of metabolism. The exogenous spores are dependent upon nutrients and temperature. The endogenous spores have their own metabolic features. During asexual reproduction, mitospores (sporangiospores), exhibit phototropism and thin walls that are easily destroyed by rain. The cell walls of these spores contain sporopollenin (Beta-carotene), which is resistant to biological and chemical degradation.
Treatment of fungal infections involving this mold includes posaconazole and Amp B.
FACTS ABOUT FUNGAL OPPORTUNISTS:
- Most are rapid growers and mature in about 4-5 days.
- They are saprobes and they thrive on dead or decaying organic matter in the soil. Sometimes, they are also airborne.
- They are frequent laboratory contaminants, since they are ubiquitous (found everywhere).
- They are usually nonpathogenic but may be opportunistic pathogens if conditions are just right (patient is ill, diabetic, hospitalized, immunosuppressed, immunocompromised) and can even cause rapid fatal infections and death in such cases.
- They are isolated on media free of antibiotics and must be repeatedly isolated in large numbers from cultured specimens from the patient to be sure they are opportunistic pathogens and not contaminants. Isolates should be transferred to potato dextrose agar (PDA) or corn meal tween-80 agar to enhance conidia production and coloration.
ASEPTATE OPPORTUNISTIC PATHOGENS: ZYGOMYCETES
These are fungi whose hyphae is free of cross-walls and fall into the phylum Zygomycota (Zygomycetes). The hyphae are wide and ribbon-like.
Phylum Zygomycota come from the Greek word "zygos", which means "joining" or "yoke". There are approximately 1,060 known species. Some of these molds are plant, insect or small animal parasites, whereas others are plant symbionts, living in symbiosis with them.
Reproduction is both sexual and asexual, and the dormant spores lie dormant hours-to-years. They have a low rate of metabolism. The exogenous spores are dependent upon nutrients and temperature. The endogenous spores have their own metabolic features. During asexual reproduction, mitospores (sporangiospores), exhibit phototropism and thin walls that are easily destroyed by rain. The cell walls of these spores contain sporopollenin (Beta-carotene), which is resistant to biological and chemical degradation.
Treatment of fungal infections involving this mold includes posaconazole and Amp B.
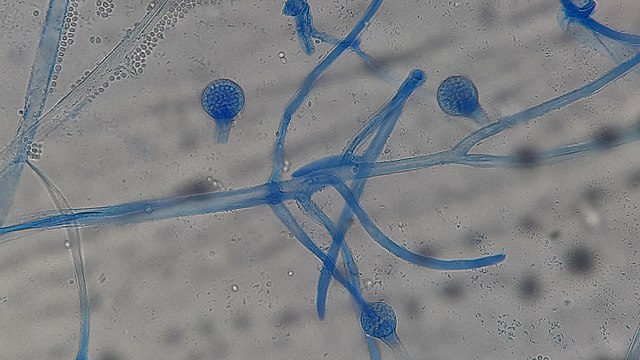
Wide, ribbon-like hyphae
*Absidia spp *Renamed to Lichtheimia corymbifera spp complex (Larone, 2023)
Causative agent of infrequent, rare zygomycosis and keratomycosis, but because this organism is ubiquitous, it may be a contaminant in laboratory cultures. It is found in the soil and it does spoil vegetation. It is an allergen to some individuals that can infect the lungs, nose, sinuses, brain, eyes, gastrointestinal system, or skin. Infection with this organism is associated with a poor prognosis. Infections are referred to as "phycomycosis".
They are a common cause of decaying vegetation and plant matter, soil, particularly in compost heaps. For this reason, when working outside with such materials, individuals should wear respirator masks if they suffer from allergies.
This organism was discovered in 1878 by Philippe Edward Leon Van Tieghem.
Macroscopic Exam:
Microscopic Exam:
Causative agent of infrequent, rare zygomycosis and keratomycosis, but because this organism is ubiquitous, it may be a contaminant in laboratory cultures. It is found in the soil and it does spoil vegetation. It is an allergen to some individuals that can infect the lungs, nose, sinuses, brain, eyes, gastrointestinal system, or skin. Infection with this organism is associated with a poor prognosis. Infections are referred to as "phycomycosis".
They are a common cause of decaying vegetation and plant matter, soil, particularly in compost heaps. For this reason, when working outside with such materials, individuals should wear respirator masks if they suffer from allergies.
This organism was discovered in 1878 by Philippe Edward Leon Van Tieghem.
Macroscopic Exam:
- Rapid grower (4 days)
- Gray to gray-olive, woolly/cottony colony with an umbonate center that fills the plate like cotton candy
Microscopic Exam:
- Broad, nonseptate hyphae (maybe a few form)
- No or rare rhizoids (rootlike hyphae)
- Large apophysis
- Collarette (only visible if the sporangial wall dissipates) at the base of the columella
- Pointed columella
- Branched sporangiophores that may arise from stolons (interconnected "runners") between rhizoids
- Pear-shaped sporangia (sac) filled with sporangiospores (spores)
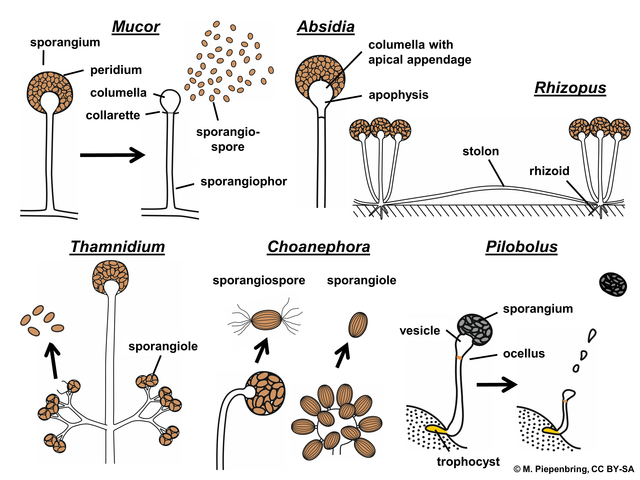
https://upload.wikimedia.org/wikipedia/commons/thumb/e/e2/Abb5.3_Mucoromycota_Mucorales_sporangiophores_Mucor_Absidia_Rhizopus_Thamnidium_Choanephora_Pilobolus_2021_%28M._Piepenbring%29.png/640px-Abb5.3_Mucoromycota_Mucorales_sporangiophores_Mucor_Absidia_Rhizopus_Thamnidium_Choanephora_Pilobolus_2021_%28M._Piepenbring%29.png
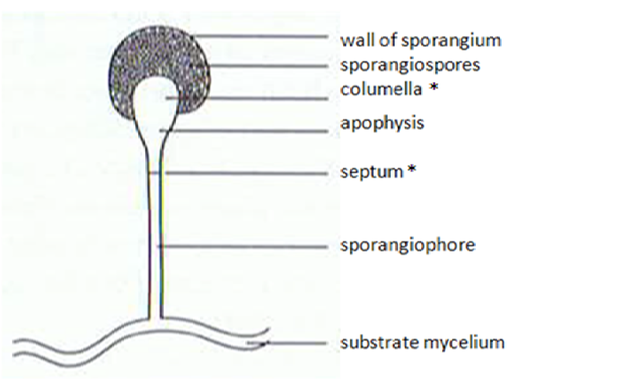
https://upload.wikimedia.org/wikipedia/commons/thumb/9/90/Sporangium..png/640px-Sporangium..png
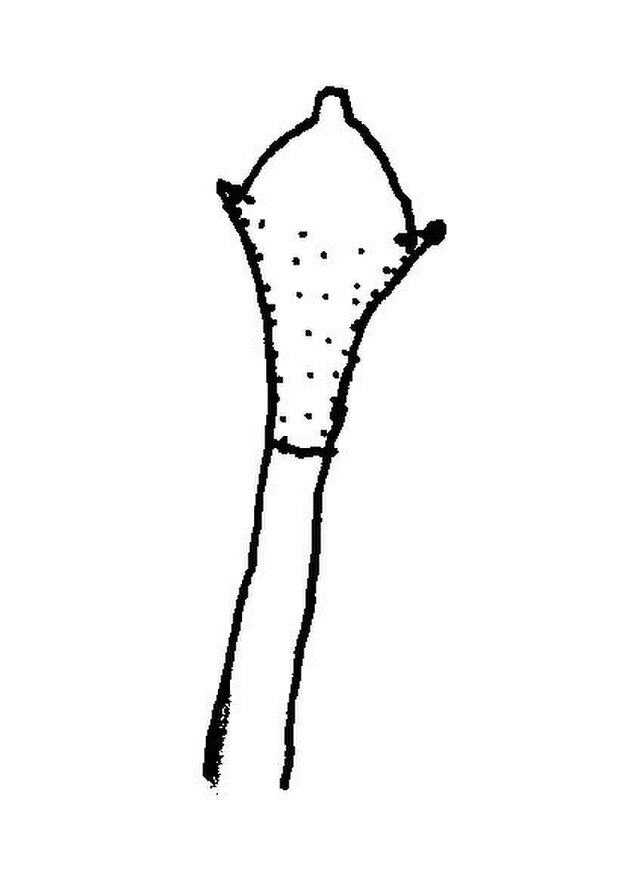
https://upload.wikimedia.org/wikipedia/commons/thumb/a/ac/Absidia_californica.jpg/640px-Absidia_californica.jpg
|
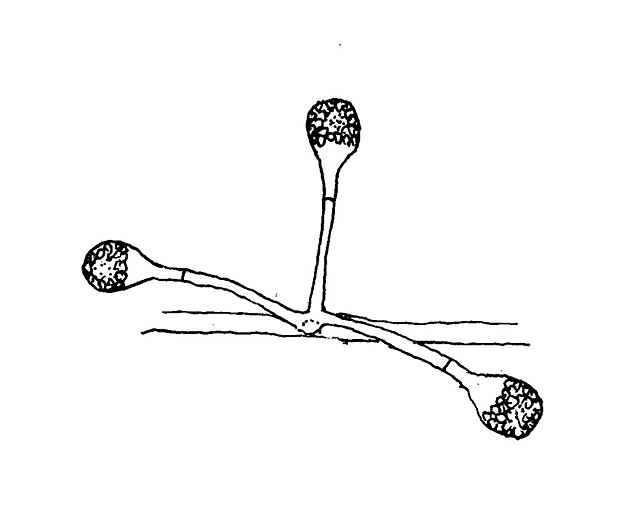
https://upload.wikimedia.org/wikipedia/commons/thumb/d/da/Absidia_cylindrospora.jpg/640px-Absidia_cylindrospora.jpg
|

Absidia "pear-shaped" columella and collarette supported by an aseptate, branching, wide hyphae (6-15 micrometers). As seen in the image above, once the sporangial wall dissipates, a pear-shaped collarette remains at the base of the columella.https://upload.wikimedia.org/wikipedia/commons/thumb/f/f7/Absidia_corymbifera.jpg/640px-Absidia_corymbifera.jpg
|

Absidia pear-shaped sporangia filled with sporangiospores, supported by pear-shaped columellas, collarettes, and long, aseptate, branching hyphae. In the background, you can see the stolons, which are interconnecting runners. This fungi is also known for its "root-like" rhizoids. It will grow on SABHI agar at room temperature.
|
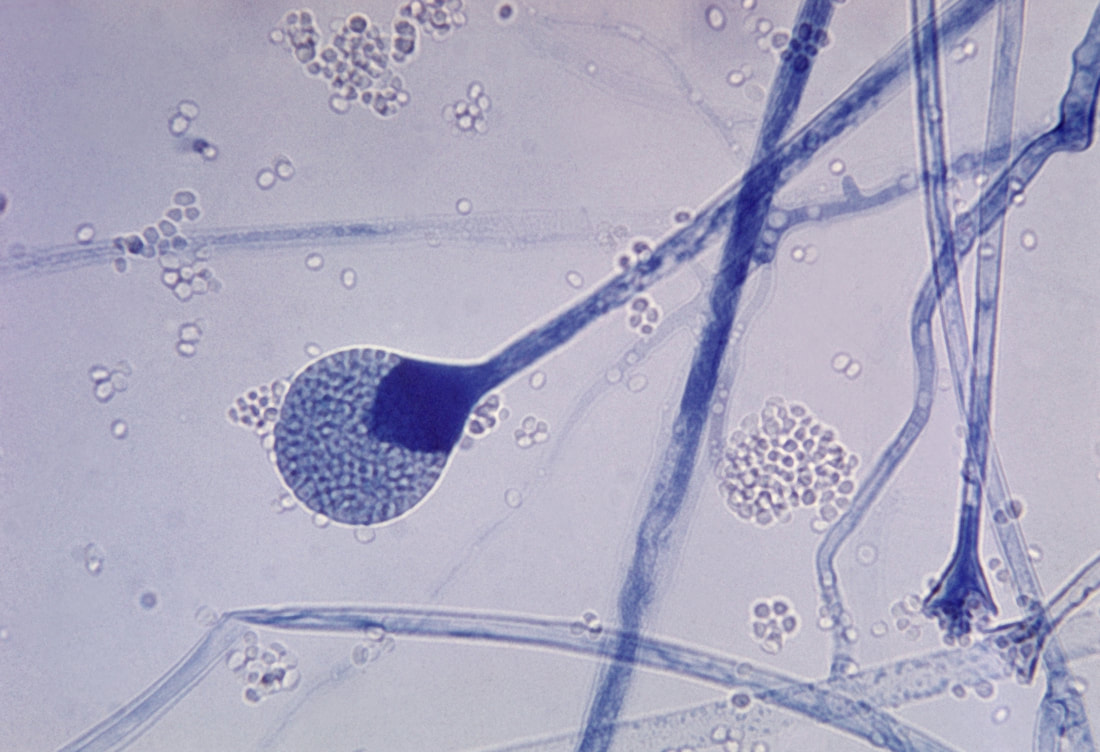
By Photo Credit:Content Providers: CDC/Dr. Lucille K. Georg - This media comes from the Centers for Disease Control and Prevention's Public Health Image Library (PHIL), with identification number #3960.Note: Not all PHIL images are public domain; be sure to check copyright status and credit authors and content providers.English | Slovenščina | +/−, Public Domain, https://commons.wikimedia.org/w/index.php?curid=4394127
|

At room temperature on SABHI agar, this mold grows rapidly within 4 days as a woolly, gray colony with an umbonate center, which rapidly matures and fills the plate or slant with fluff that looks like "cotton-candy". The reverse is colorless or white.
|
Apophysomyces spp:
This organism is an agent of zygomycosis, where infection is acquired through traumatic implantation through accidental injuries, insect bites or wounds, surgery, or skin and soft tissue infections following burns, automobile accidents, surgeries, injections, drug abuse. If it spreads, it can lead to necrotizing fasciitis, cerebritis, rhinoorbital disease, or kidney toxicity. It can also cause mucormycosis through inhalation of spores.
This organism is found in the soil and affects both immunocompetent and immunocompromised patients. It is considered to be an emerging fungal pathogen, and it can be fatal and cause serious infections. It is found in both tropical and subtropical areas.
Macroscopic Exam:
On SABHI agar, you will notice cotton-like white colonies that turn off-white or yellow with age. It grows up to 42 degrees Celsius. When subcultured to CMA or PDA at room temperature, you may just see hyphae, because they often fail to sporulate.
Microscopic Exam:
Unique microscopic features include:
Here are some images below:
This organism is an agent of zygomycosis, where infection is acquired through traumatic implantation through accidental injuries, insect bites or wounds, surgery, or skin and soft tissue infections following burns, automobile accidents, surgeries, injections, drug abuse. If it spreads, it can lead to necrotizing fasciitis, cerebritis, rhinoorbital disease, or kidney toxicity. It can also cause mucormycosis through inhalation of spores.
This organism is found in the soil and affects both immunocompetent and immunocompromised patients. It is considered to be an emerging fungal pathogen, and it can be fatal and cause serious infections. It is found in both tropical and subtropical areas.
Macroscopic Exam:
On SABHI agar, you will notice cotton-like white colonies that turn off-white or yellow with age. It grows up to 42 degrees Celsius. When subcultured to CMA or PDA at room temperature, you may just see hyphae, because they often fail to sporulate.
Microscopic Exam:
Unique microscopic features include:
- Unbranched sporangiophores
- Foot cells (bases)
- Apophyses that are funnel-shaped, swollen columellae
- Rhizoids that are thin-walled and found opposite the sporangiophores
- Sporangia that are pyriform
- Sporangiospores that are oval-shaped
Here are some images below:
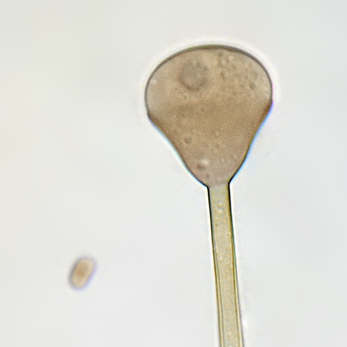
On SABHI, corn meal or potato dextrose agar at room temperature, the hyphae usually fail to sporulate as seen in the image above, with a pronounced apophysis that is "bell-shaped". To induce sporulation, you can aseptically transfer blocks of SABHI agar inoculated with fungus to tubes of sterile distilled water or 10% yeast extract medium that is used for the in vitro hair perforation test. Incubate at 37 degrees Celsius for 10-14 days. This creates the ideal conditions needed for the formation of unbranched sporangiophores with foot cells and funnel-shaped apophyses, and sporangia containing sporangiospores, which may be identified microscopically.
|

Apophysomyces spp are described as having oblong sporangium surrounded by a thin sporangial wall, filled with oblong sporangiospores supported by a cup-shaped apophysis and a sporangiophore with a foot cell (base) and "root-like" rhizoids. Another identifier is the darkening and thickening of the wall of the sporangiophore below the apophysis, as seen in the image above.
|

On SABHI at room temperature, Apophymyces spp grows as a cottony, woolly, fluffy white colony that grows and matures quickly within 4 days that fills the plate. With age, it will become off-white to yellow to brownish-gray in color. Because this mold is thermotolerant, it will also grow at temperatures of up to 42 degrees Celsius. The reverse is white to a pale yellow color.
Mucor spp:
Mycor species are the causative agent of mucormycosis, zygomycosis, otomycosis, or allergies and sinusitis. There are approximately six species of Mucor, and it is found in the soil, on plant surfaces, in digestive systems, rotting vegetation, and in some cheeses. Diabetics need to be careful of this mold, since they can get opportunistic infections from it, which can be deadly in some cases. Mucor is one of several molds normally found on bread that is molding and on molding vegetation.
Something interesting about this organisms is that it senses both light and gravity! Zygophores are the "sex organs" (+ and -), which grow toward each other due to volatile pheromones given off by the opposite strand, which attract them to each other. The precursor of this is trisporic acid. Once they make contact, it gives rise to a zygopore in a multi-step process. Their cell walls "stick" to each other, flattten, then become a fused septum. The septum extends inward, separating terminal gametangia from the base and becoming a suspensor.
Vesicles build up, the septum eventually dissolves, and the primary outer wall thickens. These are dark-colored molds due to the production of melanin pigment and sporopollenin. The branching hyphae bend because they are gravotropic. Lipid globules and lipases in the vesicles enable them to move toward the light (phototropic).The columnella has gravireceptors that sense gravity and exhibits floatability.
Mucor's lipases and proteases are used to make leather, detergents, and some steroid transformation medications.
Macroscopic Exam:
Microscopic Exam:
Mycor species are the causative agent of mucormycosis, zygomycosis, otomycosis, or allergies and sinusitis. There are approximately six species of Mucor, and it is found in the soil, on plant surfaces, in digestive systems, rotting vegetation, and in some cheeses. Diabetics need to be careful of this mold, since they can get opportunistic infections from it, which can be deadly in some cases. Mucor is one of several molds normally found on bread that is molding and on molding vegetation.
Something interesting about this organisms is that it senses both light and gravity! Zygophores are the "sex organs" (+ and -), which grow toward each other due to volatile pheromones given off by the opposite strand, which attract them to each other. The precursor of this is trisporic acid. Once they make contact, it gives rise to a zygopore in a multi-step process. Their cell walls "stick" to each other, flattten, then become a fused septum. The septum extends inward, separating terminal gametangia from the base and becoming a suspensor.
Vesicles build up, the septum eventually dissolves, and the primary outer wall thickens. These are dark-colored molds due to the production of melanin pigment and sporopollenin. The branching hyphae bend because they are gravotropic. Lipid globules and lipases in the vesicles enable them to move toward the light (phototropic).The columnella has gravireceptors that sense gravity and exhibits floatability.
Mucor's lipases and proteases are used to make leather, detergents, and some steroid transformation medications.
Macroscopic Exam:
- Colonies are fluffy, cottony, woolly and white, gray or beige.
- They grow extremely fast and may brown with age due to sporulation.
- Grows at all 3 temperatures
Microscopic Exam:
- Mucor spp lack rhizoids and have wide, aseptate hyphae bearing broad sporangiophores supporting sporangium filled with sporangia
- Sporangiophores may be branching or singular
- Most of the time, empty sporangial sacs are observed, as well as bare columellae with collarettes
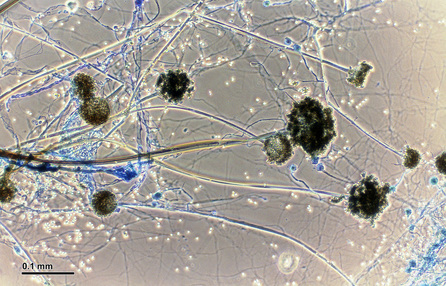
The mycelium of the Mucor spp is usually aseptate and sporangiophores may be branching or single, supporting round, spore-filled sporangia. Sometimes the empty sporangial sacs may be observed, as well as bare columellae with collarettes, which are variable in shape and either light or pigmented in color.
|

One distinguishing characteristic between Mucor spp, Rhizopus spp and Absidia spp is that in Mucor spp, THERE ARE NO RHIZOIDS OR STOLONS PRESENT.
|

At room temperature, on SABHI agar, Mucor spp grows as a fluffy, cottony, woolly white colony that grows rapidly. With age, it becomes gray to brown in color.
|

Mucor spp aerial hyphae
|

Mucor spp is consists of aseptate hyphae which branch, bearing mushroom-shaped columnellae, which bear oval-shaped sporangiospores cased within round to oval-shaped sporangium.
|
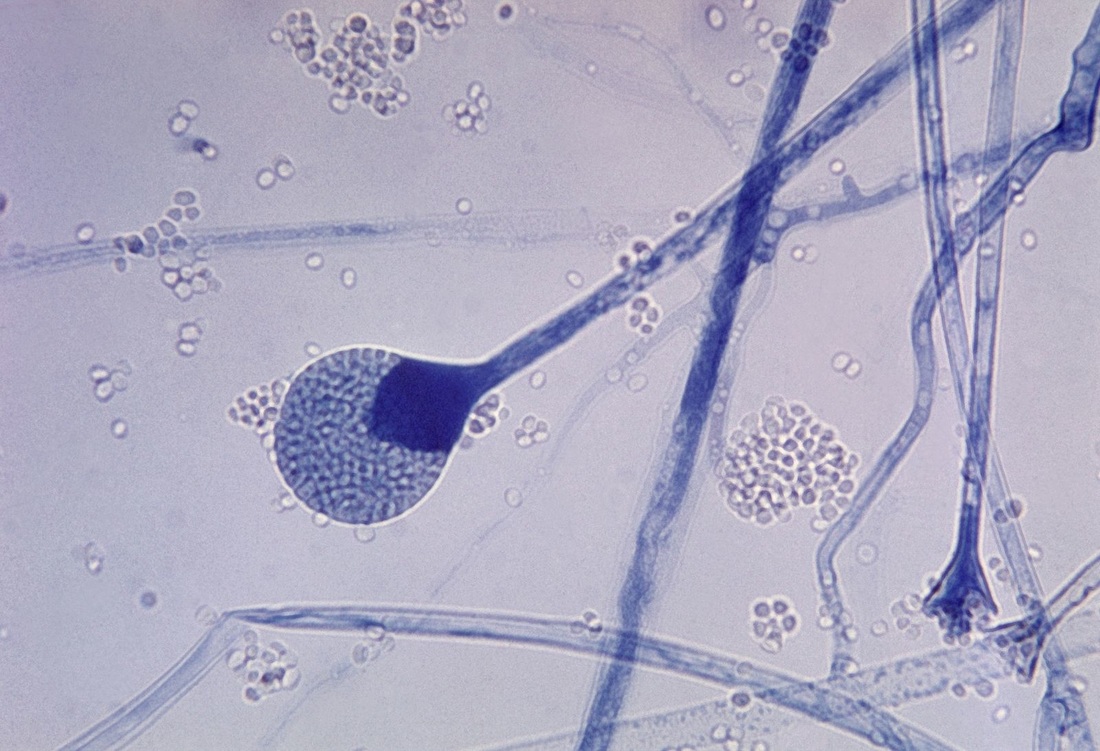
A beautiful Lactophenol Cotton Blue stained slide of Mucor species
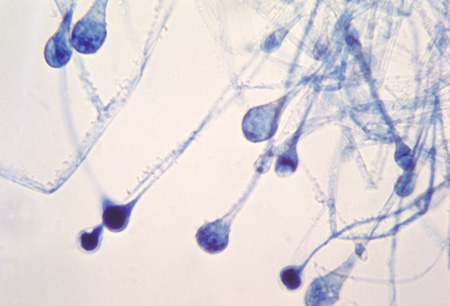
|
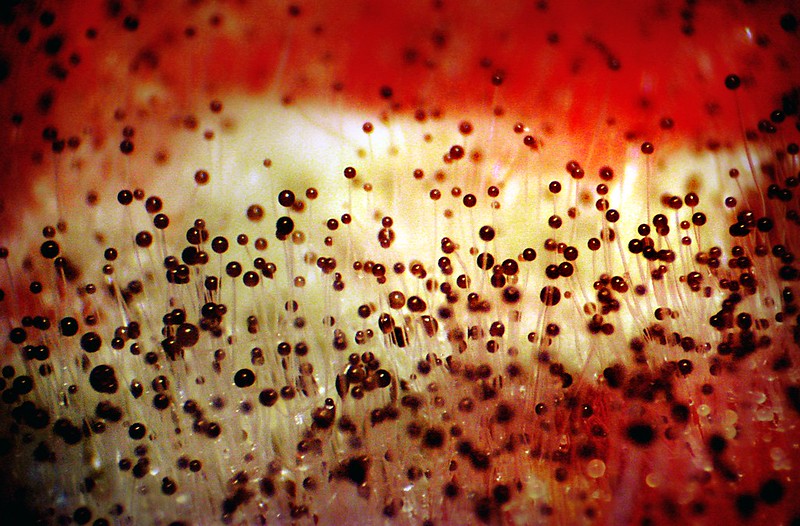
Mucor images by jeanette reynolds, 2022 (see below)
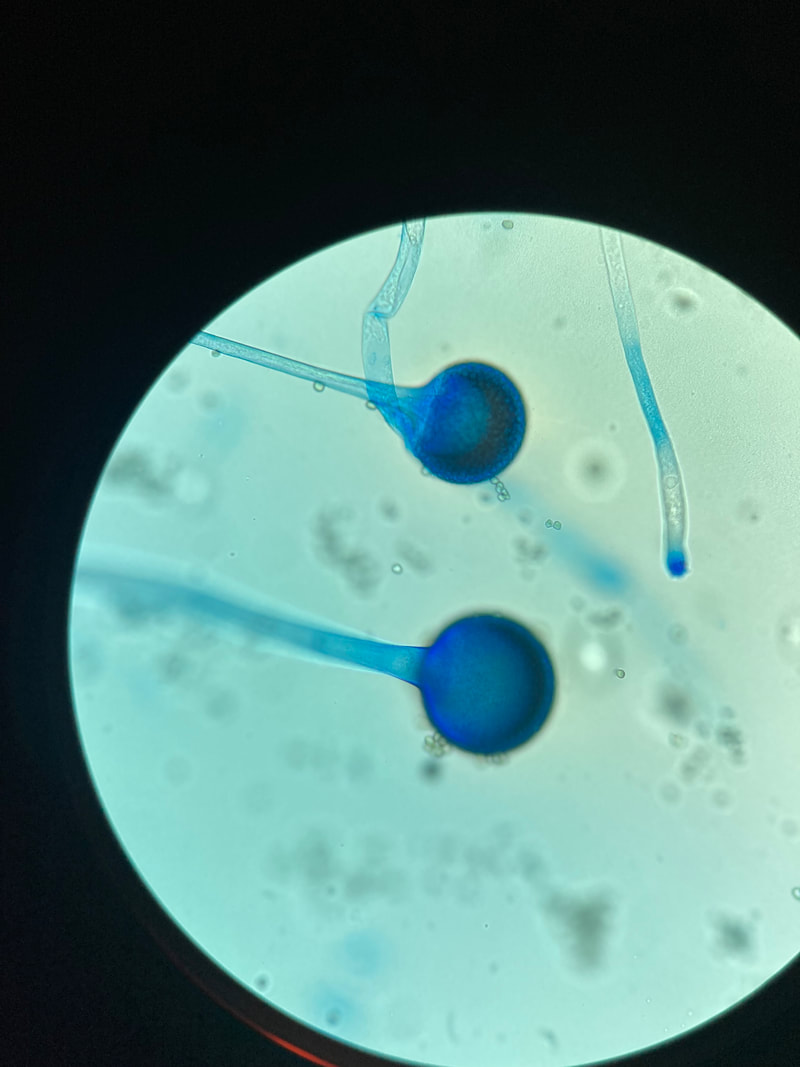
Mucor species in lactophenol cotton blue stain from a Scotch tape prep wet mount performed on bread mold, by Jeanette Reynolds, MS-Biology, MLS-AMT, M-ASCP, Certified in Emerging Diseases, Certified Instructor
|
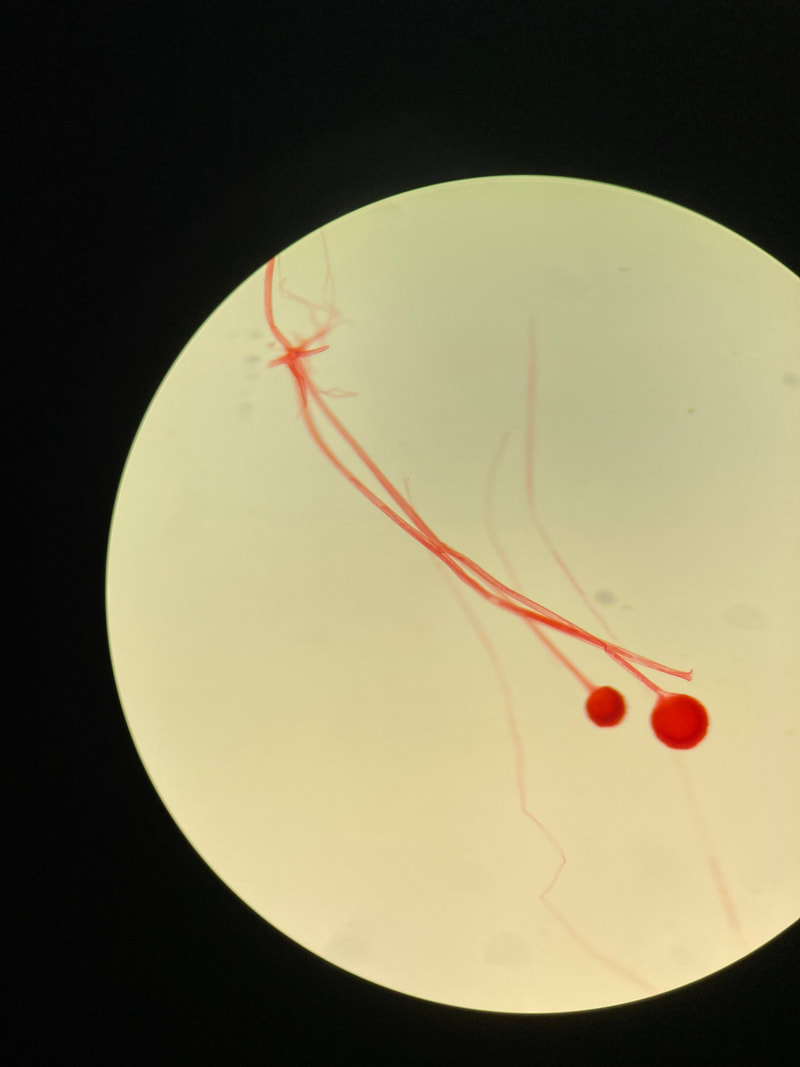
Jeanette Reynolds, MS-Biology, MLS-AMT, M-ASCP, Certified in Emerging Diseases, Certified Instructor
|

Mucor image in a lactophenol cotton blue stain and Scotch tape prep taken from bread mold by Jeanette Reynolds, MS-Biology, MLS-AMT, M-ASCP, Certified in Emerging Diseases, Certified Instructor
Image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
Rhizopus spp:
Rhizopus species were discovered by German Christian Gottfried Ehrenberg in 1818. There are approximately eight species of Rhizopus. The mold is a causative agent of zygomycosis and otomycosis, but can also be a contaminant. It grows in the soil, on decaying vegetation, on some animals, sugary foods like jams, jellies, syrups, bread, peanuts, and even tobacco and leather.
Opportunistic infections may result in zygomycosis or otomycosis in immunocompromised patients. It can also cause diabetic ketoacidosis. Diabetics should be very careful not to eat peanuts, peanut butter or breads contaminated with molds for this reason.
The zygospore grows and enlarges and thickens and darkens due to the pigment melanin. Meiosis occurs before spore germination, and the cell walls contain chitin and chitosan.
In industry, cellulases, fumaric acid, lactic acid and biotin produced by the mold are valued for food production (tempeh), supplements, face and hair products.
The organism grows well at 25-30 degrees and likes acidic pH as low as 2.2, but survives up to 9.6 pH. It produces ethyl alcohol, and it loves iron.
Macroscopic Exam:
Microscopic Exam:
Rhizopus species were discovered by German Christian Gottfried Ehrenberg in 1818. There are approximately eight species of Rhizopus. The mold is a causative agent of zygomycosis and otomycosis, but can also be a contaminant. It grows in the soil, on decaying vegetation, on some animals, sugary foods like jams, jellies, syrups, bread, peanuts, and even tobacco and leather.
Opportunistic infections may result in zygomycosis or otomycosis in immunocompromised patients. It can also cause diabetic ketoacidosis. Diabetics should be very careful not to eat peanuts, peanut butter or breads contaminated with molds for this reason.
The zygospore grows and enlarges and thickens and darkens due to the pigment melanin. Meiosis occurs before spore germination, and the cell walls contain chitin and chitosan.
In industry, cellulases, fumaric acid, lactic acid and biotin produced by the mold are valued for food production (tempeh), supplements, face and hair products.
The organism grows well at 25-30 degrees and likes acidic pH as low as 2.2, but survives up to 9.6 pH. It produces ethyl alcohol, and it loves iron.
Macroscopic Exam:
- Colonies are white, gray, beige or brown and fluffy, woolly or cottony due to sporulation.
Microscopic Exam:
- As seen in the images below, the mold is filamentous, broad, branching hyphae that are aseptate, lacking cross-walls.
- Sporangiospores are produced inside a round sporangium.
- The sporangium sits on a rounded columella.
- Rhizoids are present, opposite the sporangium.
- A stolon or runner is found between rhizoids and sporangiophores.

Broad aseptate hyphae are 6-15 micrometers in diameter and up to 4 mm long. Along the mycelia run many stolons, which connect groups of long sporangiophores. Sporangiophores are typically unbranched in this species. At the terminal end of the sporangiophore is a spherical, dark sporangium with a columnella and numerous oval-to-round brown spores. The sporangium is approximately 40-350 micrometers in diameter and the spores range from 4-11 micrometers.
|
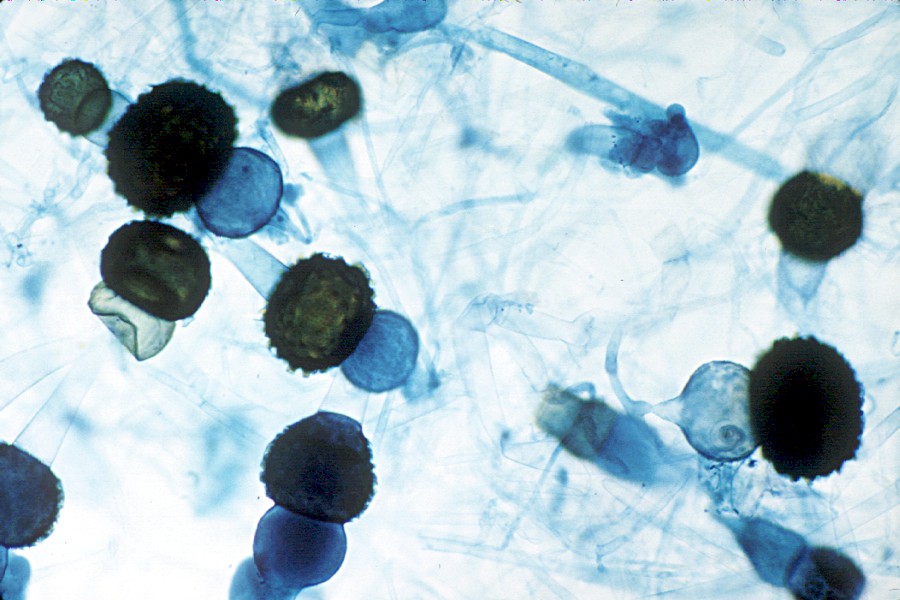
Numerous sporandium filled with sporangiospores
|
Beginning of the dissolution of the sporangial wall with dispersion of the small, round, brown spores
|

Once the sporangial wall dissolves, as seen in the image above, no collarette remains.
|
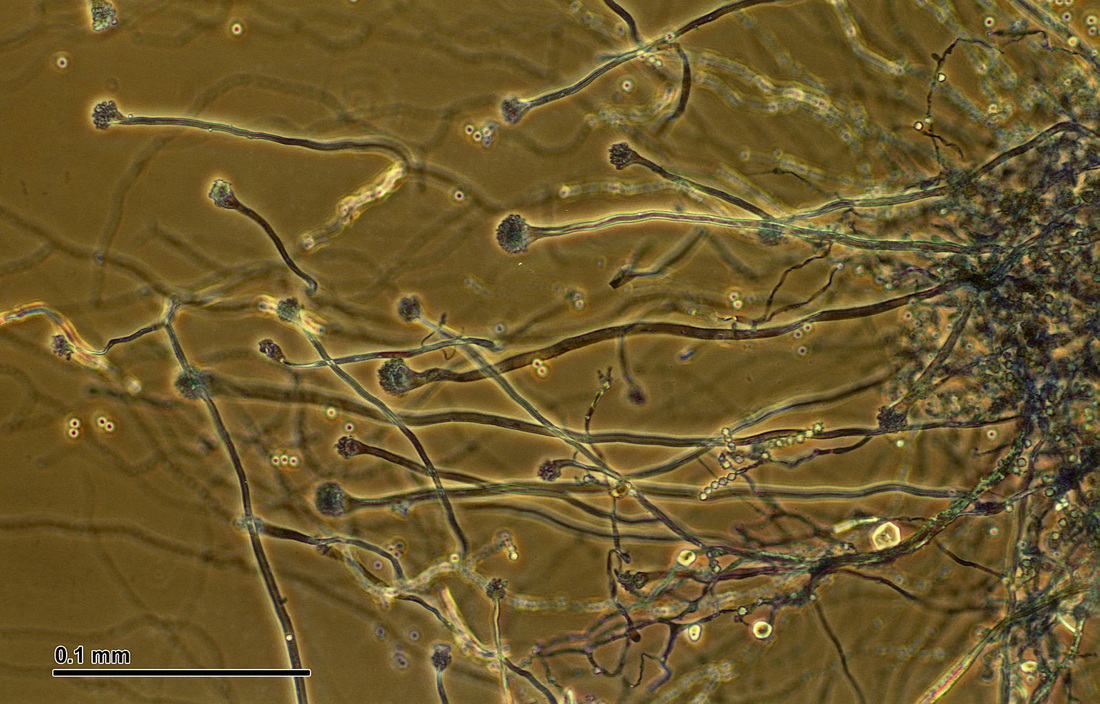
Rhizopus spp have hyphae that are usually aseptate and unbranched sporangiophores that arise opposite the root-like rhizoids at the nodes. There are usually connecting stolons between. The sporangiophores support round, spore-filled sporangia with flattened bases. On occasion, the sporangia will be completely empty, leaving only the columella to be observed. There are no collarettes.
|

Rhizopus grows on SABHI agar at room temperature as a white, dense, cottony/woolly/"cotton candy-like" colony with aerial hyphae that grow rapidly within 3-4 days, filling the plate with dense growth. The pathogenic species grow great at 37 degrees Celsius. With age, as seen in the image above, the colony will become dotted with black or brown sporangia. The reverse is white. Note that growth is inhibited by Cycloheximide.
|
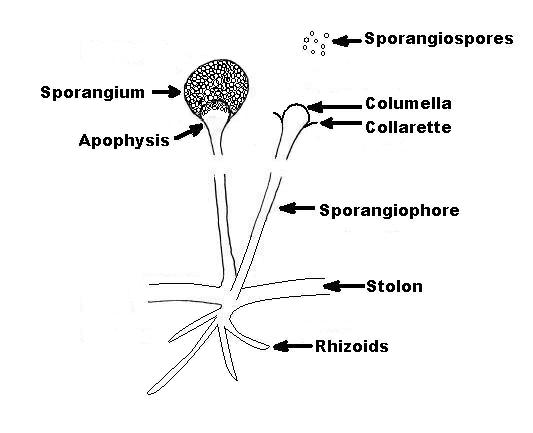
At the point at which the stolons and unbranched sporangiophores meet, notice that rhizoids ("root-like" hyphae) are produced as seen in this image. These features differentiate Rhizopus from Mucor spp. The aseptate hyphae, or sporangiophores, arise from root-like rhizoids between stolons. Small, round columnellas bear round sporangia filled with sporangiospores. Unlike Mucor or Rhizomucor spp, the hyphae of Rhizopus spp do not branch.
|
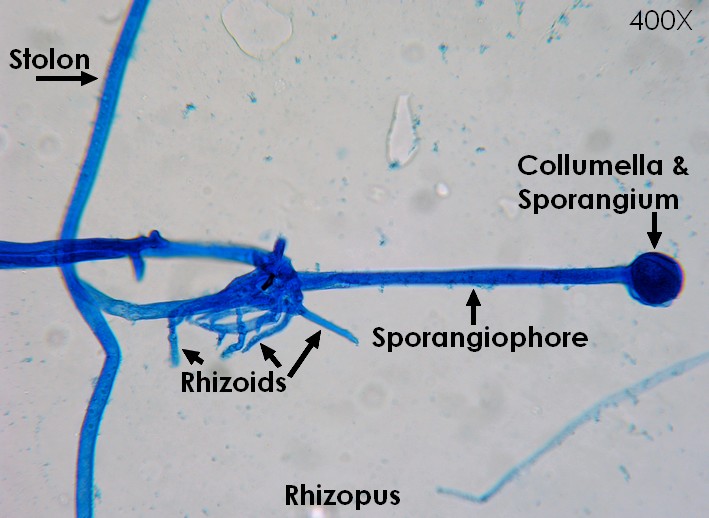
|
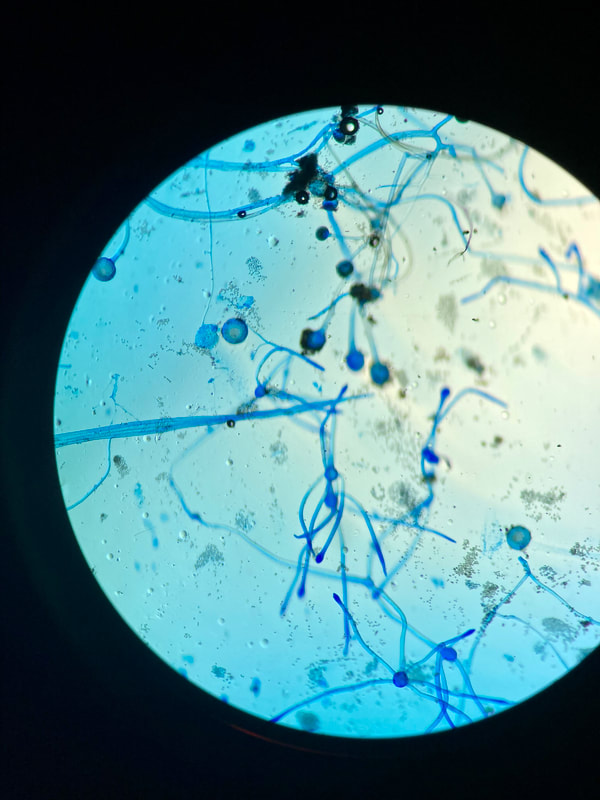
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|

Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
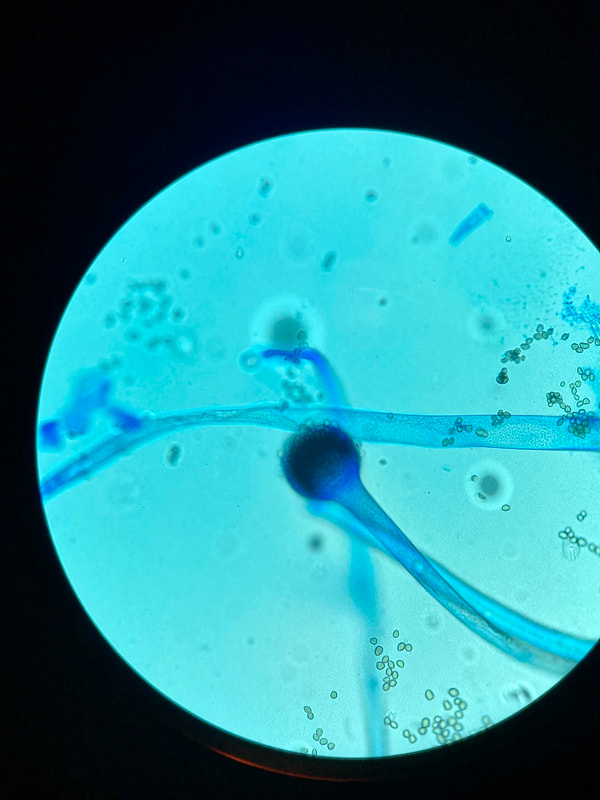
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
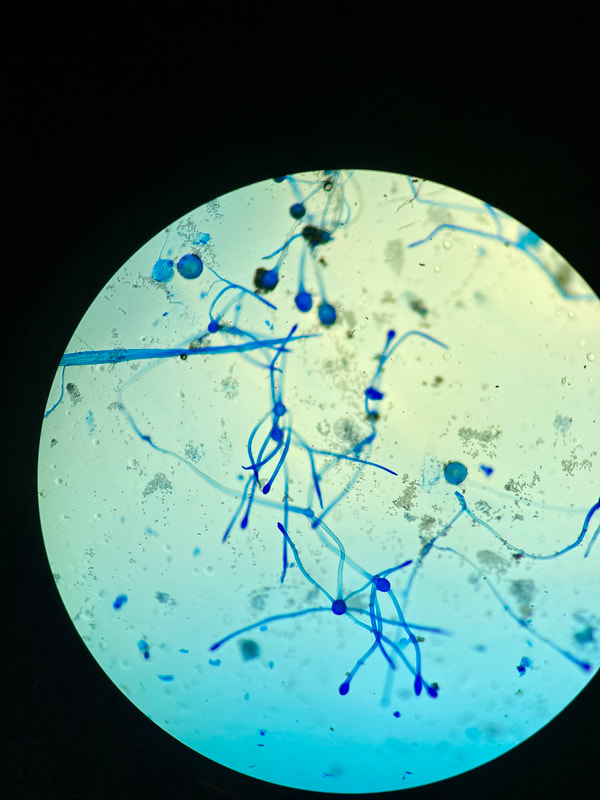
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
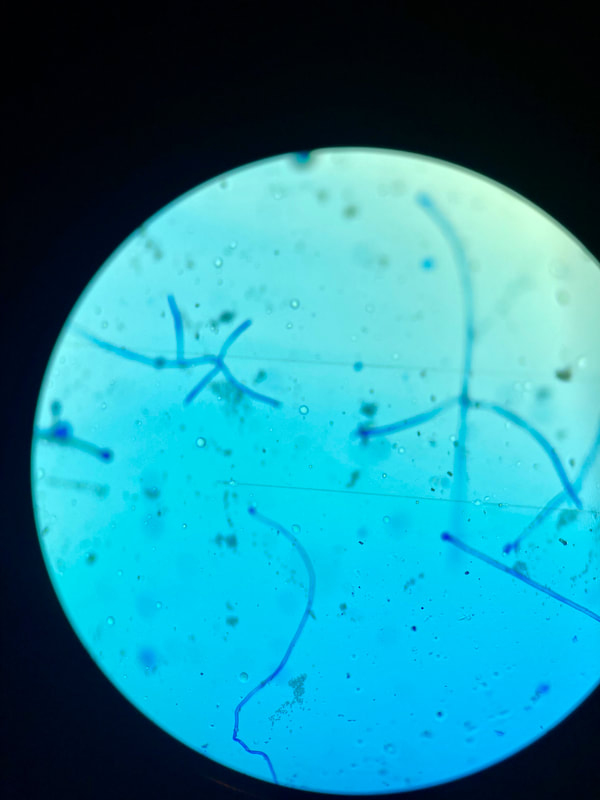
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
Rhizomucor spp
This is an etiologic agent of zygomycosis (rare pulmonary, disseminated or cutaneous) in immunocompromised individuals. This organism is associated with compost heaps.
This growth of Rhizomucor is rapid, maturing within 4 days. Growth of colonies is very fluffy and white like cotton candy. With age, growth turns gray to dark brown. The reverse is white.
|

This species appears as an intermediate between Rhizopus and Mucor, thereby the name Rhizomucor. The sporangia are similar to Rhizopus and Mucor, spherical and ranging from 60-100 microns in diameter. A few of the differentiating features include several short, irregularly branched rhizoids, which differentiate it from Mucor, which has no rhizoids. It differs from Rhizopus spp in that it has branched sporangiophores, whereas Rhizopus does not, and by the location of the rhizoids, which are located at areas on the stolon between the sporangiophores, rather then the sporangiophores originating from the rhizoids.
|

|
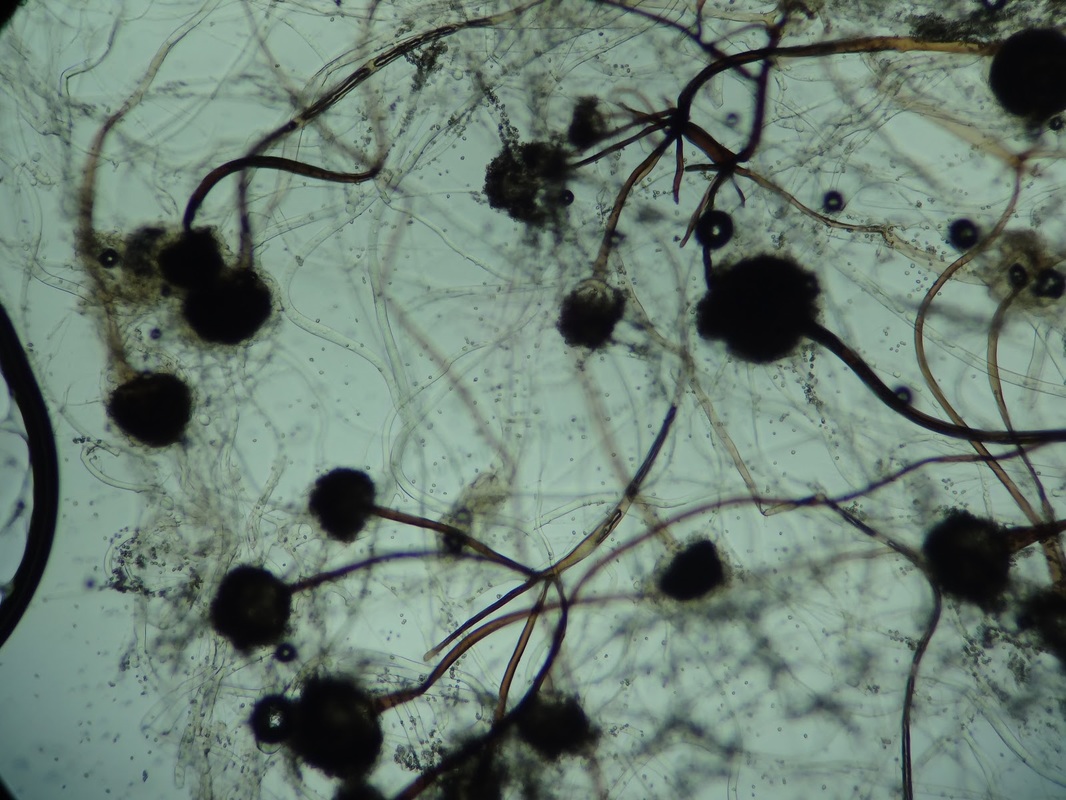
|
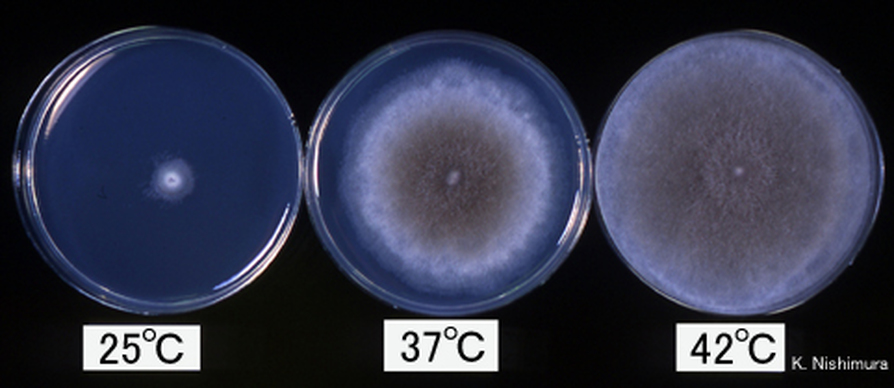
Rhizomucor spp temperature challenge
Saksenaea spp:
This organism was discovered in 1953. There are only two pathogenic species, but they can cause severe disease. On rare occasions, will cause zygomycosis and osteomyelitis, usually by traumatic implantation (injury, surgery). Other infections associated with this fungus are rhinocerebral, cranial, osteomyelitis, cutaneous and subcutaneous lesions. It may affect both immunocompetent and immunocompromised patients.
Macroscopic Exam:
On SABHI at room temperature, this fungus grows woolly white colonies.
Microscopic Exam:
This organism was discovered in 1953. There are only two pathogenic species, but they can cause severe disease. On rare occasions, will cause zygomycosis and osteomyelitis, usually by traumatic implantation (injury, surgery). Other infections associated with this fungus are rhinocerebral, cranial, osteomyelitis, cutaneous and subcutaneous lesions. It may affect both immunocompetent and immunocompromised patients.
Macroscopic Exam:
On SABHI at room temperature, this fungus grows woolly white colonies.
Microscopic Exam:
- Broad hyphae that are usually aseptate to sparsely septate and branched
- Flask-shaped sporangia
- Smooth, elongated sporangiopores
- Rhizoids are produced opposite the sporangiophores

This species is characterized by wide, broad, aseptate hyphae to sparsely septate hyphae and branched.
|

If grown on blocks of SABHI agar in distilled water-yeast extract medium at 37 degrees Celsius, flask-shaped sporangia will be observed, along with smooth, elongated sporangiospores. Root-like rhizoids, as seen in the image above, are produced opposite of the sporangiophores. Growth is rapid and fills the plate in just 4 days with a very cottony, fluffy white surface with a white reverse.
|
Cunninghamella spp:
This organism was discovered in 1903 by Alphonse Louis Paul Matruchot, but it was named after David Douglas Cunningham, a Scottish doctor and researcher who worked in India in public health and medicine. There are 13 species, and they contain carcinogens and mutagens that can cause cancer, birth defects, and change the DNA of cells.
This is the causative agent of zygomycosis in neutropenic patients, including pulmonary infections and disseminated infections, or mucormycosis in cancer patients, but otherwise a common contaminant.
Macroscopic Exam:
On SABHI agar, white cottony colonies grow well at room temperature, and they grow quickly, graying with age. Some species grwo at 37 and 42 degrees Celsius.
Microscopic Exam:
This organism was discovered in 1903 by Alphonse Louis Paul Matruchot, but it was named after David Douglas Cunningham, a Scottish doctor and researcher who worked in India in public health and medicine. There are 13 species, and they contain carcinogens and mutagens that can cause cancer, birth defects, and change the DNA of cells.
This is the causative agent of zygomycosis in neutropenic patients, including pulmonary infections and disseminated infections, or mucormycosis in cancer patients, but otherwise a common contaminant.
Macroscopic Exam:
On SABHI agar, white cottony colonies grow well at room temperature, and they grow quickly, graying with age. Some species grwo at 37 and 42 degrees Celsius.
Microscopic Exam:
- Aseptate hyphae
- Branched sporangiophores that terminate in vesicles (swollen cells)
- Sporangiola that form at the tips of swollen denticles
- Denticles: small, toothlike projections

The sporangiophores of this fungus end in spherical vesicles and spore-forming structures arise from these. On SABHI agar at room temperature, colonies grow as fluffy, white, cottony structures that grow quickly and mature within 4 days, graying with age. The reverse is white. The best growth is seen at 37 degrees Celsius. Hyphae are typically aseptate. The sporangiophores branch and terminate in vesicles.CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=476034
Syncephalastrum racemosum:
This is not known to be a human pathogen. It is considered a contaminant.
Macroscopic Exam:
This fungus grows as a woolly, cottony, white-to-dark colony that quickly matures within 3 days on SABHI agar at room temperature.
Microscopic Exam:
It is a filamentous fungi with a thick, aseptate sporangiophore and radial vesicles bearing spherical sporangiospores in rows within cylindrical merosporangia (specialized sporangia) that radiate around the surface of the vesicle like a flower. Sometimes, rudimentary rhizoids may be seen.
This is not known to be a human pathogen. It is considered a contaminant.
Macroscopic Exam:
This fungus grows as a woolly, cottony, white-to-dark colony that quickly matures within 3 days on SABHI agar at room temperature.
Microscopic Exam:
It is a filamentous fungi with a thick, aseptate sporangiophore and radial vesicles bearing spherical sporangiospores in rows within cylindrical merosporangia (specialized sporangia) that radiate around the surface of the vesicle like a flower. Sometimes, rudimentary rhizoids may be seen.

A beautiful fungus, round sporangiospores form in a nice row inside cylindrical merosporangia (specialized sporangia) that radiate around the whole surface of the vesicle
|

Syncephalastrum spp with aseptate, branching sporangiophore terminating in vesicles
|

This fungus has rudimentary rhizoids as well
|

|
Basidiobolus spp:
Conidiobolus coronatus:
ZYGOMYCOSIS, MUCORMYCOSIS, PHYCOMYCOSIS:
Zygomycosis is an acute fungal infection. It is caused by fungi from the phylum Zygomycota. This fungi is commonly seen growing on breads and fruits. Spores easily become airborne, and if the patient is immunocompromised, in diabetic ketoacidosis, is malnourished, or on corticosteroids, heavy antibiotics, or antileukemic drugs, the spores may infect the nasal sinuses and orbital eye area, rapidly spreading to nearby blood vessels, leading to necrosis and blood clot formation (vascular thrombosis). This can spread and disseminate systemically to the brain and meninges, quickly resulting in a fatal meningoencephalitis. It can spread to the lungs and the gastrointestinal tract as well. Death may occur in just 2-10 days after initial sinus or eye infection with the organism, which has a high fatality rate since it can rapidly spread. It is fatal in 15% of skin cases, 50% of sinus cases, 66% of lung cases, and nearly all systemic cases.
Chronic zygomycosis is a more self-limiting form that may occur in subcutaneous lesion infections, or may progress to a more serious acute progressive cellulitis of the legs in diabetic patients. Direct wet mounts of specimens in this category show branching, large, aseptate hyphae and round sporangia and/or columellas and/or collarettes. Repeated isolation of the organism may confirm the diagnosis, as may sending out the culture for molecular speciation. Zygomycosis of the sinuses, orbital areas and meninges is rapidly fatal, so early treatment is key. Treatment typically begins with amphotericin B and sometimes includes surgery to remove infected tissue via debridement, as well as surgical drainage.
Cutaneous zygomycosis results in the formation of a black eschar lesion (painful, necrotic) and a fever. Those at highest risk are those with diabetes and those with malignancies. Those at highest risk for the pulmonary form are those with lung transplants, which can be invasive and fatal. Those at highest risk for rhinocerebral types include those with paranasal swellin with necrotic tissues and bloody exudate.
Diagnosis is by Kott prep, fungal culture, X-rays revealing 10+ nodules and pleural effusion, and CT scans revealing a halo sign.
Zygomycosis is an acute fungal infection. It is caused by fungi from the phylum Zygomycota. This fungi is commonly seen growing on breads and fruits. Spores easily become airborne, and if the patient is immunocompromised, in diabetic ketoacidosis, is malnourished, or on corticosteroids, heavy antibiotics, or antileukemic drugs, the spores may infect the nasal sinuses and orbital eye area, rapidly spreading to nearby blood vessels, leading to necrosis and blood clot formation (vascular thrombosis). This can spread and disseminate systemically to the brain and meninges, quickly resulting in a fatal meningoencephalitis. It can spread to the lungs and the gastrointestinal tract as well. Death may occur in just 2-10 days after initial sinus or eye infection with the organism, which has a high fatality rate since it can rapidly spread. It is fatal in 15% of skin cases, 50% of sinus cases, 66% of lung cases, and nearly all systemic cases.
Chronic zygomycosis is a more self-limiting form that may occur in subcutaneous lesion infections, or may progress to a more serious acute progressive cellulitis of the legs in diabetic patients. Direct wet mounts of specimens in this category show branching, large, aseptate hyphae and round sporangia and/or columellas and/or collarettes. Repeated isolation of the organism may confirm the diagnosis, as may sending out the culture for molecular speciation. Zygomycosis of the sinuses, orbital areas and meninges is rapidly fatal, so early treatment is key. Treatment typically begins with amphotericin B and sometimes includes surgery to remove infected tissue via debridement, as well as surgical drainage.
Cutaneous zygomycosis results in the formation of a black eschar lesion (painful, necrotic) and a fever. Those at highest risk are those with diabetes and those with malignancies. Those at highest risk for the pulmonary form are those with lung transplants, which can be invasive and fatal. Those at highest risk for rhinocerebral types include those with paranasal swellin with necrotic tissues and bloody exudate.
Diagnosis is by Kott prep, fungal culture, X-rays revealing 10+ nodules and pleural effusion, and CT scans revealing a halo sign.
SEPTATE OPPORTUNISTS:
The septate opportunists are characterized by hyphae with septate cross-walls. Medically significant septate opportunists are from the phylum Deuteromycota and are divided into two categories:
1) Dematiaceous (dark-colored hyphae and/or conidia)
-Dark green to black colonies, even on the reverse
2) Hyaline (light-color hyphae and/or conidia)
-A tease mount is required because light-colored aerial hyphae may be covered over with brightly colored conidia
I. DEMATIACEOUS OPPORTUNISTS:
The dematiaceous opportunistic molds are the causative agents of phaeohyphomycosis, chromoblastomycosis and eumycotic mycetoma. Think of these are dark, dangerous and even deadly.
The term "dematiaceous" means molds that are dark (brown or black, sometimes gray or olive colonies) and produce dark hyphae and structures microscopically. This is due to the amount of melanin pigment in their cell walls. They darken with age, can produce dangerous infections that persist or come back, and they can disseminate (spread). Severe dissemination can occur with certain types of phaeohyphomycosis linked to Cladophialophora spp, resulting in CNS symptoms, such as brain abscess, epilepsy, and meningitis, all of which can be fatal if left untreated or if spread to the cerebrum occurs from the scalp.
Alternaria spp:
Alternaria species is a member of the ascomycete fungi family. It is a major plant pathogen, particularly of tomato plants. Most of the time, this is considered a contaminant, but it can be a causative agent of phaeohyphomycosis (keratomycosis, osteomyelitis, pulmonary disease, nasal septum infection, skin infections), particularly in immunocompromised patients, such as those with HIV/AIDS. It is a potent allergen for some individuals, resulting in hay fever or sinusitis. It can also provoke asthma attacks in susceptible individuals. It is difficult to avoid, since it is ubiquitous (everywhere), and there are around 299 species. It is a common cause of decay of vegetation and is a decomposer. Spores are released airborne and are found on surfaces and water.
Macroscopic Exam:
Mold colonies are green, black or gray on agar (SABHI), with a black reverse.
Microscopic Exam:
The septate opportunists are characterized by hyphae with septate cross-walls. Medically significant septate opportunists are from the phylum Deuteromycota and are divided into two categories:
1) Dematiaceous (dark-colored hyphae and/or conidia)
-Dark green to black colonies, even on the reverse
2) Hyaline (light-color hyphae and/or conidia)
-A tease mount is required because light-colored aerial hyphae may be covered over with brightly colored conidia
I. DEMATIACEOUS OPPORTUNISTS:
The dematiaceous opportunistic molds are the causative agents of phaeohyphomycosis, chromoblastomycosis and eumycotic mycetoma. Think of these are dark, dangerous and even deadly.
The term "dematiaceous" means molds that are dark (brown or black, sometimes gray or olive colonies) and produce dark hyphae and structures microscopically. This is due to the amount of melanin pigment in their cell walls. They darken with age, can produce dangerous infections that persist or come back, and they can disseminate (spread). Severe dissemination can occur with certain types of phaeohyphomycosis linked to Cladophialophora spp, resulting in CNS symptoms, such as brain abscess, epilepsy, and meningitis, all of which can be fatal if left untreated or if spread to the cerebrum occurs from the scalp.
Alternaria spp:
Alternaria species is a member of the ascomycete fungi family. It is a major plant pathogen, particularly of tomato plants. Most of the time, this is considered a contaminant, but it can be a causative agent of phaeohyphomycosis (keratomycosis, osteomyelitis, pulmonary disease, nasal septum infection, skin infections), particularly in immunocompromised patients, such as those with HIV/AIDS. It is a potent allergen for some individuals, resulting in hay fever or sinusitis. It can also provoke asthma attacks in susceptible individuals. It is difficult to avoid, since it is ubiquitous (everywhere), and there are around 299 species. It is a common cause of decay of vegetation and is a decomposer. Spores are released airborne and are found on surfaces and water.
Macroscopic Exam:
Mold colonies are green, black or gray on agar (SABHI), with a black reverse.
Microscopic Exam:
- Dematiaceous (dark) raquet-shaped hyphae or club-shaped spores that may alternate and form long chains (poroconidia) with horizontal and vertical septa
- They have club-shaped bases with apices that are tapered.
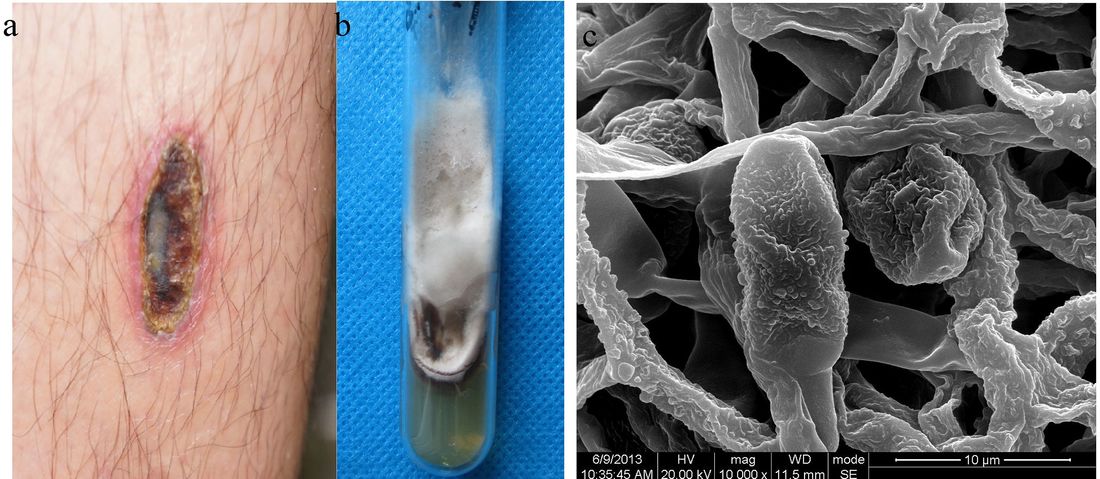
This image shows a cutaneous (skin) infection caused by Alternaria species;By Ran Yuping et al. - [1], CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=52253227
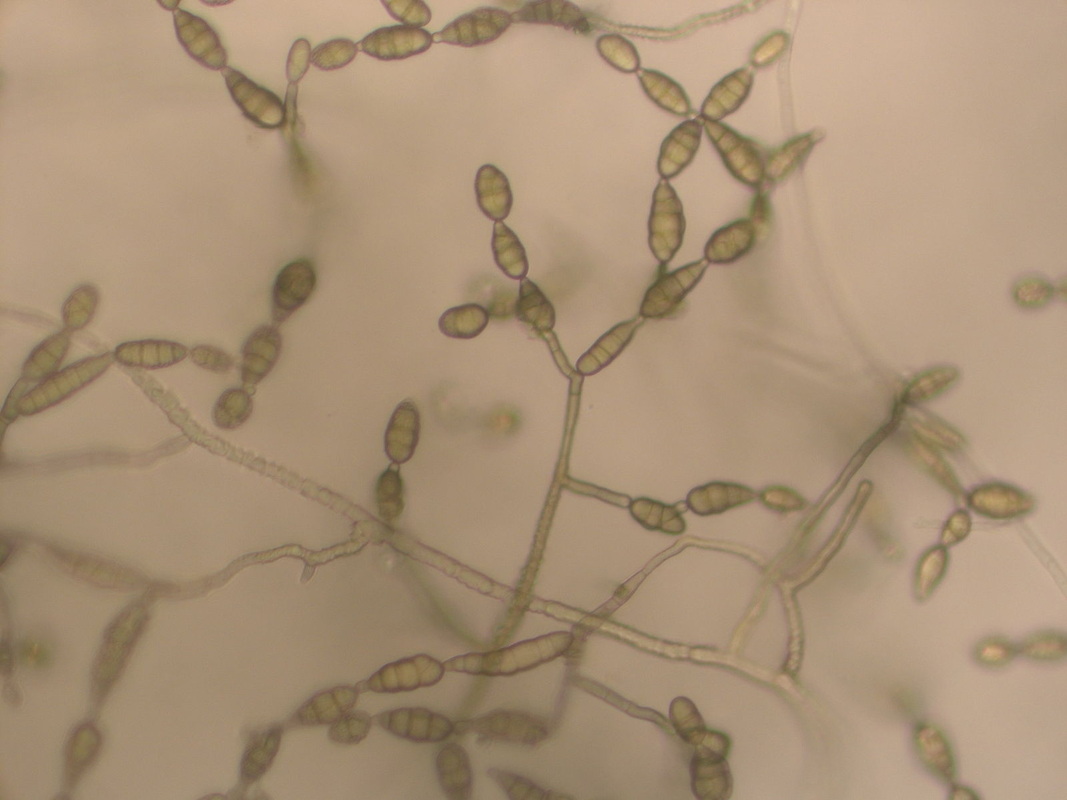
The septate hyphae contain both horizontal and vertical septa in this image of A. alternata;By Vanluubio (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
|
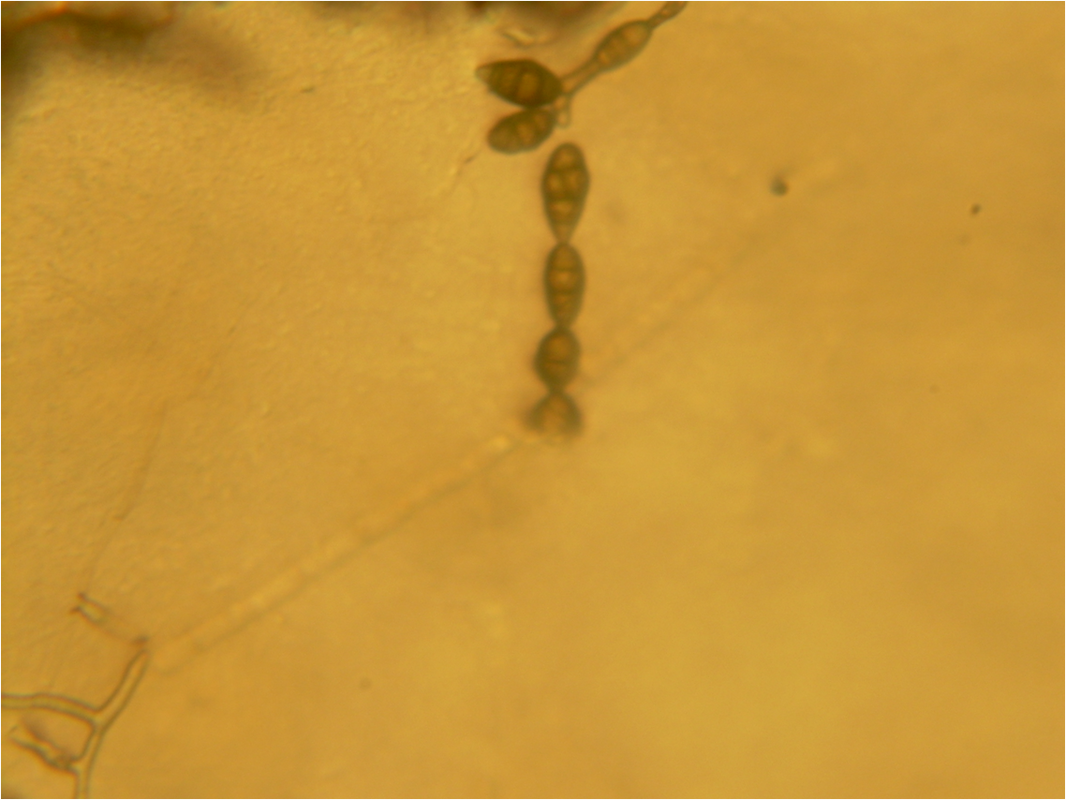
Chained poroconidia of A. alternata are observed here (racquet hyphae);By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6657550
|
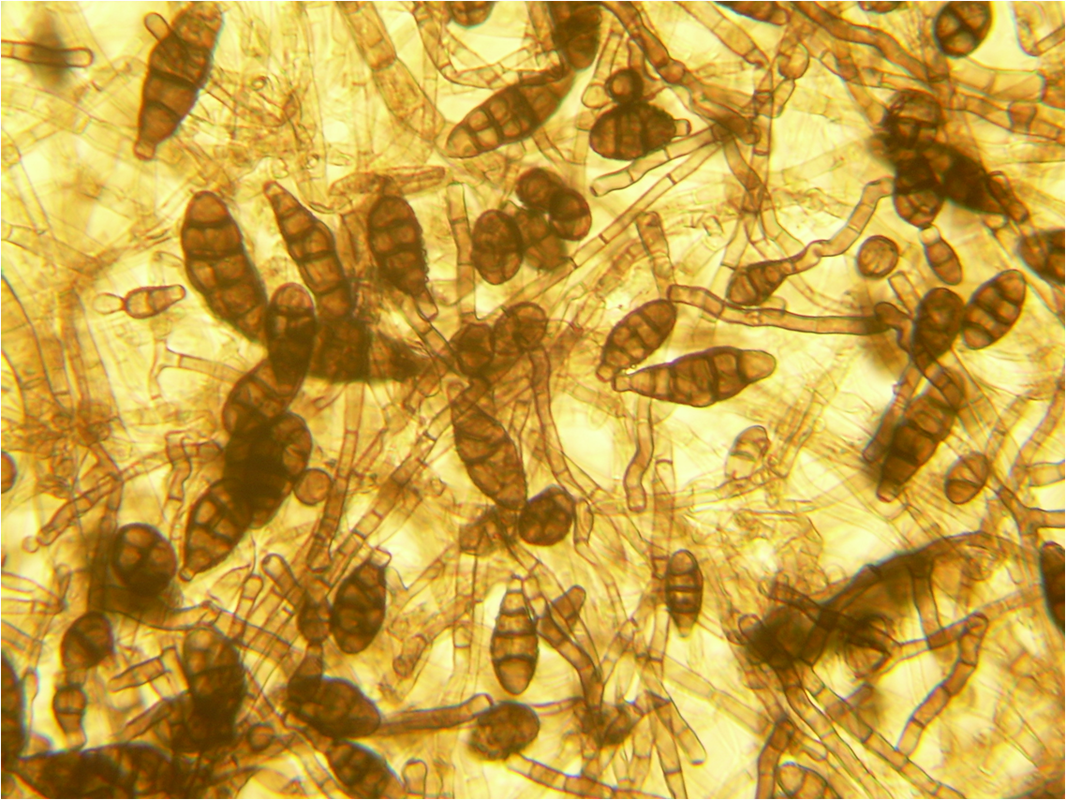
Club-shaped bases with tapered apices characterize the poroconidia of Alternaria alternata;By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
|
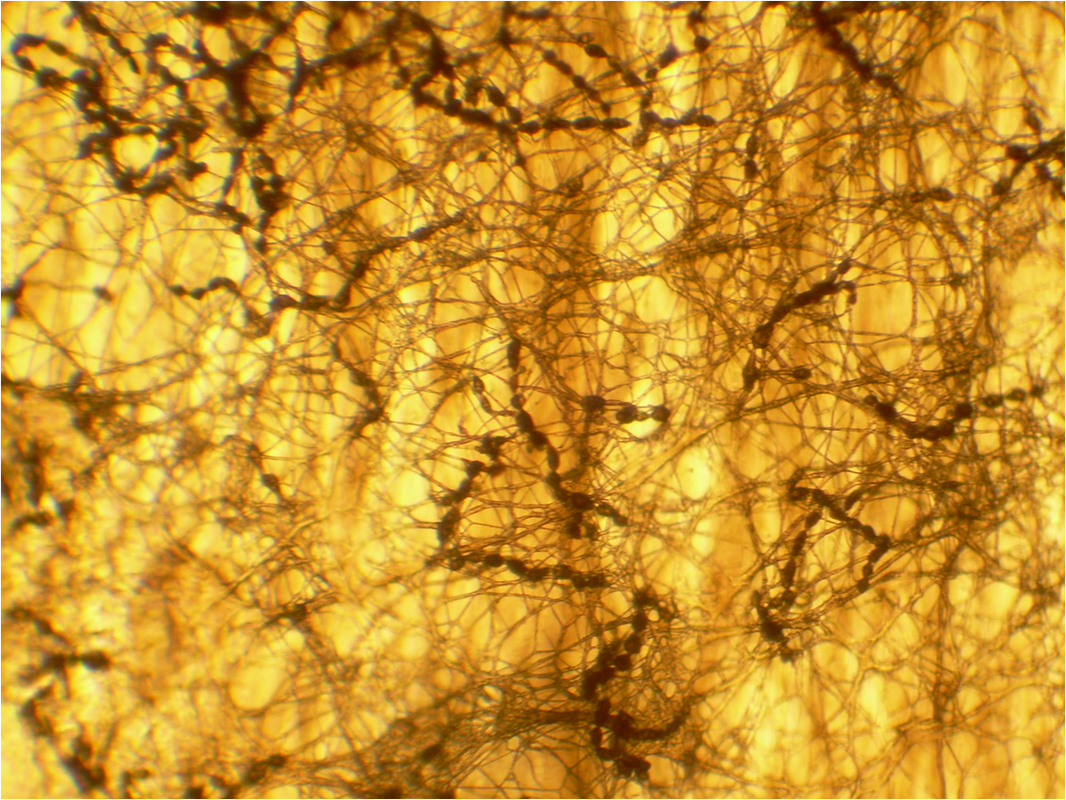
As seen here, the hyphae and conidia of Alternaria alternata are DARK.By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6657601
|

By Abdulghafour - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=40158030
|

Club-shaped bases with tapered apices;By Vanluubio - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=23688310
|
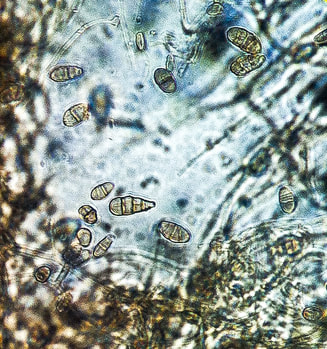
By Alepopoli (Own work) [CC BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0)], via Wikimedia Commons
|

Alternaria produces "racquet hyphae"; CDC, Dr. Lucille K. George, 1955,https://phil.cdc.gov/Details.aspx?pid=3963
|

Racquet hyphae, CDC, Dr. Lucille K. George, 1955,https://phil.cdc.gov/Details.aspx?pid=3962
|
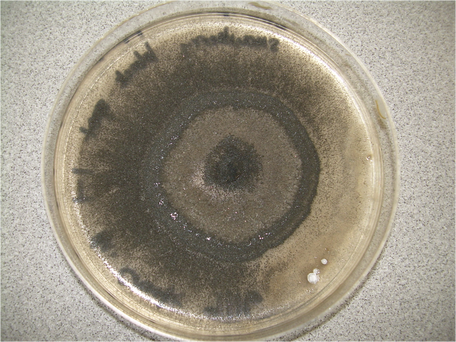
At room temperature, on SABHI agar, Alternaria spp grows as a light gray, woolly colony that quickly matures within 5 days to dark greenish black or brown, with a black reverse;By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6657734
|
Alternaria spp on Potato Flake Agar, producing a velvety brown colony with white border and umbonate center
|

By Seemadua, S. Department of Agriculture, Thailand [CC BY 3.0 au (http://creativecommons.org/licenses/by/3.0/au/deed.en)], via Wikimedia Commons
Aureobasidium spp:
This organism is a common contaminant, but can be a causative agent of foot or leg lesions, allergies, cheloid blastomycosis. This is a black yeast-like mold that can contaminate air conditioners and humidifiers, causing human disease such as human pneumonitis, allergic alveolitis, with cough, shortness of breath, fever, chest infiltrates, and inflammation. It can also become chronic in susceptible individuals. Sometimes, colonies will appear smooth and creamy with mycelium.
Macroscopic Exam:
Microscopic Exam:
This organism is a common contaminant, but can be a causative agent of foot or leg lesions, allergies, cheloid blastomycosis. This is a black yeast-like mold that can contaminate air conditioners and humidifiers, causing human disease such as human pneumonitis, allergic alveolitis, with cough, shortness of breath, fever, chest infiltrates, and inflammation. It can also become chronic in susceptible individuals. Sometimes, colonies will appear smooth and creamy with mycelium.
Macroscopic Exam:
- Colonies are shiny white and yeast-like at first, becoming shiny black and leathery with a white fringe with age
Microscopic Exam:
- Light or dark brown conidiophores
- Short denticles support hyaline single or clustered conidia
- Secondary blastoconidia
- Conidiophores darken with age with one or two-celled arthroconidia

Image by Jeanette Sprute, MT-AMT, M-ASCP (cm), 2015, own work
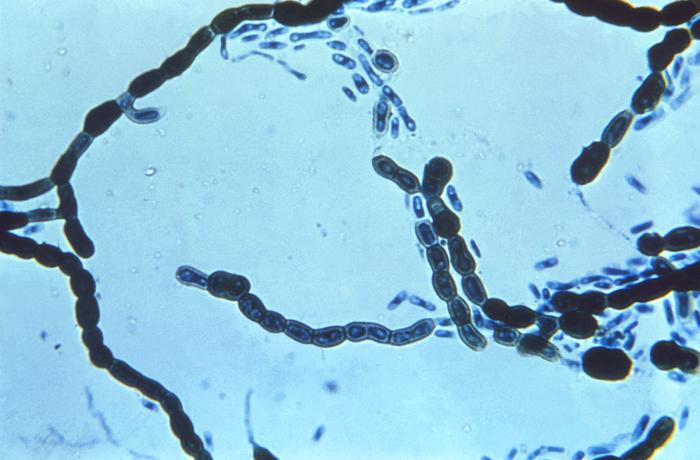
https://phil.cdc.gov/Details.aspx?pid=15682
|

https://phil.cdc.gov/Details.aspx?pid=15683
|
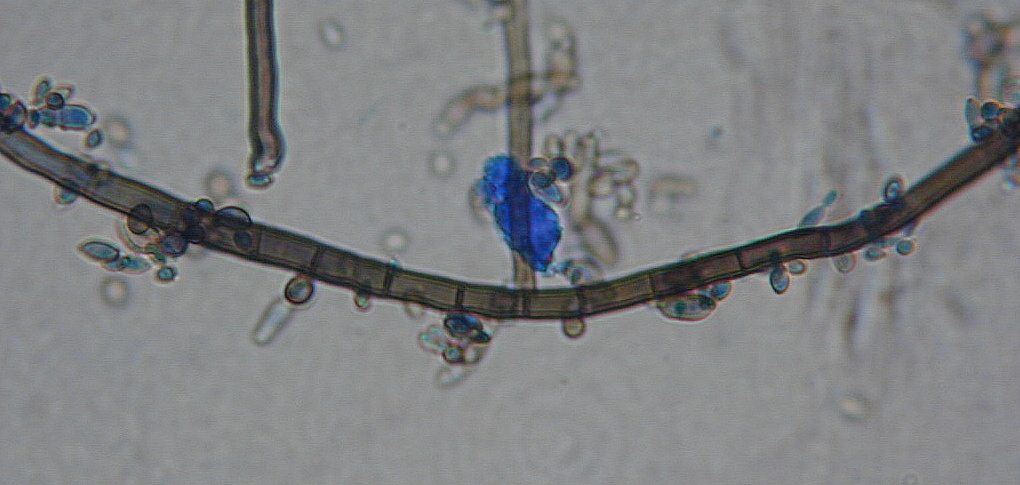
LPCB stain wet mount of Auerobasidium spp, indicating hyaline blastoconidia and dark arthroconidia is seen here. Immature colonies are observed as unicellular budding, yeast-like cells. Two types of hyphae are observed: 1) hyaline, fragile, thin-walled, with conidia produced directly from the walls at various points and 2) dark, thick-walled, septate hyphae as seen above with some of the cells producing short tubes that bear conidia, which are hyaline and oval in shape and keep multiplying by budding.By This image was created by user Tom Volk (TomVolk) at Mushroom Observer, a source for mycological images.You can contact this user here. - This image is Image Number 44026 at Mushroom Observer, a source for mycological images.This tag does not indicate the copyright status of the attached work. A normal copyright tag is still required. See Commons:Licensing for more information., CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=11723488
|
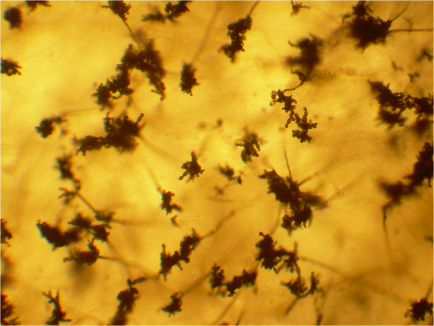
Light to dark brown condiophores and short denticles support singular hyaline or clustered conidia, with the formation of secondary blastoconidia.By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
|

Aureobasidium spp;By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
|

With age, condiophores darken and become one-to-two-celled arthroconidia;By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6658105
|
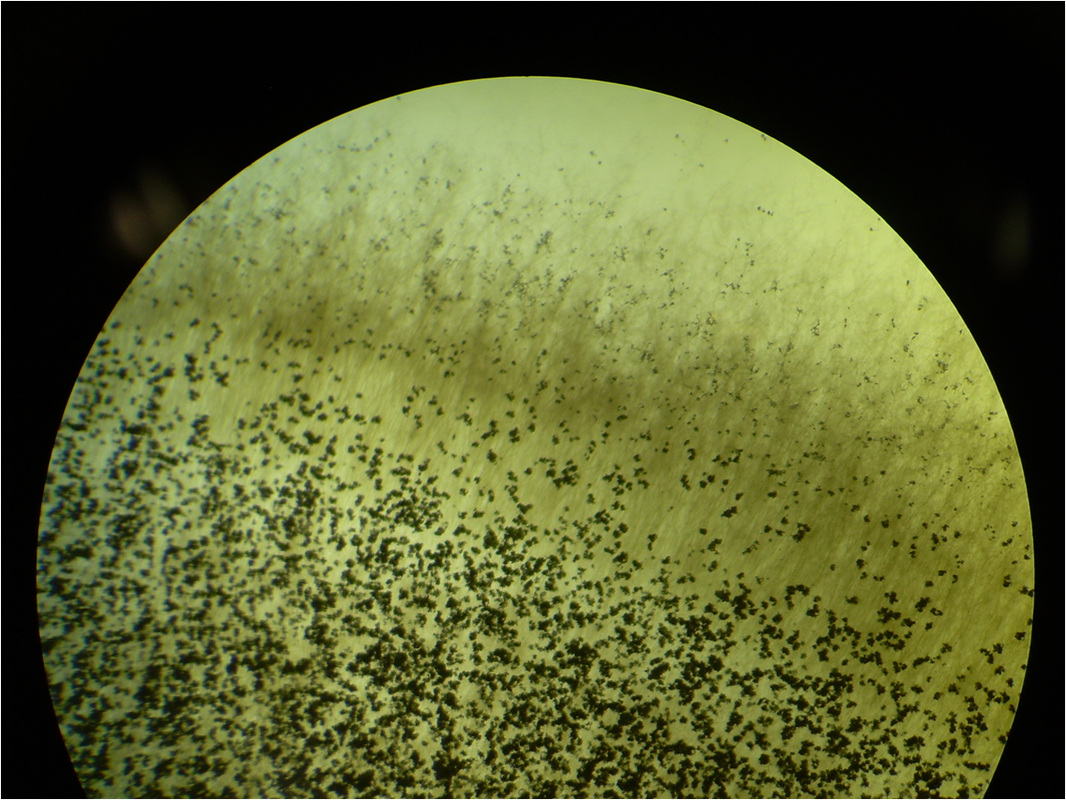
Aerial hyphae with black conidia;By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
|
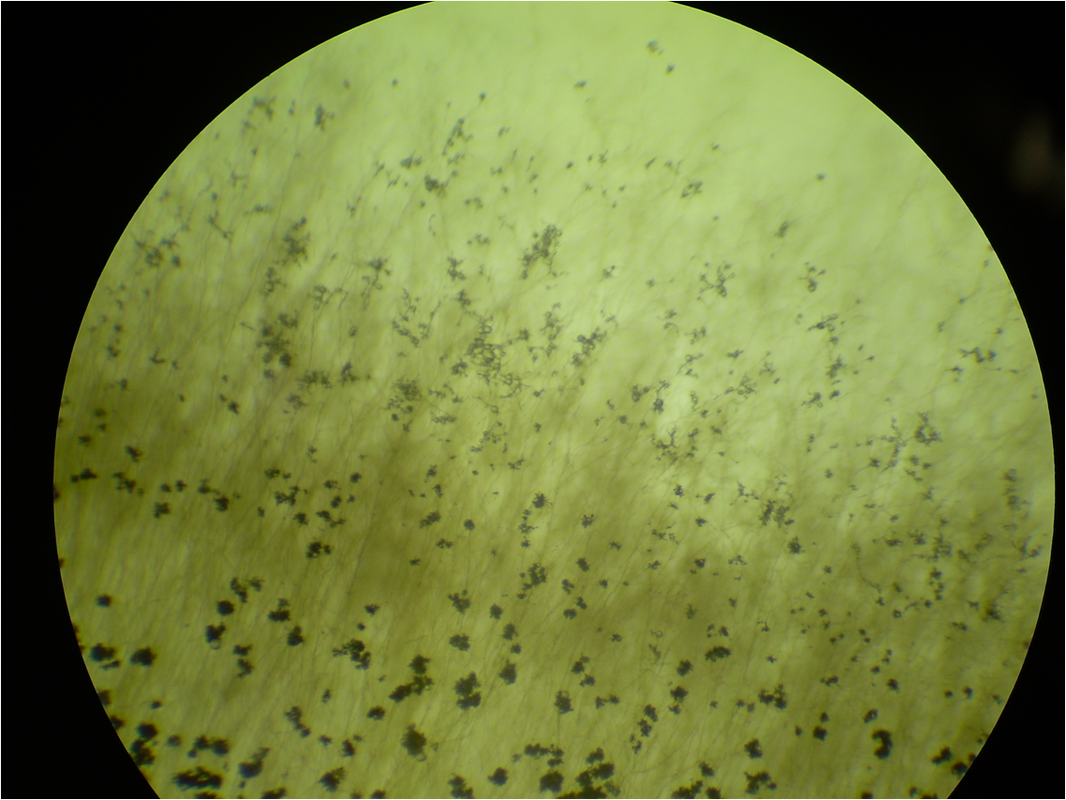
Light-to-dark conidiophores;By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6658019
|
On SABHI at room temperature, initially, colonies of Aureobasidium grow at a moderately rapid rate as shiny white and similar to yeast in appearance. However, with age, they become shiny black with a leathery texture and a white edge. The reverse is black. This is a BLACK YEAST.By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
Bipolaris spp:
Bipolaris species is a plant pathogen that causes cactus stem rot and rots other plants as well. In humans, it is a causative agent of keratomycosis, fungal sinusitis, subcutaneous abscesses, phaeohyphomycosis, meningitis, allergies, or peritonitis. May simply be a contaminant in a clinical specimen as well. Infections are treated with long-term Amp B therapy.
Macroscopic Exam:
Microscopic Exam:
Bipolaris species is a plant pathogen that causes cactus stem rot and rots other plants as well. In humans, it is a causative agent of keratomycosis, fungal sinusitis, subcutaneous abscesses, phaeohyphomycosis, meningitis, allergies, or peritonitis. May simply be a contaminant in a clinical specimen as well. Infections are treated with long-term Amp B therapy.
Macroscopic Exam:
- Look for rapid-growing colonies that are velvety or woolly and gray-brown in color with a center that is black and matted.
- The reverse is light or dark.
Microscopic Exam:
- Septate hyphae are dark.
- It produces zig-zag shaped conidiophores bearing numerous elongated poroconidia with 3-5 thick-walled septations.
- Poroconidia have truncate hila (points of attachment) in clusters along a bent-knee shaped conidiophore
- Germination: germ tubes may arise from one or both poles (ends) and grow along the axis of the conidium

This LPCB wet mount shows Bipolaris spp, characterized by septate hyphae with numerous dark, cylindrical 4-5-celled poroconidia with points of attachment referred to as truncate hila. Image CDC, 1971,https://phil.cdc.gov/Details.aspx?pid=4338
|

When poroconidia such as these germinate, they may form a germ tube from one or both ends (poles) and grow along the conidial axis
|

Bipolaris Species, CDC, 1971;https://phil.cdc.gov//phil_images/20030725/36/PHIL_4318.tif
|
At room temperature on SABHI agar, Bipolaris spp grows very quickly as a velvety or woolly colony that appears grayish-brown at first, maturing to a matted, black center, with a light or dark reverse.
|
Bipolaris app growing on Potato Flake Agar, CDC, 1971;https://phil.cdc.gov/Details.aspx?pid=10605
|

Bipolaris spp, CDC, 1971;https://phil.cdc.gov/Details.aspx?pid=10606
|
https://phil.cdc.gov/Details.aspx?pid=10606
|
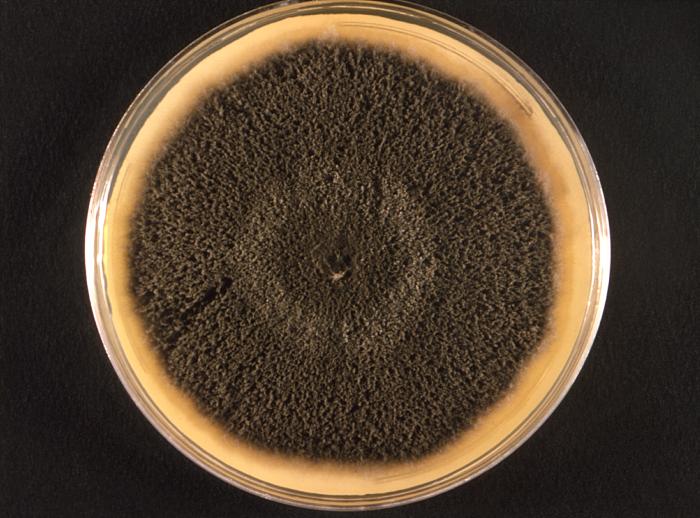
https://phil.cdc.gov/Details.aspx?pid=10604
|
Cladosporium spp: (Many have been renamed to Cladophialophora spp)
Cladosporium spp is a common mold and the causative agent of keratomycosis and allergies, asthma attacks, rare skin infections, rare nail infections, sinus infections, lung infections. It is one of the most common indoor and outdoor molds. It is found often on both living and dead plant material. Some are plant pathogens and some are parasites of other types of fungi. It produces yellow, brown, and green spots on plants where moisture is present. There are more than 40 known species. This organism thrives in moisture/humidity, and can cause "sick building syndrome" and mold toxicity with health problems.
Cladosporium
Cladophialophora carrionii, Cladophialophora boppii, Cladophialophora bantiana
It grows slowly on SABHI agar at room temperature, requiring 7 days to grow. It is a widespread organism that is found everywhere, but it can affect air quality and have long-term health effects.
Macroscopic Exam:
Microscopic Exam:
Cladosporium spp is a common mold and the causative agent of keratomycosis and allergies, asthma attacks, rare skin infections, rare nail infections, sinus infections, lung infections. It is one of the most common indoor and outdoor molds. It is found often on both living and dead plant material. Some are plant pathogens and some are parasites of other types of fungi. It produces yellow, brown, and green spots on plants where moisture is present. There are more than 40 known species. This organism thrives in moisture/humidity, and can cause "sick building syndrome" and mold toxicity with health problems.
Cladosporium
Cladophialophora carrionii, Cladophialophora boppii, Cladophialophora bantiana
It grows slowly on SABHI agar at room temperature, requiring 7 days to grow. It is a widespread organism that is found everywhere, but it can affect air quality and have long-term health effects.
Macroscopic Exam:
- It produces powdery, velvety, heaped and folded dark, gray-green colonies with a black reverse.
Microscopic Exam:
- It produces septate hyphae that are dark.
- It produces short chains of dark, 1-4-celled blastoconidia with a distinct scar at each point of attachment.
- Blastoconidia are borne from repeatedly forking shield cells (shield-shaped conidiogenous parent cells).

Image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|

Image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|
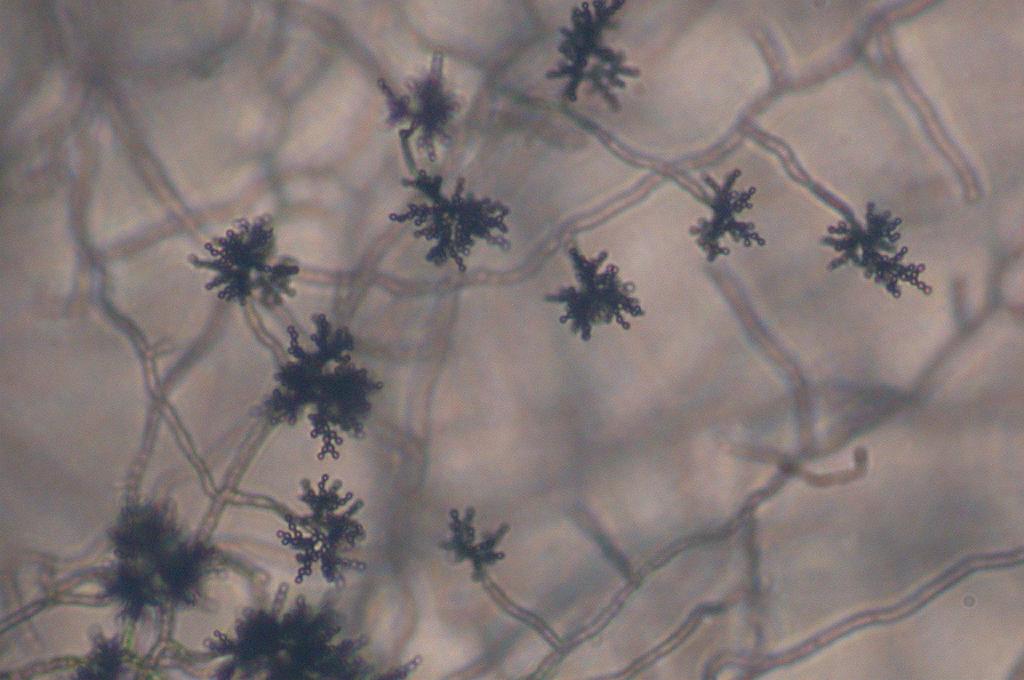
Dark-colored septate hyphae characterize the Cladosporium spp, along with short chains of 1-4-celled blastoconidia characterized by a distinct "scar" at the point of attachment, which arise from repeats of "forking shield cells" shaped like shields.CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=730537
|
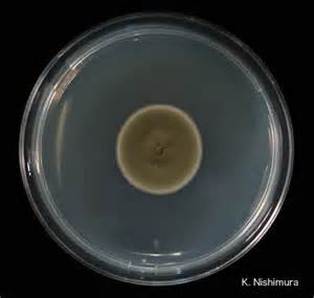
At room temperature, on SABHI agar, Cladosporium spp slowly grows as a powdery or velvety, heaped and folded colony (verrucose), and dark or gray-green with a black reverse. It takes about 7 days for this one to grow.
|

|
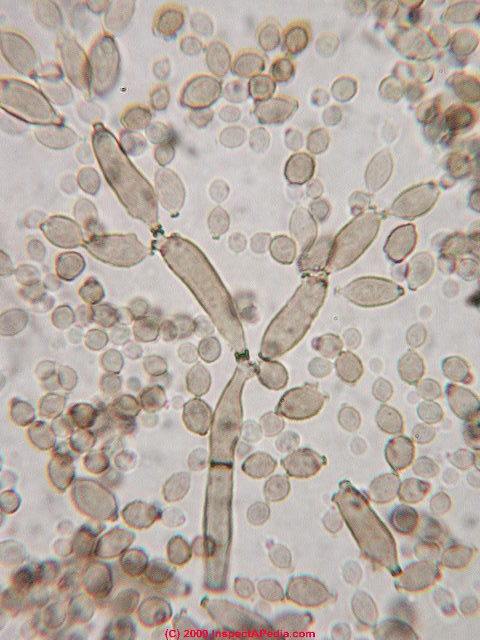
Known for its septate hyphae bearing "shield cells" and conidia that are lemon-shaped with dark spots (hila) at their base where they connect to the conidiophore or other conidia
|


By Medmyco (Own work) [CC BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0)], via Wikimedia Commons
|
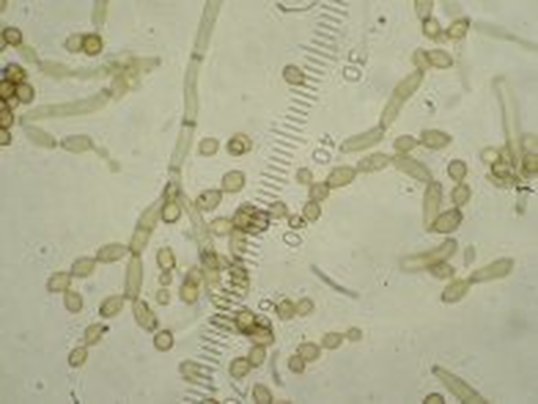
|
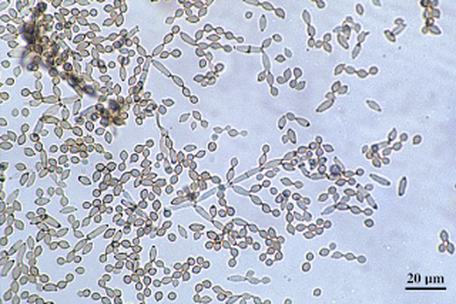
|

|

|
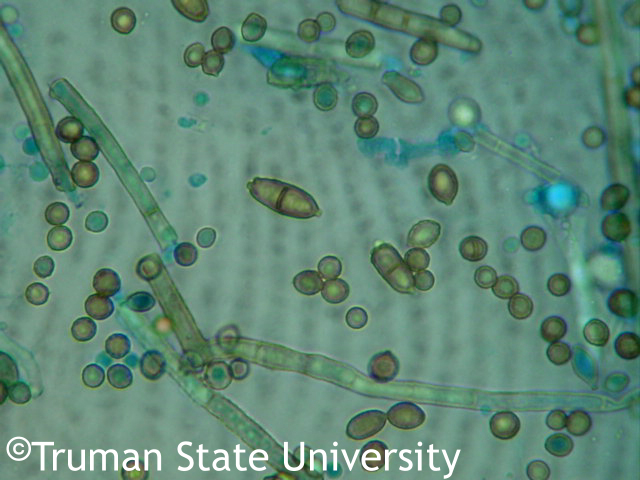
|
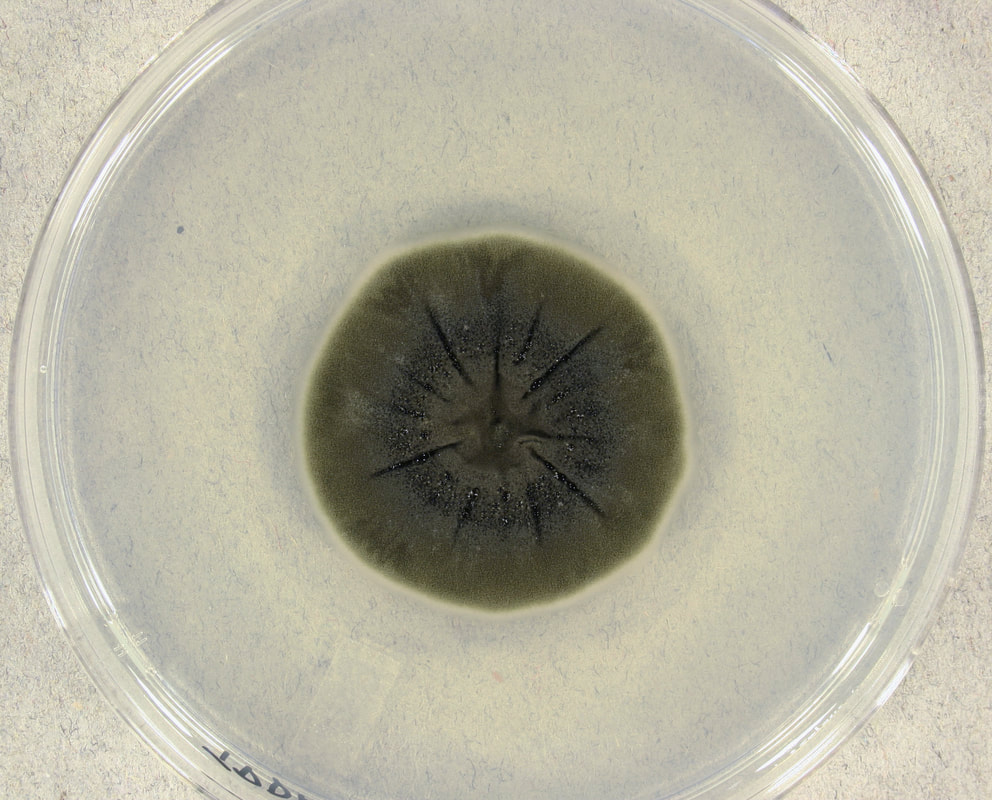
By Medmyco (Own work) [CC BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0)], via Wikimedia Commons
|

Cladosporium spp, a rugose, umbonate colony that is tan-brown in color with a dark reverse; image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|
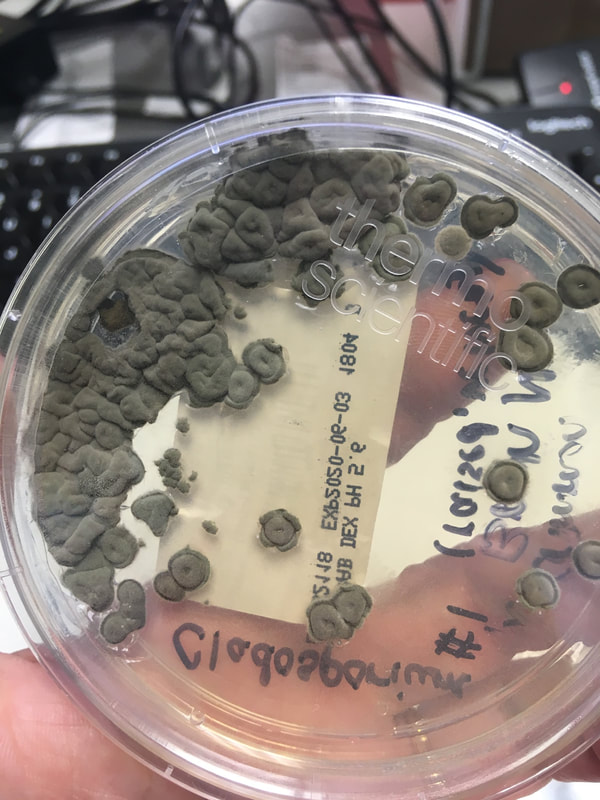
Images of Cladosporium, by Jeanette Reynolds, MS-Biology, MLS-AMT, M-ASCP, certified in emerging diseases, certified instructor, MLS LMC (own work)
|

Images of Cladosporium, by Jeanette Reynolds, MS-Biology, MLS-AMT, M-ASCP, certified in emerging diseases, certified instructor, MLS LMC (own work)
|
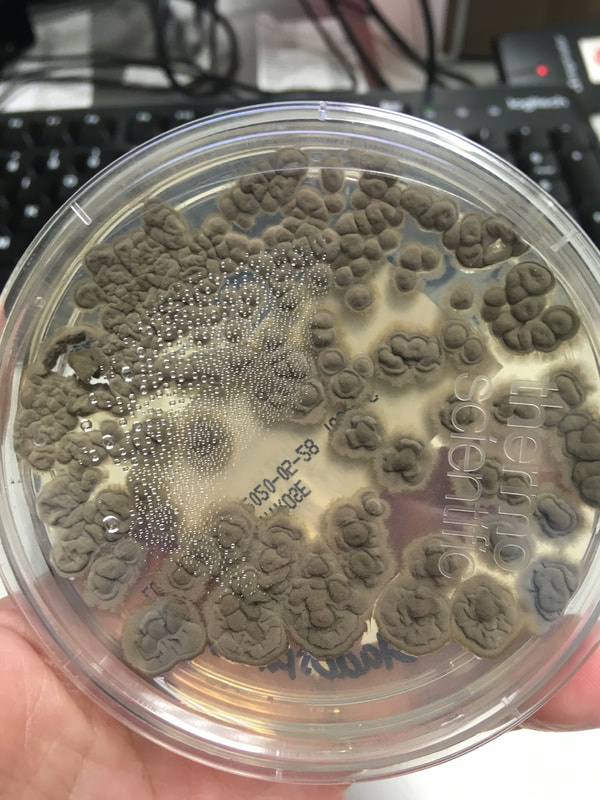
Images of Cladosporium, by Jeanette Reynolds, MS-Biology, MLS-AMT, M-ASCP, certified in emerging diseases, certified instructor, MLS LMC (own work)
|
Cladophialophora spp:
This is one of the most common causative agents of chromoblastomycosis worldwide. The main cause is C. carionii. It produces granules that bear sclerotic bodies resembling "copper pennies" in tissue stains. Microscopically, it looks like Cladosporium spp, from which it was renamed, with chains of lemon-shaped conidia born on branched conidiophores on septate hyphae. The short conidiophores resemble "shields" and are referred to as "shield cells". C. bantiana is the most common cause of cerebral phaeohyphomycosis, which affects the CNS, resulting in brain abscess, epilepsy and meningitis and is fatal if left untreated. Always work with these suspect cultures under the biological safety hood and do not make slide cultures!
This is one of the most common causative agents of chromoblastomycosis worldwide. The main cause is C. carionii. It produces granules that bear sclerotic bodies resembling "copper pennies" in tissue stains. Microscopically, it looks like Cladosporium spp, from which it was renamed, with chains of lemon-shaped conidia born on branched conidiophores on septate hyphae. The short conidiophores resemble "shields" and are referred to as "shield cells". C. bantiana is the most common cause of cerebral phaeohyphomycosis, which affects the CNS, resulting in brain abscess, epilepsy and meningitis and is fatal if left untreated. Always work with these suspect cultures under the biological safety hood and do not make slide cultures!
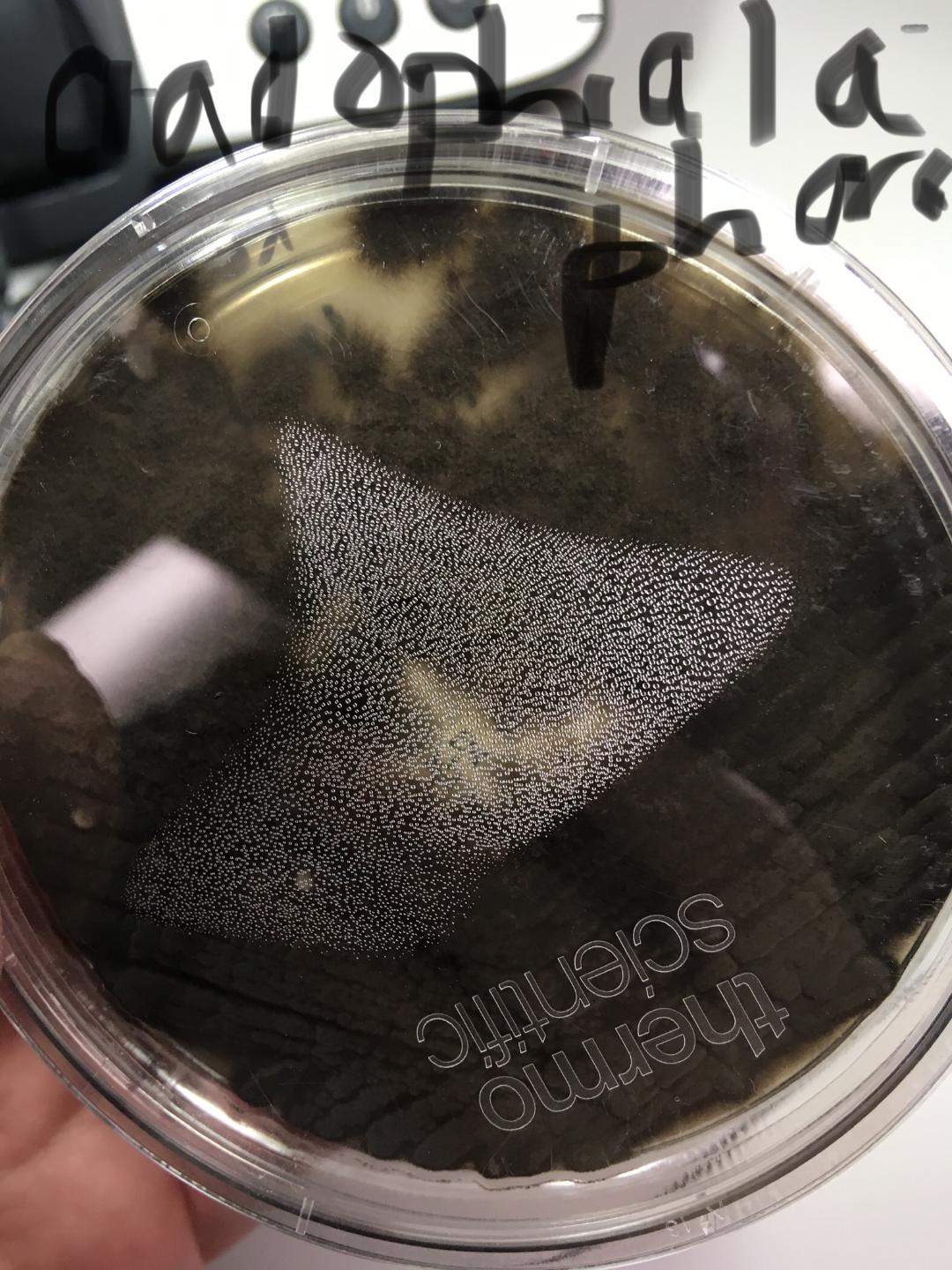
Image by Jeanette Reynolds, MS-Biology, M (ASCP) cm, MLS-AMT, certified instructor, certified in emerging infectious diseases, MLS II, Microbiology Lab/Mycology/AFB, 2020 (undisclosed location)
|
Image by Jeanette Reynolds, MS-Biology, M (ASCP) cm, MLS-AMT, certified instructor, certified in emerging infectious diseases, MLS II, Microbiology Lab/Mycology/AFB, 2020 (undisclosed location)
|
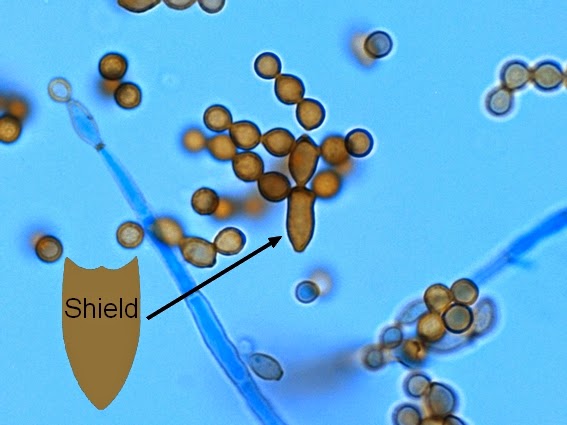
Image by Yuri, "Fun With Microbiology (What's Buggin' You), thunderhouse4-yuri.blogspot.com
|
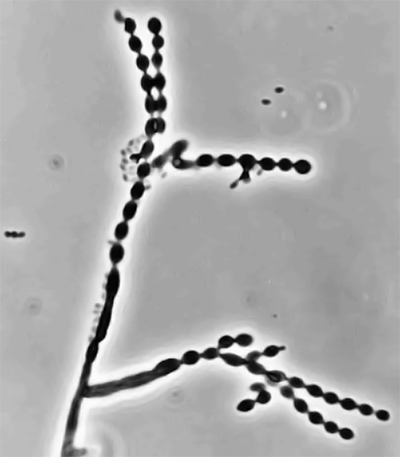
https://upload.wikimedia.org/wikipedia/commons/7/78/Cladophialophora_carrionii.jpg
|
Curvularia spp: "LOVE THOSE CURVES"
This is the causative agent of keratomycosis, mycetoma, endocarditis, pulmonary infection, allergies, or infection of the nasal septum in humans, and is a plant pathogen.
Macroscopic Exam:
Microscopic Exam:
This is the causative agent of keratomycosis, mycetoma, endocarditis, pulmonary infection, allergies, or infection of the nasal septum in humans, and is a plant pathogen.
Macroscopic Exam:
- On SABHI agar, it is a rapid-grower
- It produces cottony, white, light pink, orange, or green colonies with a brown reverse.
Microscopic Exam:
- It produces dark, septate mycelium.
- It produces 4-5-celled, large, dark poroconidia.
- Poroconidia are borne on a bent-knee-shaped conidiophore.
- Poroconidia are centrally distended due to an over-enlarged central cell, with ends that are lighter than the middle, making it resemble "curved" orange slices or orange slice candy.

Images of Cladosporium, by Jeanette Reynolds, MS-Biology, MLS-AMT, M-ASCP, certified in emerging diseases, certified instructor, MLS LMC (own work)

The septate mycelium of the Curvularia spp are dark.By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
|

Curvularia spp are characterized by large, 4-5-celled, dark poroconidia.By Medmyco at English Wikipedia - Transferred from en.wikipedia to Commons., CC0, https://commons.wikimedia.org/w/index.php?curid=30361370
|
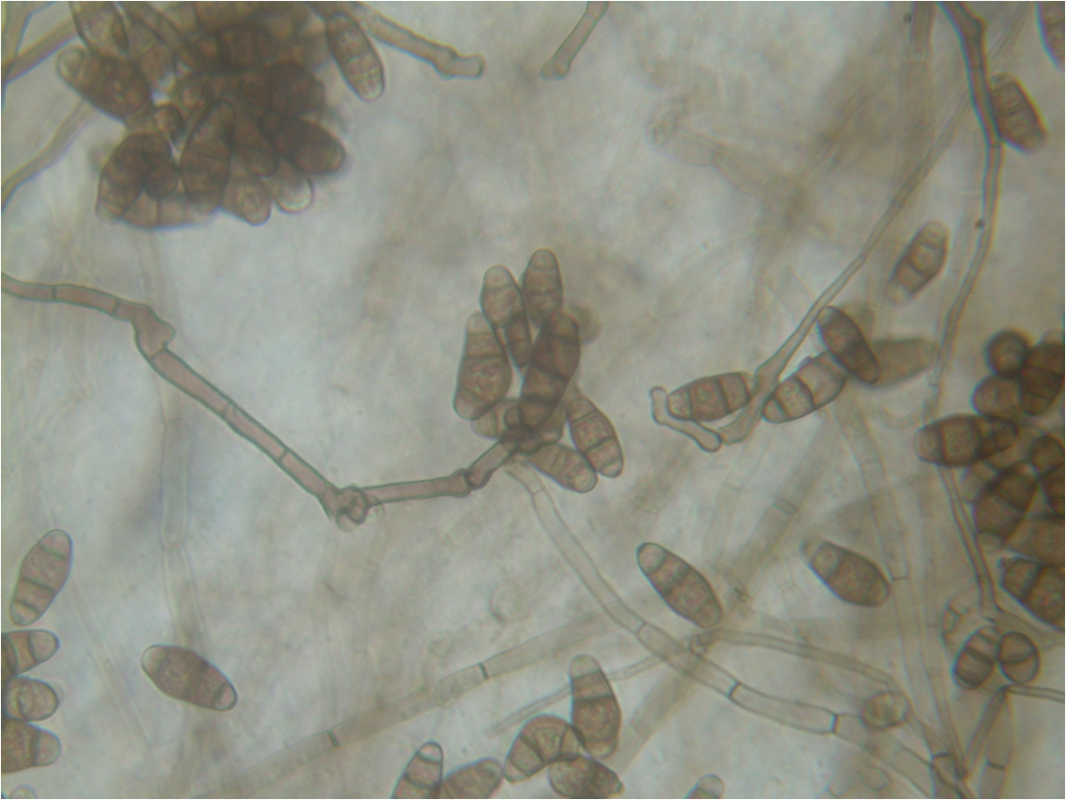
Poroconidia arise from "bent-knee-shaped" conidiophores.By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6764325
|
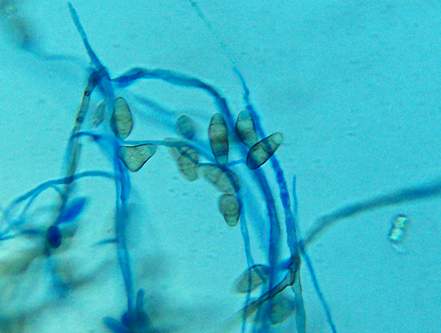
The ends of the poroconidia are lighter than the middle.By Microrao (Own work) [Public domain], via Wikimedia Commons
|
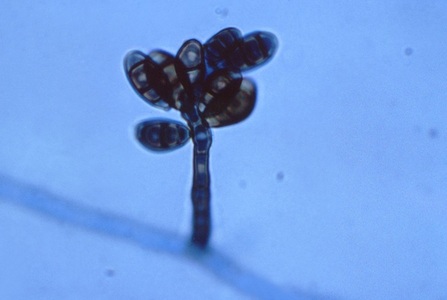
Poroconidia are centrally distended because of a central cell that is overly-enlarged.By Transferred from en.wikipedia to Commons.This media comes from the Centers for Disease Control and Prevention's Public Health Image Library (PHIL), with identification number #4512.Note: Not all PHIL images are public domain; be sure to check copyright status and credit authors and content providers.English | Slovenščina | +/−, Public Domain, https://commons.wikimedia.org/w/index.php?curid=1880104
|
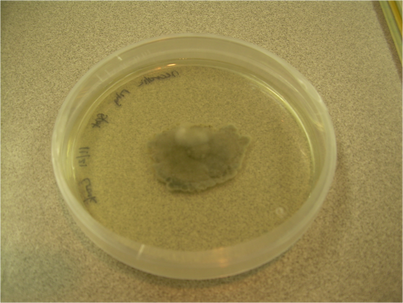
On SABHI at room temperature, Curvularia colonies grow moderately quickly as cottony, white, light pink, orange, or green as seen above with a brown reverse.By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
|

Curvularia oryzae;By Chanintorn Doungsa-ard, Department of Agriculture, Thailand - This image is found here at PaDIL, a source of images designed for Biosecurity and Biodiversity.This tag does not indicate the copyright status of the attached work. A normal copyright tag is still required. See Commons:Licensing for more information.PaDIL, CC BY 3.0 au, https://commons.wikimedia.org/w/index.php?curid=34765787
|

Curvularia verruciformis;By Chanintorn Doungsa-ard, Department of Agriculture, Thailand [CC BY 3.0 au (http://creativecommons.org/licenses/by/3.0/au/deed.en)], via Wikimedia Commons
|
Exserohilum spp:
This organism is the causative agent of phaeohyphomycosis or fungal sinusitis, keratitis, infected heart valve prosthesis, aortic embolus, corneal ulcer, CNS vasculitis, or meningitis; Infections require long-term treatment with amphotericin B.
Macroscopic Exam:
Microscopic Exam:
This organism is the causative agent of phaeohyphomycosis or fungal sinusitis, keratitis, infected heart valve prosthesis, aortic embolus, corneal ulcer, CNS vasculitis, or meningitis; Infections require long-term treatment with amphotericin B.
Macroscopic Exam:
- Colonies are rapid-growers on SABHI agar at room temperature.
- Colonies are light gray and woolly at first but darken with age.
- They produce a black reverse.
Microscopic Exam:
- Septate hyphae are dark.
- It produces long, dark, cylindrical poroconidia with 6-14 cells.
- Has distinct, protruding truncate hila in clusters.

Exserohilum stained with LPCB.See page for author [Public domain], via Wikimedia Commons
|
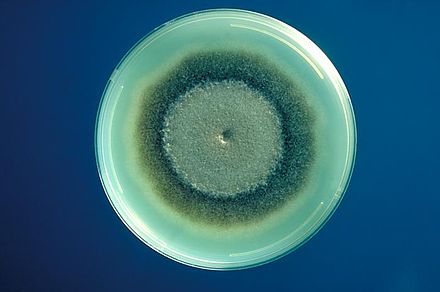
On SABHI agar at room temperature, colonies grow very quickly as umbonate, woolly, light gray colonies that become darker gray to black with age with a black reverse.By http://phil.cdc.gov/phil_images/20030513/15/PHIL_3786_lores.jpg, Public Domain, https://commons.wikimedia.org/w/index.php?curid=763317
|

The septate hyphae that characterize this fungi are dark with elongated, dark poroconidia, cylindrical in shape. There are 6-14+ cells that are distinct, protruding, and there are clusters of truncate hila.By CDC [Public domain], via Wikimedia Commons
|

Exserohilum macroconidia.By Wanich Khampanich, Department of Agriculture, Thailand - This image is found here at PaDIL, a source of images designed for Biosecurity and Biodiversity.This tag does not indicate the copyright status of the attached work. A normal copyright tag is still required. See Commons:Licensing for more information.PaDIL, CC BY 3.0 au, https://commons.wikimedia.org/w/index.php?curid=34767039
|
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
Epicoccum spp:
This organism is a causative agent of allergies.
Macroscopic Exam:
Microscopic Exam:
This organism is a causative agent of allergies.
Macroscopic Exam:
- It produces rings of yellow, orange, and brown, and pigments diffuse into the agar.
Microscopic Exam:
- Thick clusters of sporodchia (short conidiophores) support terminal dark round conidia
- Conidia have unconstricted horizontal AND vertical septa
- Conidia become rough-walled with age
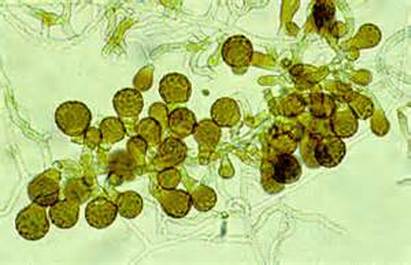
As seen in the image, Epicoccum spp are characterized by thick clusters of sporodchiaon short conidiophores, which support terminal DARK spherical conidia. The conidiophores contain both horizontal and vertical septa. As they age, the conidia develop into thick-walled/rough-walled structures.
|
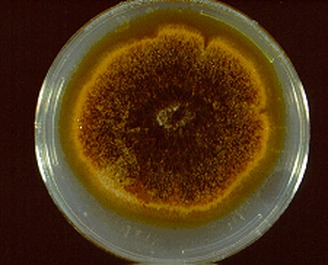
On SABHI at room temperature, this woolly colony produces rings of color, including yellow, orange, and tan-to-brown, whose color diffuses into the agar.
|
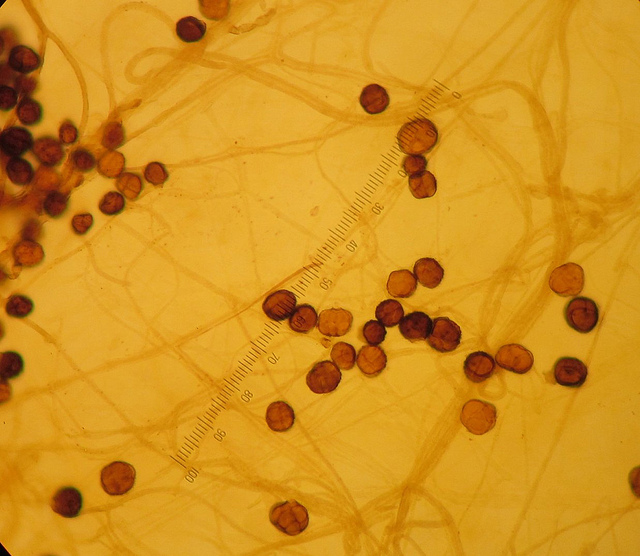
Onychocola canadensis:
This is a mold with arthrospores that is a rare cause of nail infections. It grows as a small, cream, white, or pale grey densely floccose to velvety, domed colony with a pale brown to grey reverse. Microscopically, you will see long chains of small oval arthrospores. It is a slow grower, arthrospores are slow to develop, and it resembles other species, such as Chryseosporium spp, Coccidioides spp, or Malbranchea spp.
This is a mold with arthrospores that is a rare cause of nail infections. It grows as a small, cream, white, or pale grey densely floccose to velvety, domed colony with a pale brown to grey reverse. Microscopically, you will see long chains of small oval arthrospores. It is a slow grower, arthrospores are slow to develop, and it resembles other species, such as Chryseosporium spp, Coccidioides spp, or Malbranchea spp.
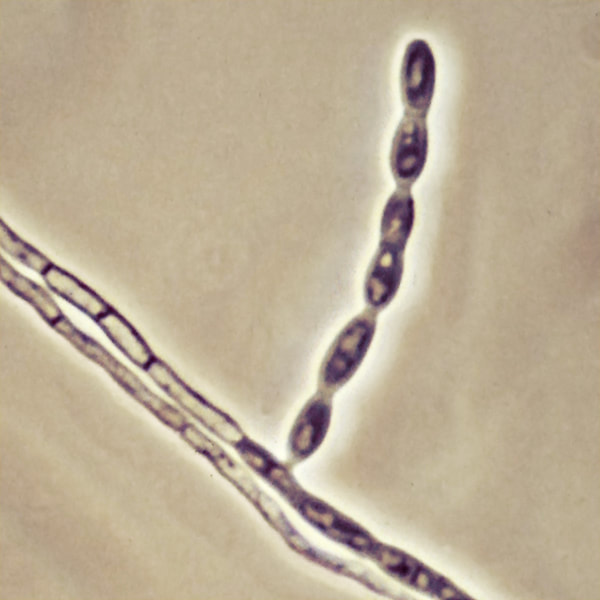
By Medmyco at English Wikipedia - Transferred from en.wikipedia to Commons., CC0, https://commons.wikimedia.org/w/index.php?curid=30360242
Ulocladium spp:
This species is commonly considered a contaminant and rarely causes infection. It is a plant pathogen and a decomposer that decomposes vegetation. In humans, it is occasionally linked to allergies or to more serious diseases in the immunocompromised. Some species are linked to keratitis, corneal infection in humans, onychomycosis (nail infection), or rarely, skin infections.
This species is commonly considered a contaminant and rarely causes infection. It is a plant pathogen and a decomposer that decomposes vegetation. In humans, it is occasionally linked to allergies or to more serious diseases in the immunocompromised. Some species are linked to keratitis, corneal infection in humans, onychomycosis (nail infection), or rarely, skin infections.
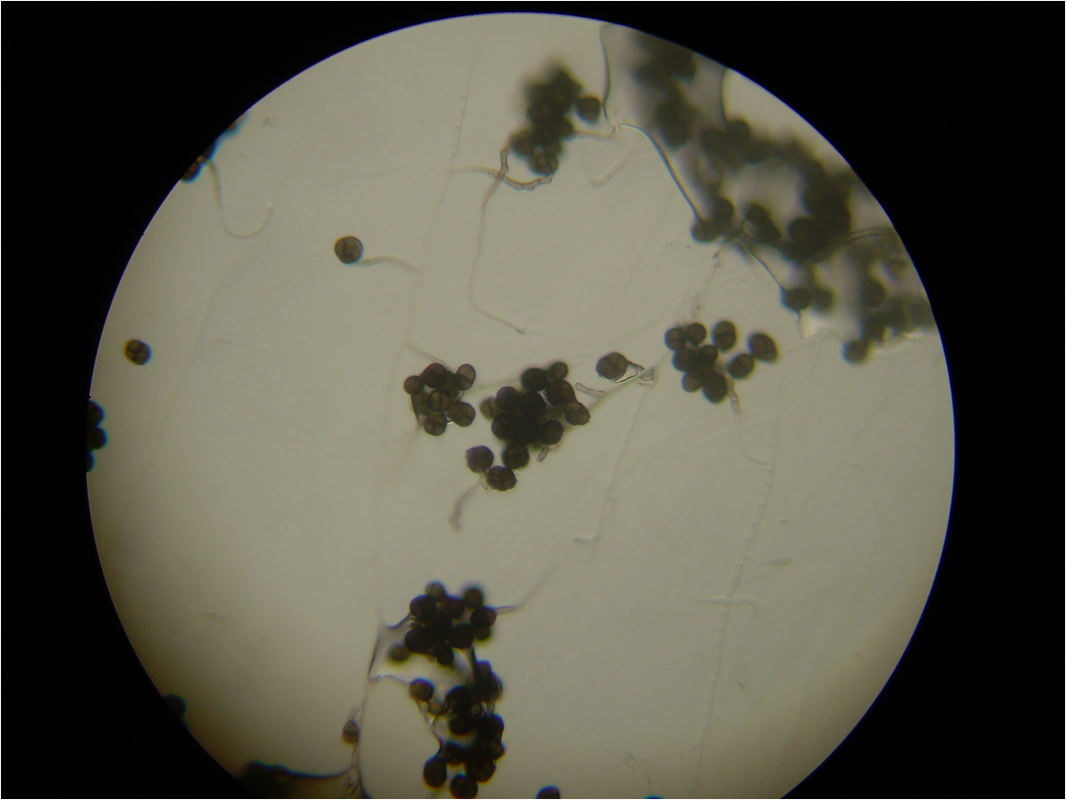
Conidia are dark brown-to-black in appearance, and they range from smooth-to-rough, and most are oval in shape.By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6754953
|
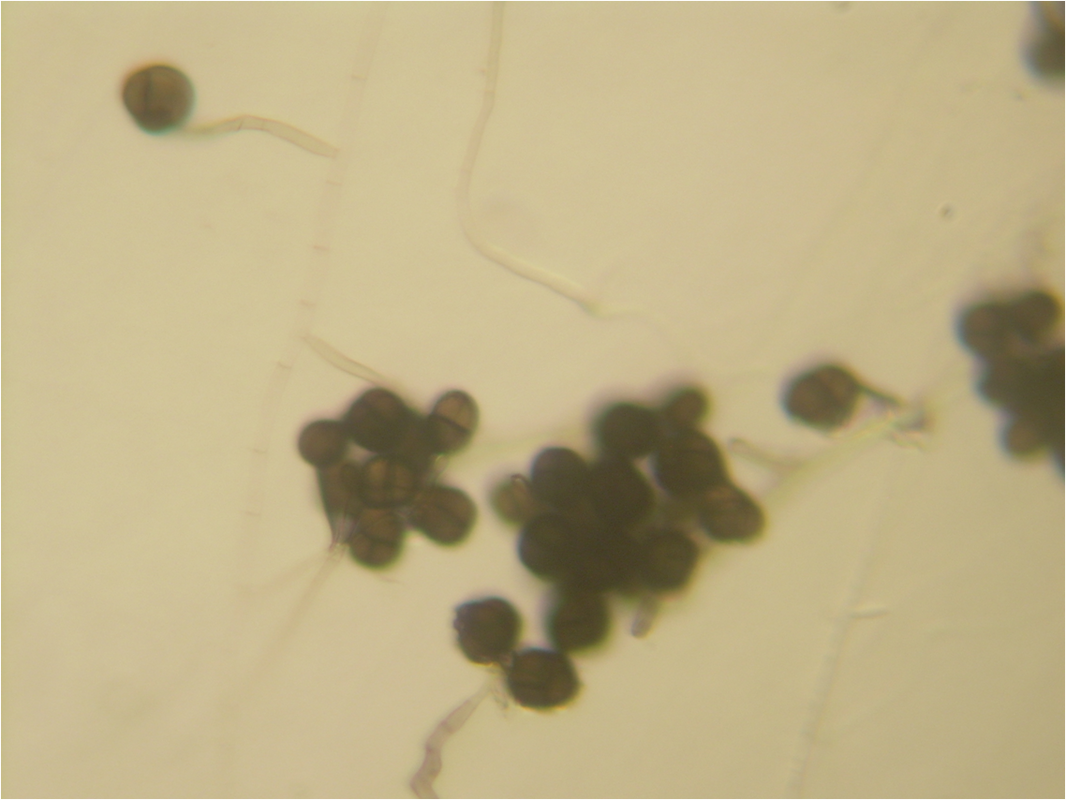
The conidiophores are both simple or branched and can be seen here, and some are bent where conidia are produced. This explains the "zigzag" appearanced of some of the conidia and conidiophores. Conidia contain both transverse and longitudinal septations, giving them a "hot cross buns" or "hot roll" appearance
|
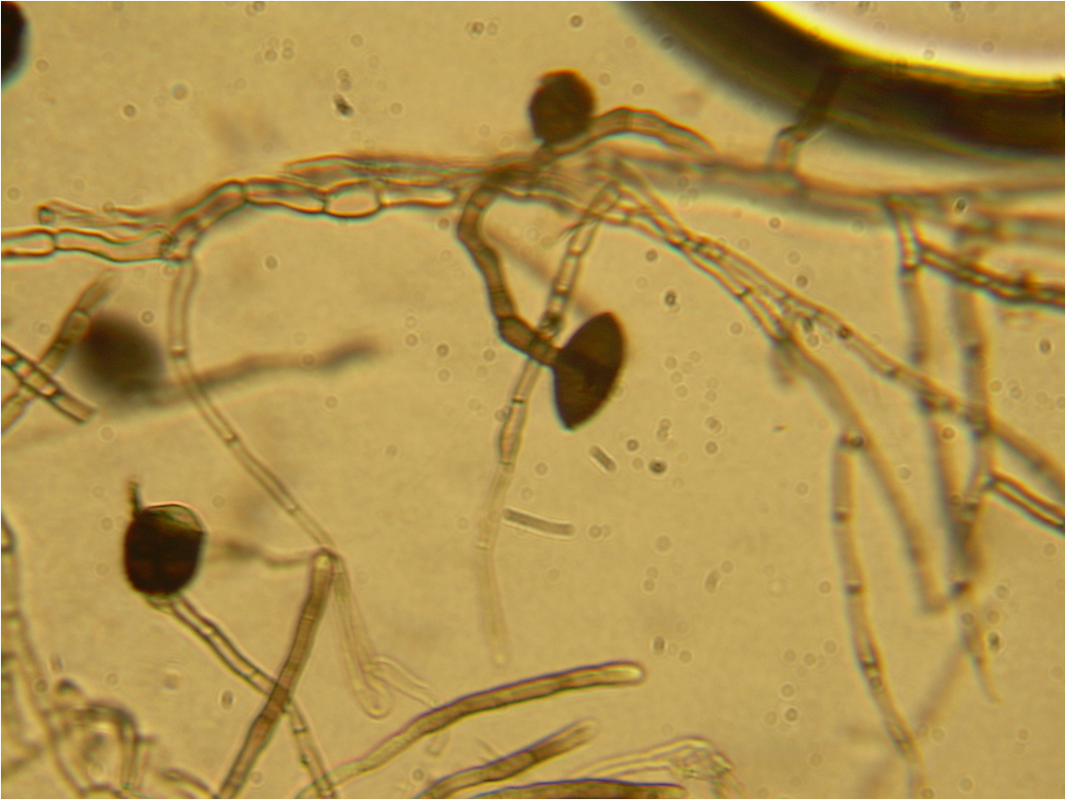
Sepatate hyphae may be observed in this slide, which are light brown and dark brown.
|
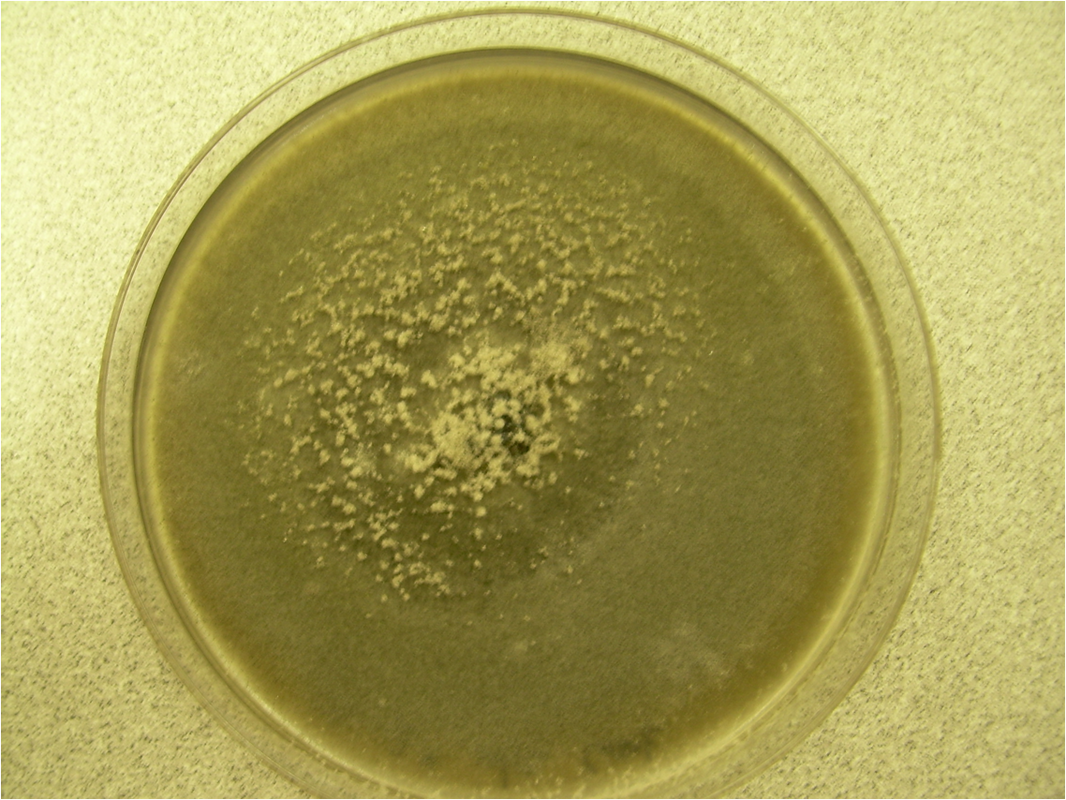
Ulocladium spp rapidly matures on SABHI in 5 days, with a dark brown-to-black, crumbly-to-cottony surface. The reverse is black.
|
Nigrospora spp:
Most of the time, considered a contaminant, but rarely a causative agent of keratomycosis, skin or nail infections, hay fever, or asthma.
Most of the time, considered a contaminant, but rarely a causative agent of keratomycosis, skin or nail infections, hay fever, or asthma.

On SABHI agar at room temperature, colonies grow and mature within 4 days as white and woolly, turning gray with age, with a black reverse. Colonies quickly fill the plate and with age, the aerial mycelium become gray.
|

The hyphae of this organism are dark with short, fat, and septate with conidiophores supporting round-to-oval, single, smooth-walled, large, black conidia at the terminal end ranging from 10-14 microns in diameter.
|
Fonsecaea pedrosoi:
This is the one of thhe most common causative agents of chromoblastomycosis worldwide. Typically, lesions occur on the lower extremities and rarely cause internal infections. This slow grower takes about 14 days to mature. Colonies are black, gray or dark green with silvery, velvety mycelium and are flat-to-convex with a black reverse.
This is the one of thhe most common causative agents of chromoblastomycosis worldwide. Typically, lesions occur on the lower extremities and rarely cause internal infections. This slow grower takes about 14 days to mature. Colonies are black, gray or dark green with silvery, velvety mycelium and are flat-to-convex with a black reverse.
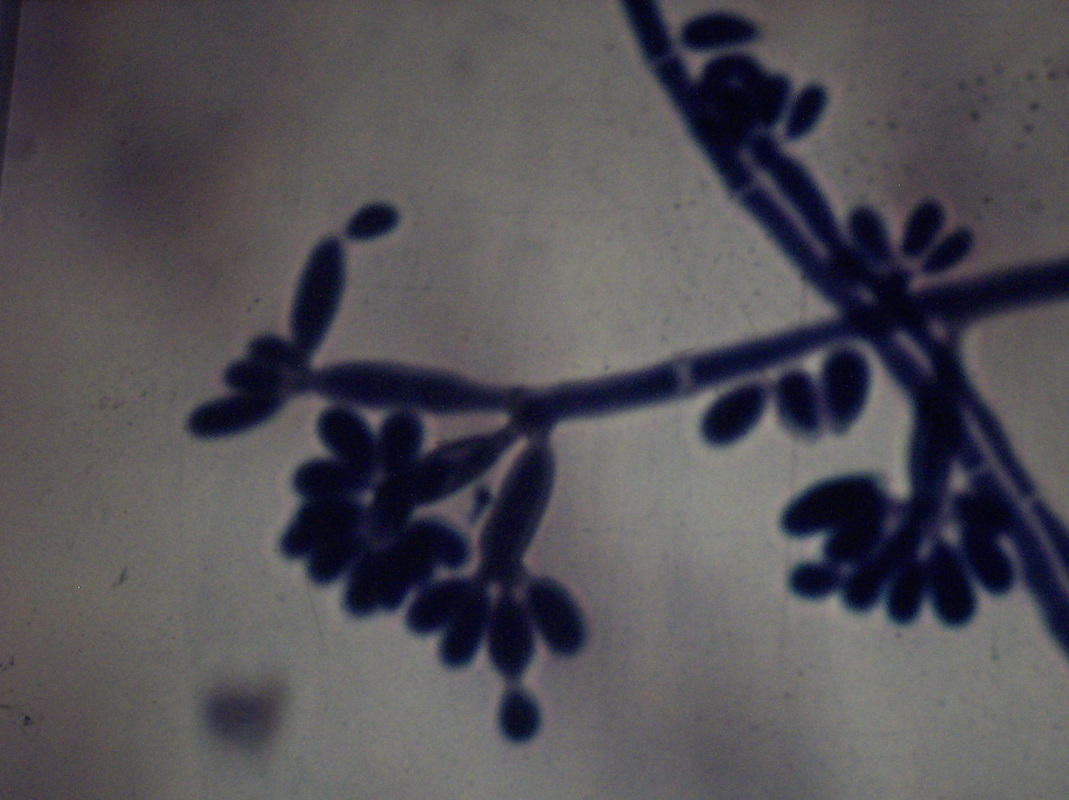
Fonsecaea pedrosoi;By Roberto J. Galindo - Own Work: Foto tomada por Roberto J. Galindo, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=2320167
|
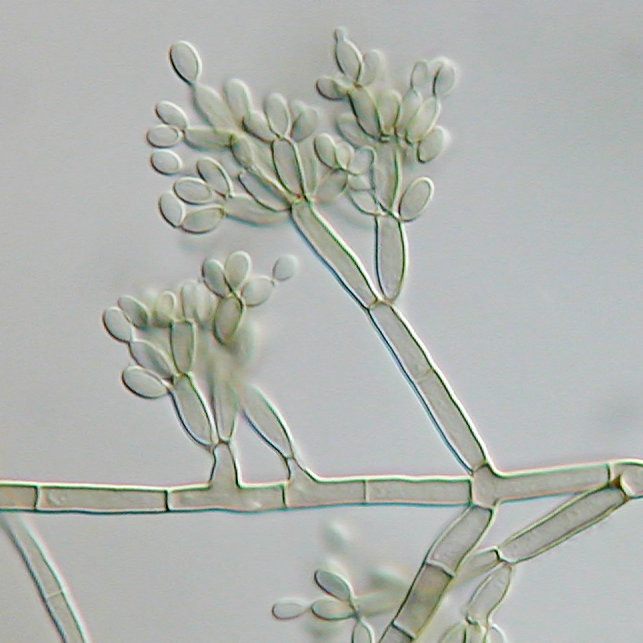
By Medmyco at English Wikipedia - Transferred from en.wikipedia to Commons., CC0, https://commons.wikimedia.org/w/index.php?curid=30364123
|
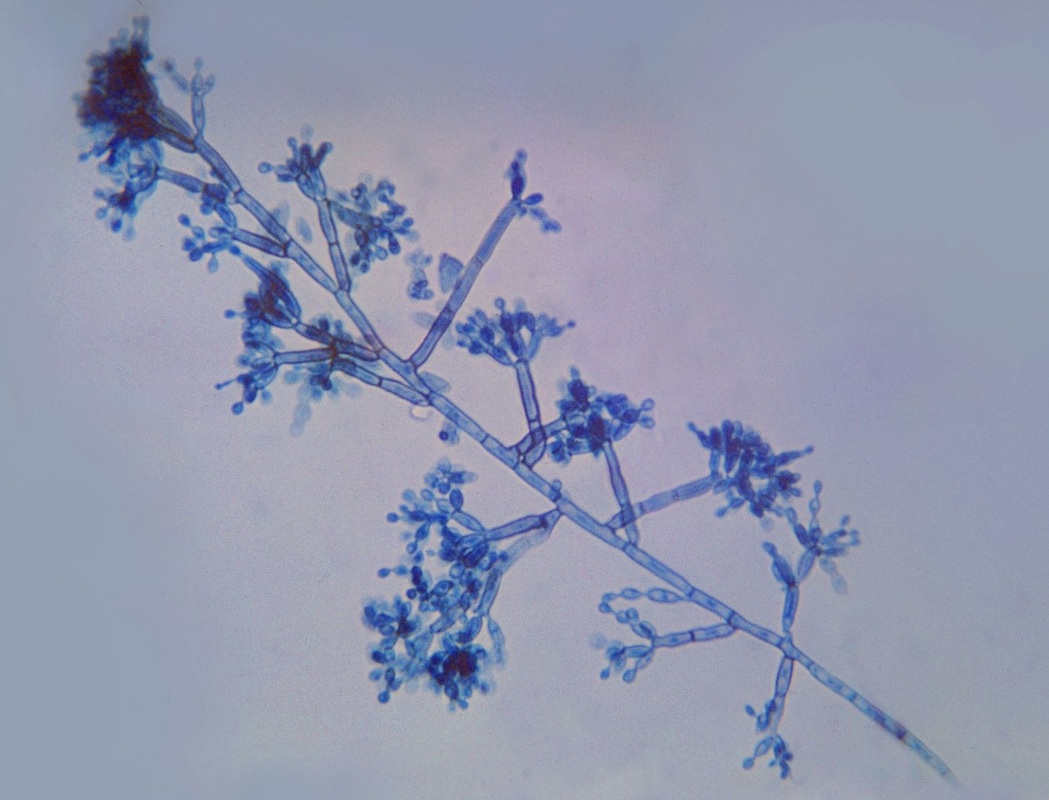
By CDC/Sherry Brinkman - This media comes from the Centers for Disease Control and Prevention's Public Health Image Library (PHIL), with identification number #2920.Note: Not all PHIL images are public domain; be sure to check copyright status and credit authors and content providers.English | Slovenščina | +/−, Public Domain, https://commons.wikimedia.org/w/index.php?curid=763232
|
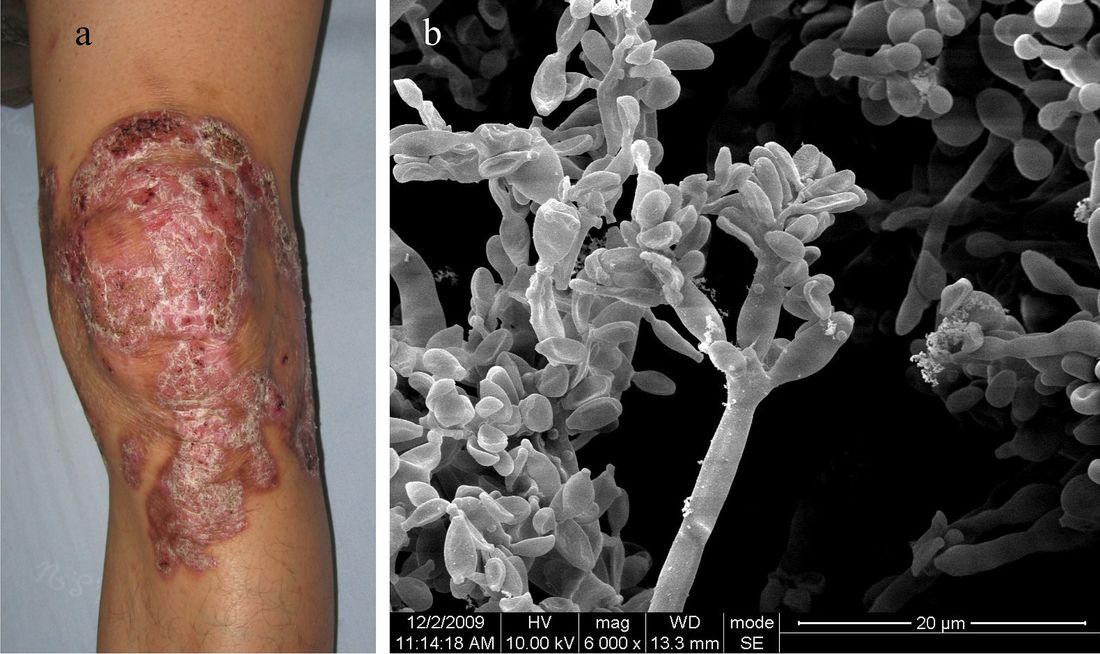
By Ran Yuping et al. ([1]) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
|
Phialophora verrucosa, P. richardsiae:
Phialophora species are decomposers of fruit, but they can also parasitize humans (skin). Microscopically, they produce short conidiophores shaped like "vases", bearing oval-shaped conidia in clusters.
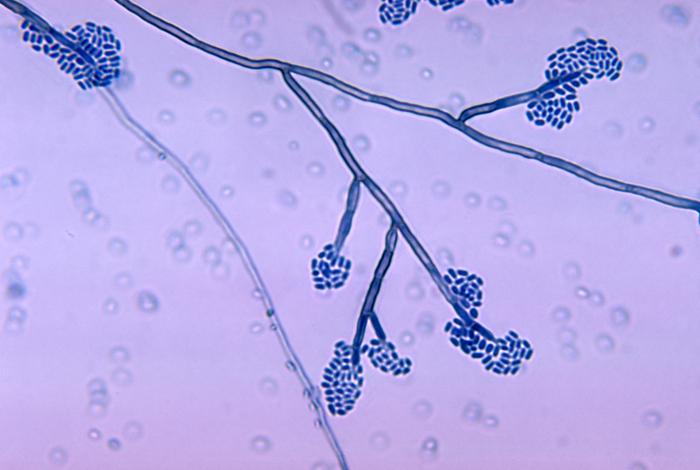
|

|
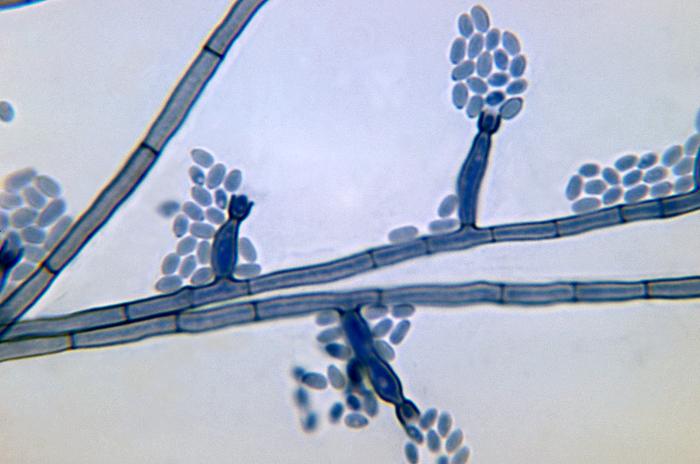
pithomyces spp:
By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
|
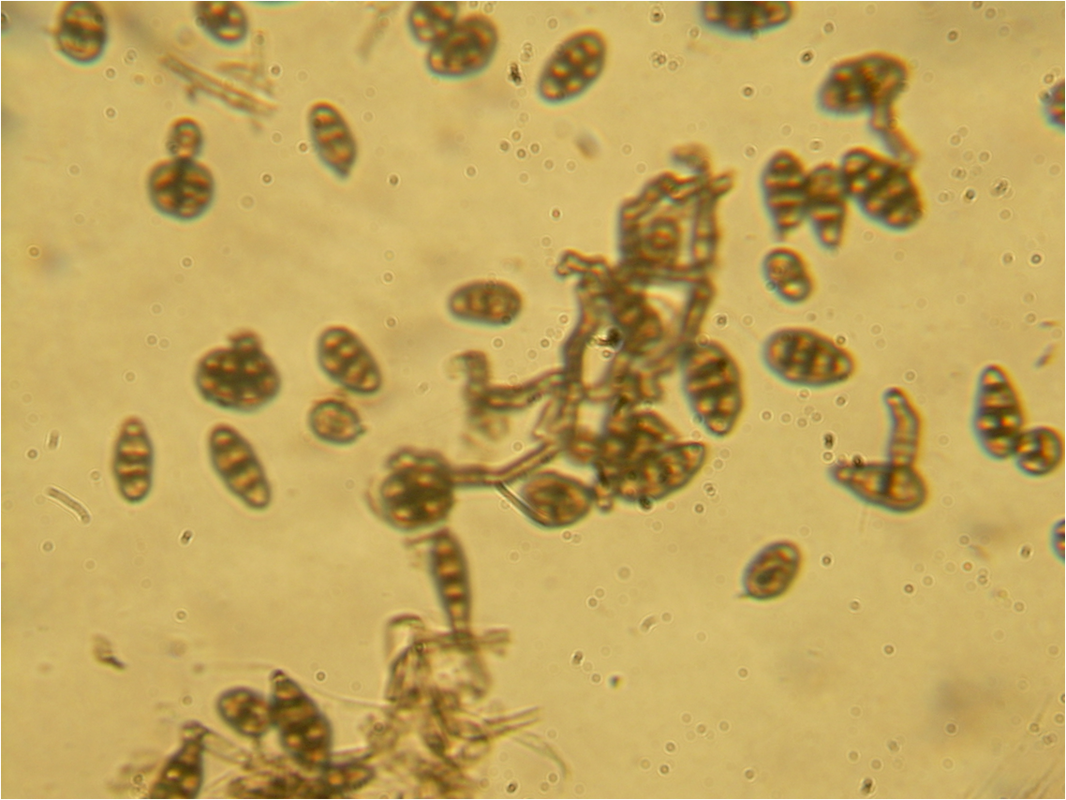
By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6694465
|
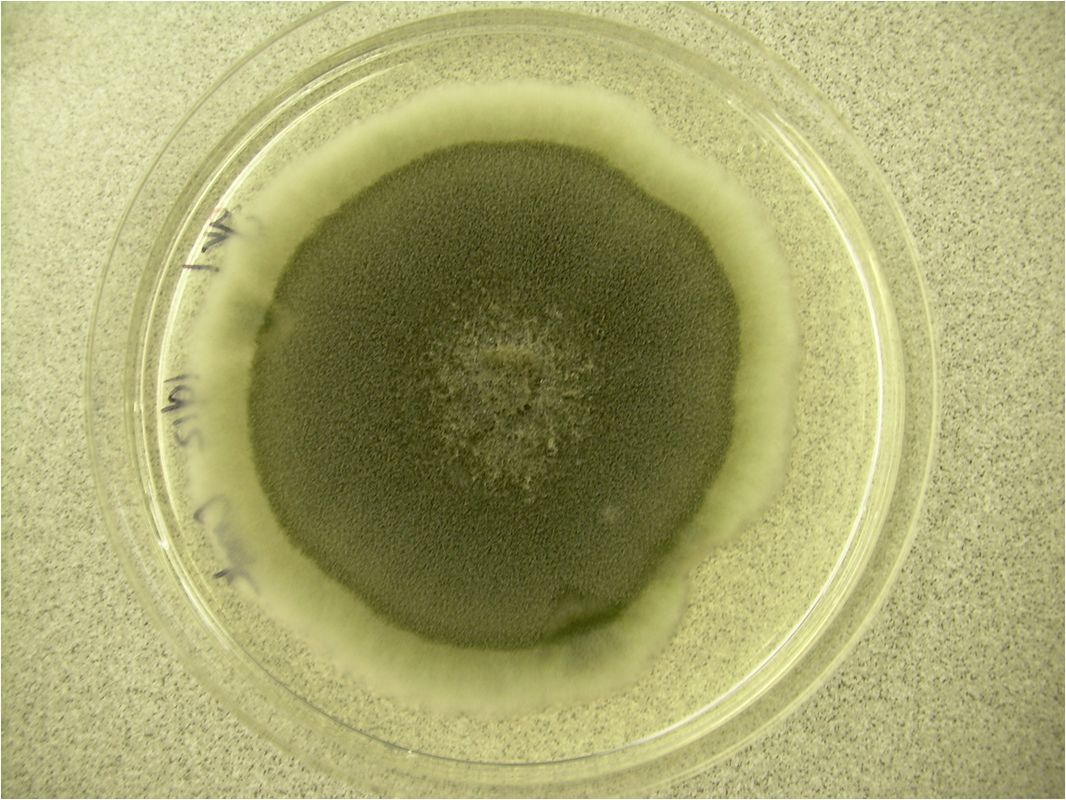
By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6694433
Chaetomium spp:
This spp is commonly considered a contaminant. It rarely causes cutaneous phaeohyphomycosis or systemic disease. It is found in the soil, air, plant debris, and cellulose. It can cause allergic hypersensitivity reactions in some individuals. There have been several cases of deep, fatal infections in humans (rare). It has also rarely been linked to brain abscess, peritonitis, and onychomycosis. It has been linked to CNS infections, lung, skin and eye infections.
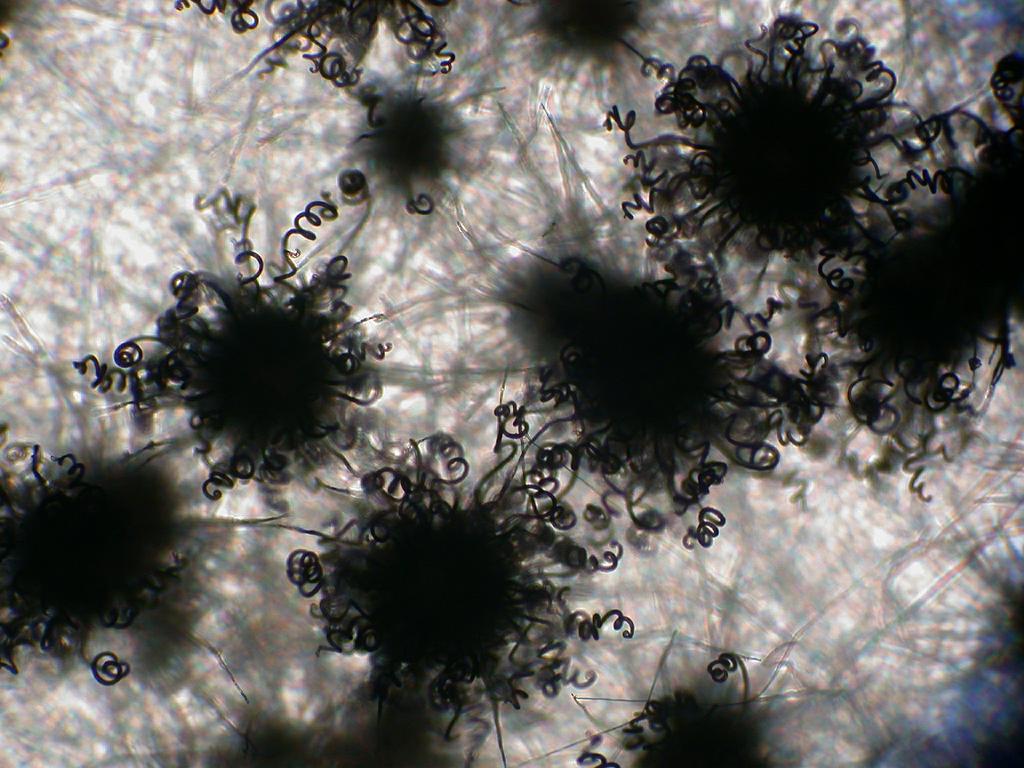
By No machine-readable author provided. Keisotyo assumed (based on copyright claims). - No machine-readable source provided. Own work assumed (based on copyright claims)., CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=1762242
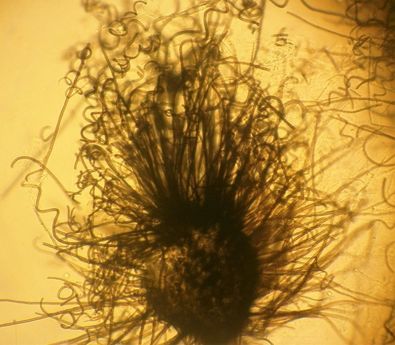
By Ulitca (Own work) [CC BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0)], via Wikimedia Commons
|
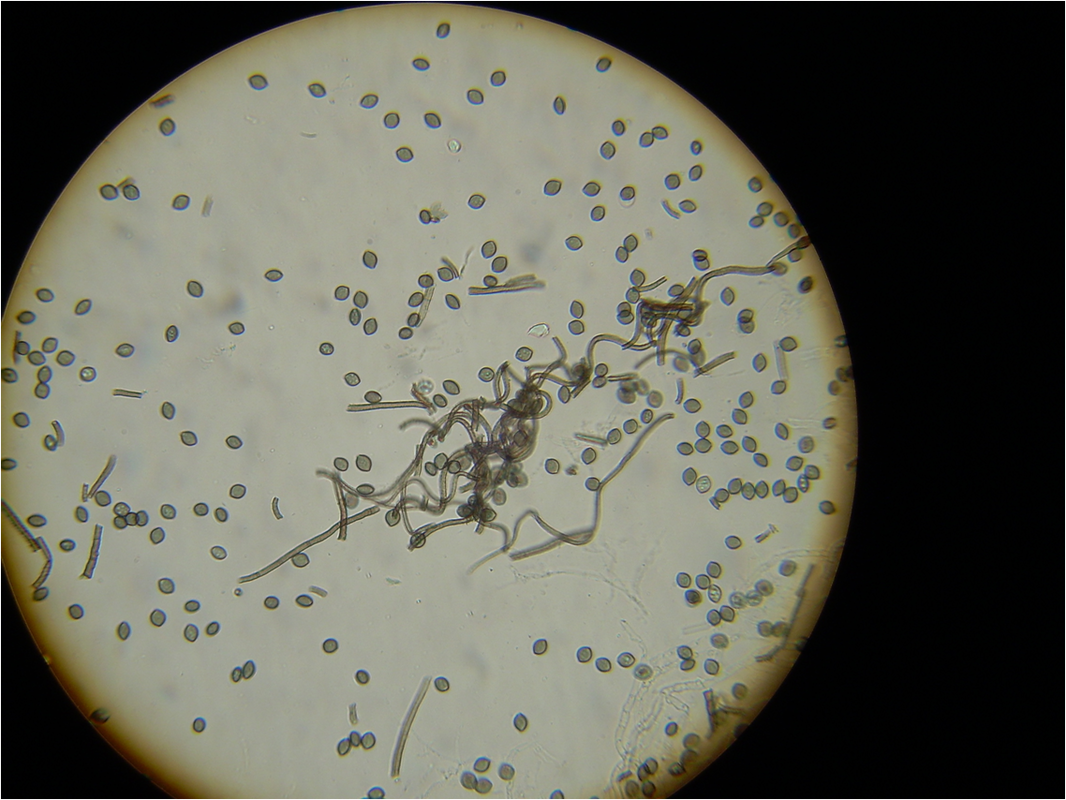
By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6762231
|
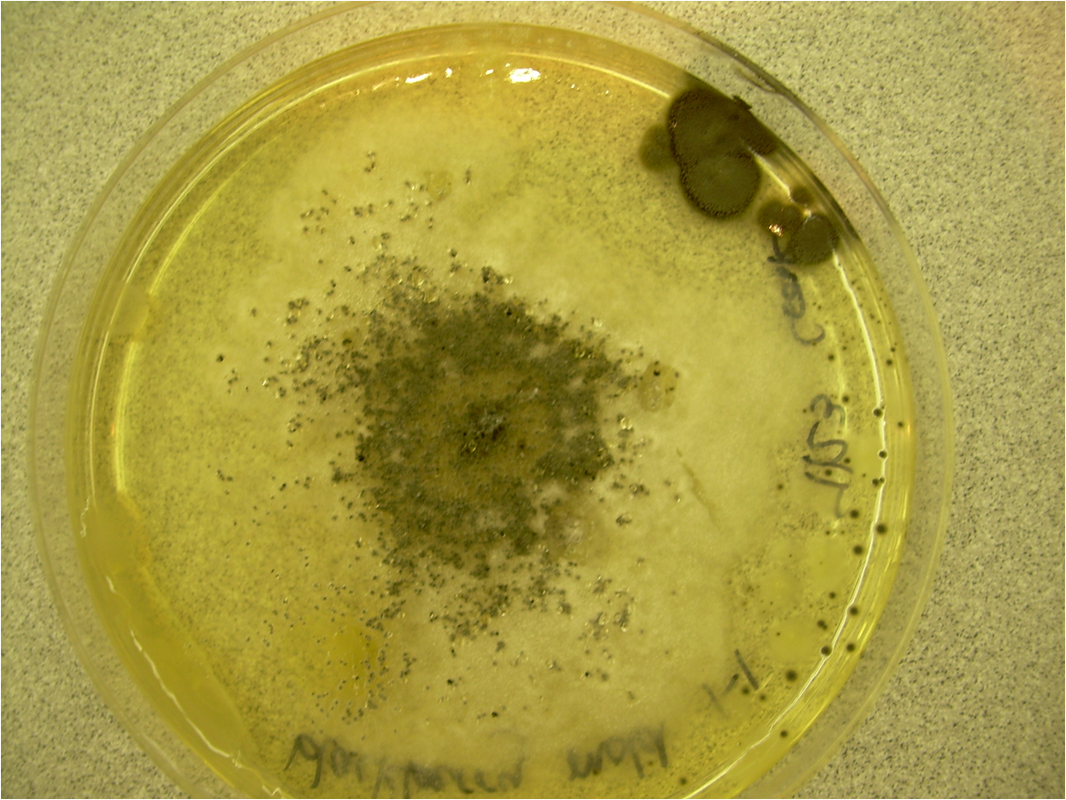
By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
phoma spp:
This spp is commonly considered a contaminant. It rarely causes phaeohyphomycosis.

By Brawlings - Olympus BX45 Stereo Microscope 600x magnification, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=25136065
Others:
Myrmercridium schulzeri
Rhinocladiella mackenziei
Pleurostoma richardsiae
Phaeoacremonium parasiticum
Phialemonium spp
Scedosporium apiospermum complex
Myrmercridium schulzeri
Rhinocladiella mackenziei
Pleurostoma richardsiae
Phaeoacremonium parasiticum
Phialemonium spp
Scedosporium apiospermum complex
II. HYALINE OPPORTUNISTS:
Hyaline opportunitsts tend to produce light-colored colonies with light-colored hyphae may cause hyalohyphomycosis. Because they tend to be transparent and light, the lactophenol cotton blue stain for microscopic morphology is extremely beneficial.
Acremonium spp:
This organism is the causative agent of keratomycosis, mycetoma, lesions of the hard palate, meningitis, arthritis, or systemic disease.
Macroscopic Exam:
Microscopic Exam:
Hyaline opportunitsts tend to produce light-colored colonies with light-colored hyphae may cause hyalohyphomycosis. Because they tend to be transparent and light, the lactophenol cotton blue stain for microscopic morphology is extremely beneficial.
Acremonium spp:
This organism is the causative agent of keratomycosis, mycetoma, lesions of the hard palate, meningitis, arthritis, or systemic disease.
Macroscopic Exam:
- On SABHI at room temperature, this is a rapid-grower.
- It produces wrinkled, membranouse, white, gray, or rose-colored colonies that become covered with loose, aerial mycelium, making it appear velvety.
- The reverse is either colorless, pale, yellow or pinkish.
Microscopic Exam:
- The mycelium is septate and has cross-walls.
- The tapering conidiophores are unbranched and support closely packed spheres of sickle-shaped or elliptical-shaped conidia.
- Sometimes the conidiophores are in whorls around the hyphae.
- It is not dimorphic, though it slightly resembles Sporothrix schenckii.
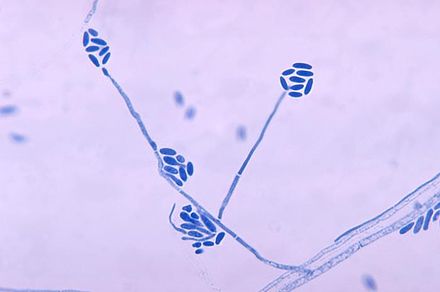
This LPCB stained specimen shows the septate hyphae that characterize the Acremonium spp, along with unbranched, tapering conidiophores that support balls of sickle-shaped or elliptical-shaped conidia that are tightly packed together.By http://phil.cdc.gov/phil_images/20030717/10/PHIL_4168_lores.jpg, Public Domain, https://commons.wikimedia.org/w/index.php?curid=763362
|

At room temperature, on SABHI agar, this fungi is a rapid-grower with a wrinkled, membranous, white, gray or rose colony that, with maturity, becomes covered with loose aerial mycelium. The reverse may be pale, colorless, light yellow or pink.See page for author [Public domain], via Wikimedia Commons
|
Coccidioides immitis:
Coccidioides immitis is unique in that it produces "barrel-shaped" arthroconidia. It causes the disease coccidioidomycosis, or "valley fever". This organism is mainly seen out west in the states of Arizona, New Mexico, Nevada, West Texas, Utah, California and in Mexico. It thrives in the dry desert climate. It is very difficult to diagnose and it forms a mass in the lungs that can resemble lung cancer or a tumor on chest X-rays. Accurate diagnosis sometimes requires an actual biopsy.
The incubation period is 7-21 days and symptoms include an ongoing fever that lasts >1 month, weight loss, night sweats, lung infiltrates, weakness, and possible meningeal involvement.
The incubation period is 7-21 days and symptoms include an ongoing fever that lasts >1 month, weight loss, night sweats, lung infiltrates, weakness, and possible meningeal involvement.
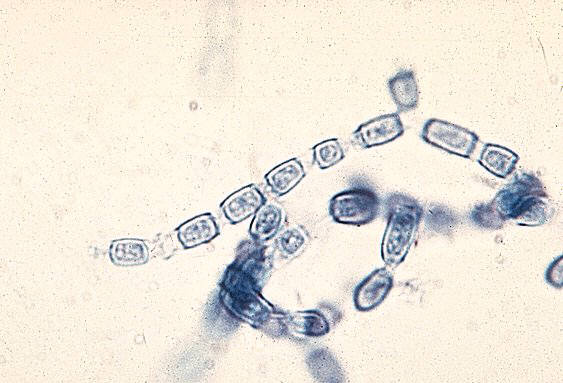
By http://phil.cdc.gov/PHIL_Images/11121998/00004/39G0040_lores.jpg, Public Domain, https://commons.wikimedia.org/w/index.php?curid=759647

1965, CDC, Dr. Lucille George,https://phil.cdc.gov/Details.aspx?pid=12196
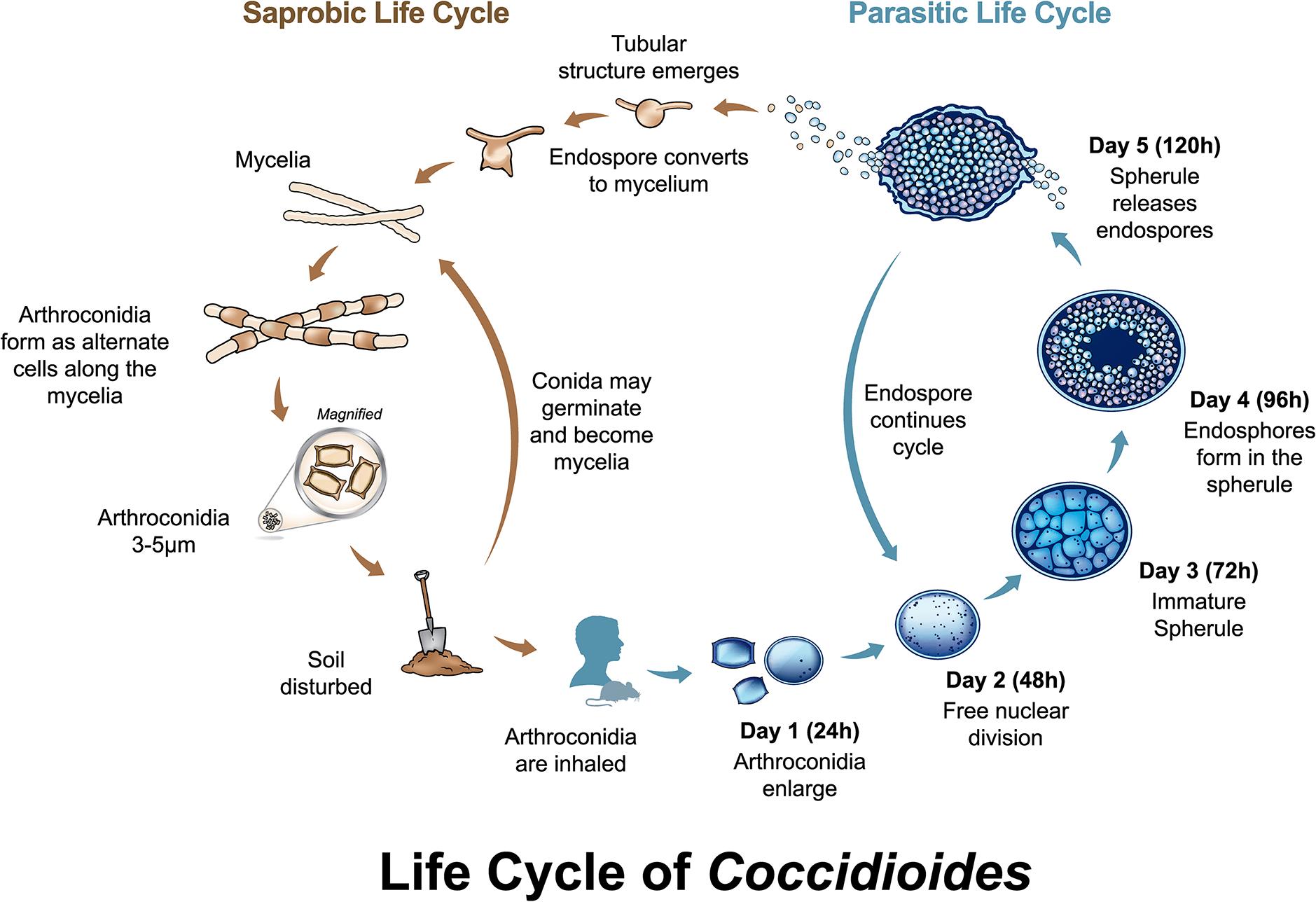
https://upload.wikimedia.org/wikipedia/commons/1/19/Life_cycle_of_Coccidioides.PNG
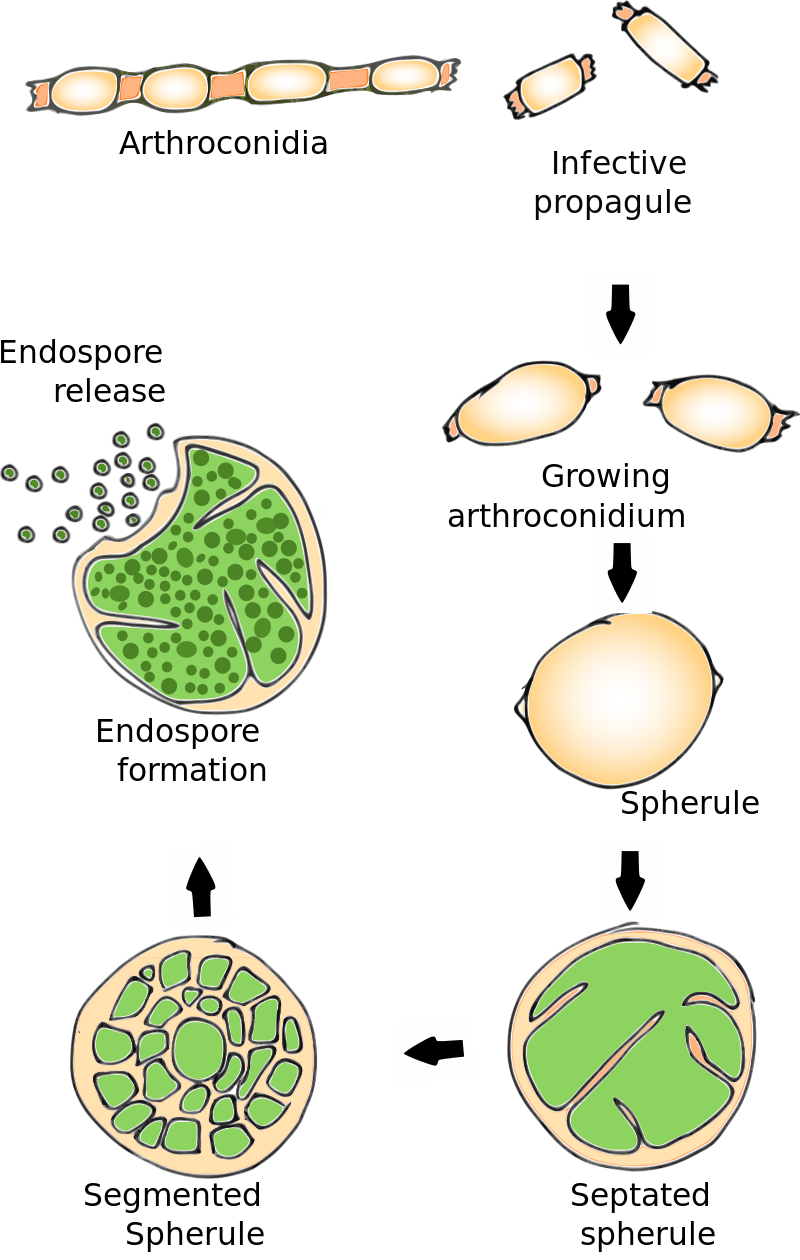
https://upload.wikimedia.org/wikipedia/commons/thumb/6/62/Life_cycle_of_coccidioides.svg/800px-Life_cycle_of_coccidioides.svg.png
|
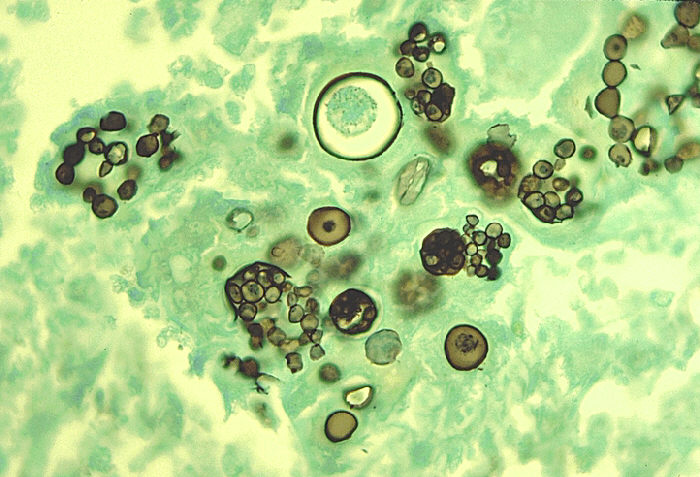
https://upload.wikimedia.org/wikipedia/commons/7/7b/Spherule_and_endospore_forms_of_Coccidioides_immitis_01ee057_lores.jpg
|

https://upload.wikimedia.org/wikipedia/commons/f/f2/Coccidioides_immitis.jpg
Trichoderma Spp:
This species of mold is a soil inhabitant. There are about 89 species, one of which is considered to be a toxic household mold. Trichoderma longibrachiatum is toxic because it produces toxins that can affect the central nervous system, including neurons (nerve cells), myocytes (heart cells) and pneumocystis (lung cells).
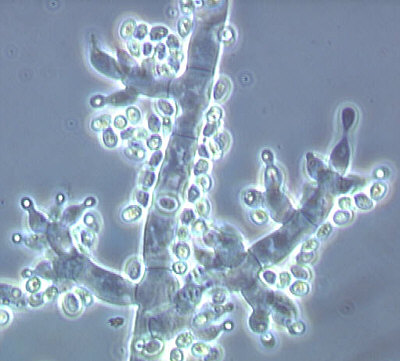
See page for author [Public domain], via Wikimedia Commons
|
By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6770154
|

https://upload.wikimedia.org/wikipedia/commons/0/07/Trichoderma_colony_in_nature.jpg
Aspergillosis:
The human pathogens Aspergillus flavus, fumigatus, niger and others may cause a variety of human illness. They aer commonly found in the air, so exposure is widespread. Construction, contaminated ventilation systems, and compost heaps are also sources of exposure. Aspergillosis is a common occurrence in patients with underlying chronic pulmonary disease like chronic sinusitis or emphysema. There are several forms:
The human pathogens Aspergillus flavus, fumigatus, niger and others may cause a variety of human illness. They aer commonly found in the air, so exposure is widespread. Construction, contaminated ventilation systems, and compost heaps are also sources of exposure. Aspergillosis is a common occurrence in patients with underlying chronic pulmonary disease like chronic sinusitis or emphysema. There are several forms:
- Aspergilloma (fungus ball)
- PulmonaryParanasal Sinus
- Develops after unrestricted growth of the mold within a pulmonary cavity
- A. fumigatus (MAIN CAUSE); produces endotoxins
- A niger (can cause, but not the main type; rare)
- Dyspnea, hemoptysis
- May have underlying tuberculosis, sarcoidosis, or other
- Fungus ball (mass of tangled hyphae/mycelium)
- Hyphae seen in sputum on Gram stain
- Serology test helps in detection
- Surgical removal necessary if bleeding occurs
- Develops after unrestricted growth of the mold within a paranasal sinus
- Allergic Disease
- Asthma
- Hay Fever
- Allergic Alveolitis with Secondary Fibrosis
- Allergic Bronchopulmonary Aspergillosis (dyspnea, shortness of breath, aspergillum growing in airways, inflammation, bronchial mucous plugs and bronchial dilation)
- Exacerbates cystic fibrosis
- Sputum may contain bronchial casts
- Allergic Aspergillus Sinusitis (obstruction and mucoid exudate with hyphae and eosinophils)
- Caused by inhaling spores, which cause an allergic or asthmatic reaction
- Invasive Aspergillosis (Life-Threatening)
- Acute Invasive Disease (Pulmonary, Paranasal Sinus, Disseminated)
- Invasion of tissues by aspergilli (A. fumigatus)
- Seen in severely ill patients, especially if they have neutropenia, organ transplant recipients, multiorgan failure, or who are receiving high doses of corticosteroids
- Fever, cough, pulmonary infiltrates, pleural effusions, cavitations, intrabronchial invasion by aspergilli
- Chronic Necrotizing Disease (Rare)
- Inflammation with fibrosis in those with underlying illness such as sarcoidosis, chronic corticosteroid therapy, or fibrotic lung disease leading to extensive fibrosis and recurrent secondary infections with weight loss and fever, chronic infiltrate, bronchial dilation, and aspergillomas
- Paranasal Aspergillus Granuloma
- Occurs in severely immunocompromised patients
- Facial pain and swelling with nasal obstruction, palatal erosion, and even spread to sites like the brain or bone
- Progressive and invasive
Aspergillus spp:
The most common opportunistic pathogen of the genus is Aspergillus fumigatus. It can cause disseminated aspergillosis, pulmonary disease, allergic bronchopulmonary disease (farmer's lung), keratomycosis (eye infections), otomycosis (ear infections), or infection of the nasal sinuses.
Aspergillus fumigatus:
A. fumigatus is the predominant cause of aspergillosis in both humans and animals, and it is ubiquitous (found everywhere and is a common environmental organism). In immunocompromised patients, inhaling the spores can cause invasive, life-threatening infections of the lungs, sinuses, or other parts of the body, and can spread throughout the body resulting in a systemic infection, which can be fatal. In those who are not sick, it can cause a local infection of the sinuses, lungs, or other sites, such as the nails. It can also provoke allergies and asthma in susceptible individuals.
It is the most common opportunistic pathogen of the genus. It is linked to disseminated aspergillosis, pulmonary disease, and allergies. It can also cause bronchopulmonary disease and bronchospasm (farmer's lung).
Macroscopic Exam:
Microscopic Exam:
The most common opportunistic pathogen of the genus is Aspergillus fumigatus. It can cause disseminated aspergillosis, pulmonary disease, allergic bronchopulmonary disease (farmer's lung), keratomycosis (eye infections), otomycosis (ear infections), or infection of the nasal sinuses.
- A. fumigatus-most common cause of aspergillosis
- A. flavus-typically a contaminant, but has also been known to cause illness; commonly linked to production of aflatoxins, which are mycotoxins that are known carcinogens and have been known to contaminate peanuts, grains, cereals, breads
- A. niger-typically a contaminant, but has also been known to cause disease in the immunocompromised and is a common cause of otomycosis (ear infection)
- A. nidulans-typically a contaminant, but has been known to cause infections
- A. terreus-typically a contaminant, but has been known to cause infections
- A. versicolor-typically a contaminant, but has been known to cause infections
- A. clavatus-typically a contaminant
- A. glaucus group-typically a contaminant, but has been known to cause infections under various conditions
- A. ustus -a rare cause of human disease
- A. candidus-a rare cause of onychomycosis and otomycosis
Aspergillus fumigatus:
A. fumigatus is the predominant cause of aspergillosis in both humans and animals, and it is ubiquitous (found everywhere and is a common environmental organism). In immunocompromised patients, inhaling the spores can cause invasive, life-threatening infections of the lungs, sinuses, or other parts of the body, and can spread throughout the body resulting in a systemic infection, which can be fatal. In those who are not sick, it can cause a local infection of the sinuses, lungs, or other sites, such as the nails. It can also provoke allergies and asthma in susceptible individuals.
It is the most common opportunistic pathogen of the genus. It is linked to disseminated aspergillosis, pulmonary disease, and allergies. It can also cause bronchopulmonary disease and bronchospasm (farmer's lung).
Macroscopic Exam:
- On agar, it grows rapidly at 30-37 degrees Celsius as a flat, spreading, powdery to felt-like colony that is smoky, blue-green in color, and may be surrounded by a white margin ("apron").
- Aspergillus fumigatus grows at 45 degrees Celsius, whereas other species do not.
- It has a cream reverse.
Microscopic Exam:
- The mycelium is septate.
- The conidiophores are unbranched and either smooth or rough, with a foot cell at the base.
- The conidiophores bear a large vesicle at their tip.
- The vesicles support short, flask-shaped phialides in a single or double row, which produce chains of smooth or rough phialoconidia.
- Sporing heads seen under the microscope bear large, wide, pear-to-flask-shaped vesicles with one row of crowded phialides pointing upward over the upper 2/3rds of the surface.
- Conidia are produced in parallel chains.
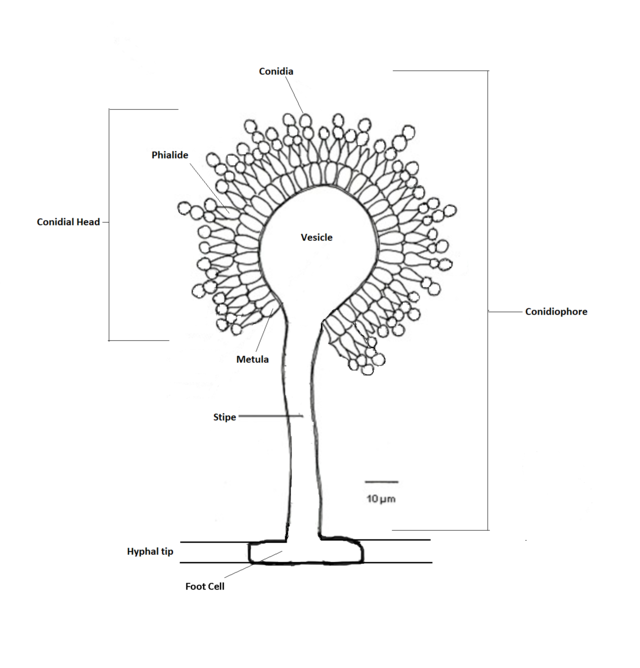
https://upload.wikimedia.org/wikipedia/commons/thumb/a/af/Aspergillus_wentii_morphological_structure.png/640px-Aspergillus_wentii_morphological_structure.png
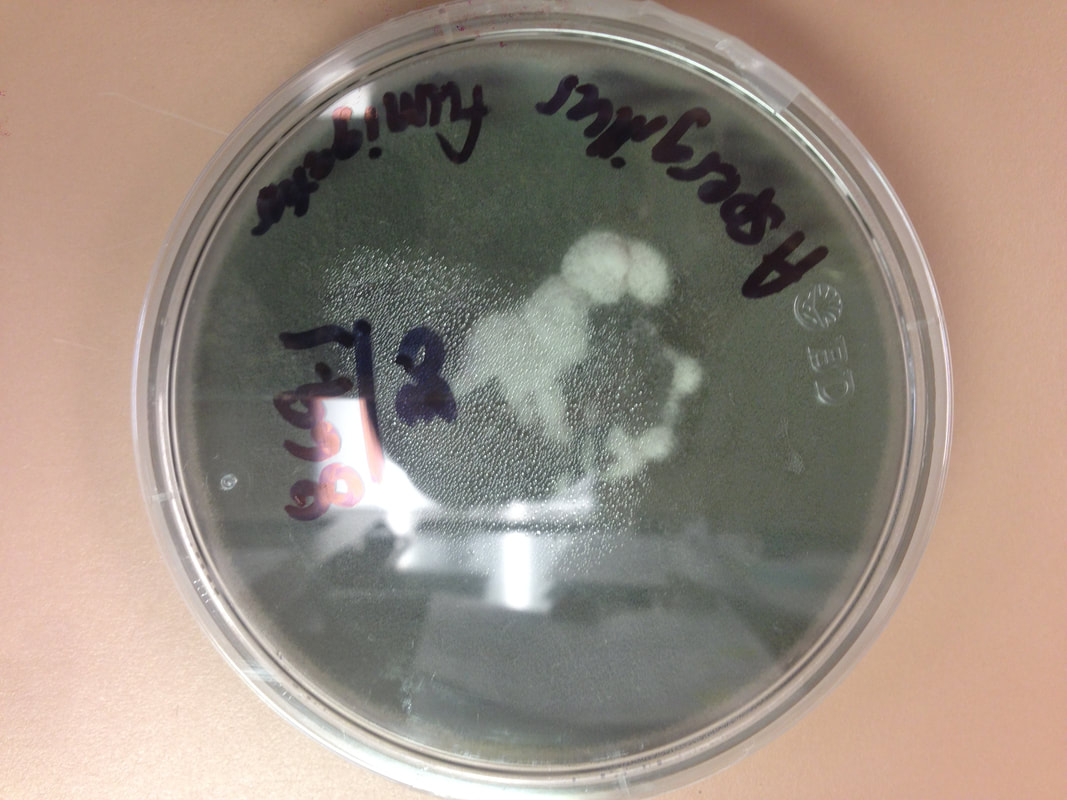
A. fumigatus, image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|
A. fumigatus, image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|

The mycelium are septate, unbranched, smooth or rough conidiophores with a unique FOOT CELL at their base, which support a big vesicle at their tip. The vesicle in turn supports short, vase-shaped phialides on a single or double row. These produce chains of smooth or rough phialoconidia.https://phil.cdc.gov/Details.aspx?pid=300
|

At room temperature on SABHI agar, these rapidly growing colonies exhibit rugose and velvety or powdery characteristics with dense production of conidia, and colors ranging from blue, green, yellow, black, white and gray. The reverse is white to tan in color. Interestingly, this species can really grow at any temperature.By Dr. David Midgley - Dr. David Midgley. Dr. Midgley cultured the isolate himself and also captured the photo., CC BY-SA 2.5, https://commons.wikimedia.org/w/index.php?curid=1023087
|
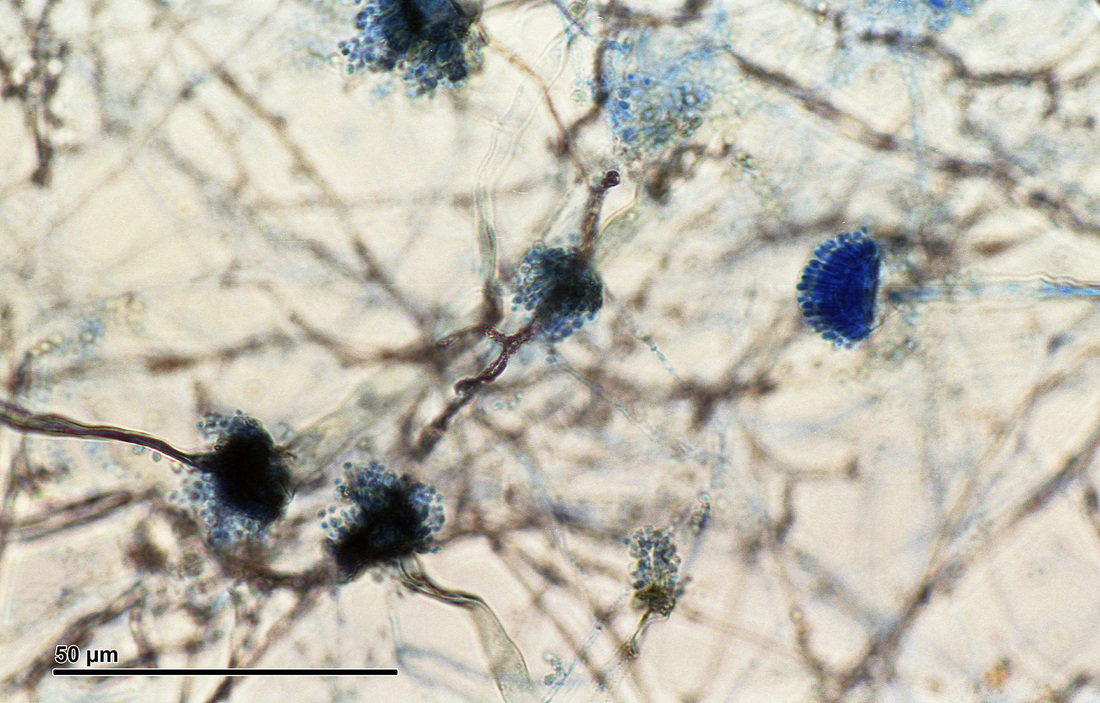
By Doc. RNDr. Josef Reischig, CSc. - Author's archive, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=30900186
|
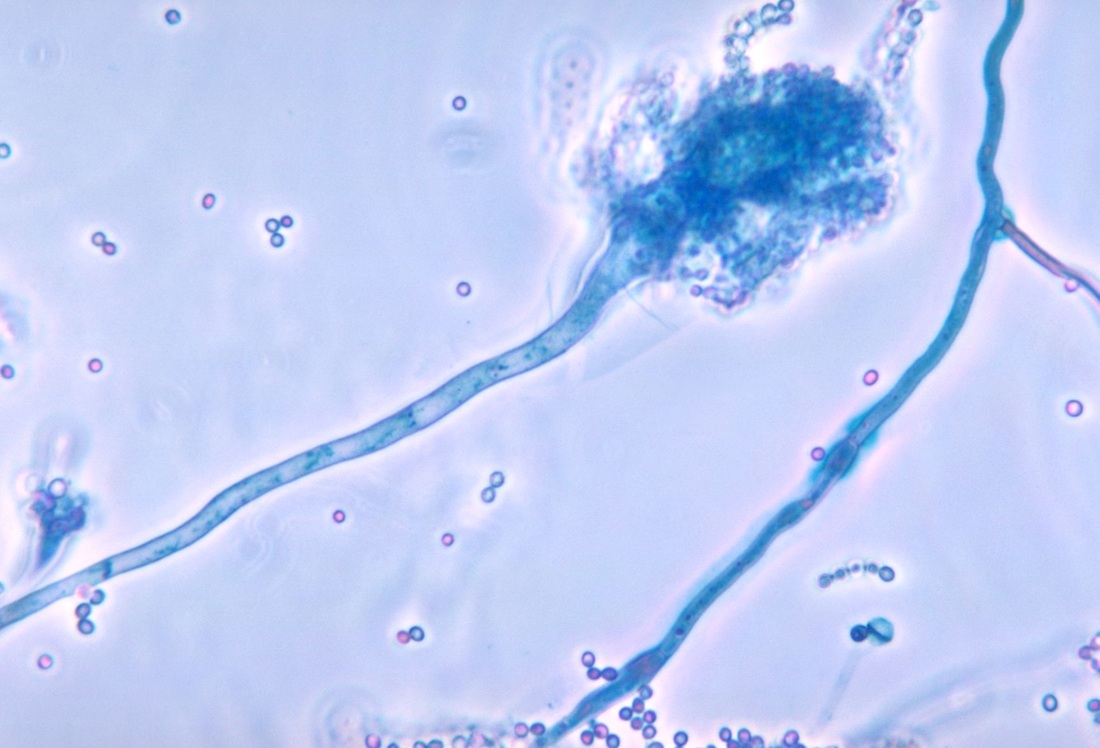
By CDC/Dr. Libero Ajello (PHIL #4297), - Obtained from the CDC Public Health Image Library., Public Domain, https://commons.wikimedia.org/w/index.php?curid=924867
|
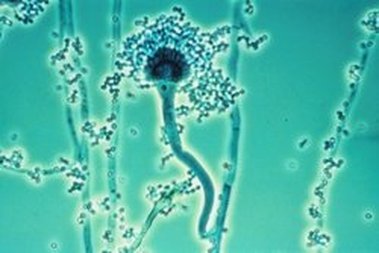
Phialides are uniseriate, typically only on the upper 2/3rds of the vesicle and they run parallel to the axis of the conidiophore.By User:Jplm, from User:Strobilomyces [Public domain], via Wikimedia Commons
|
https://upload.wikimedia.org/wikipedia/commons/9/9b/Aspergillus.gif
|
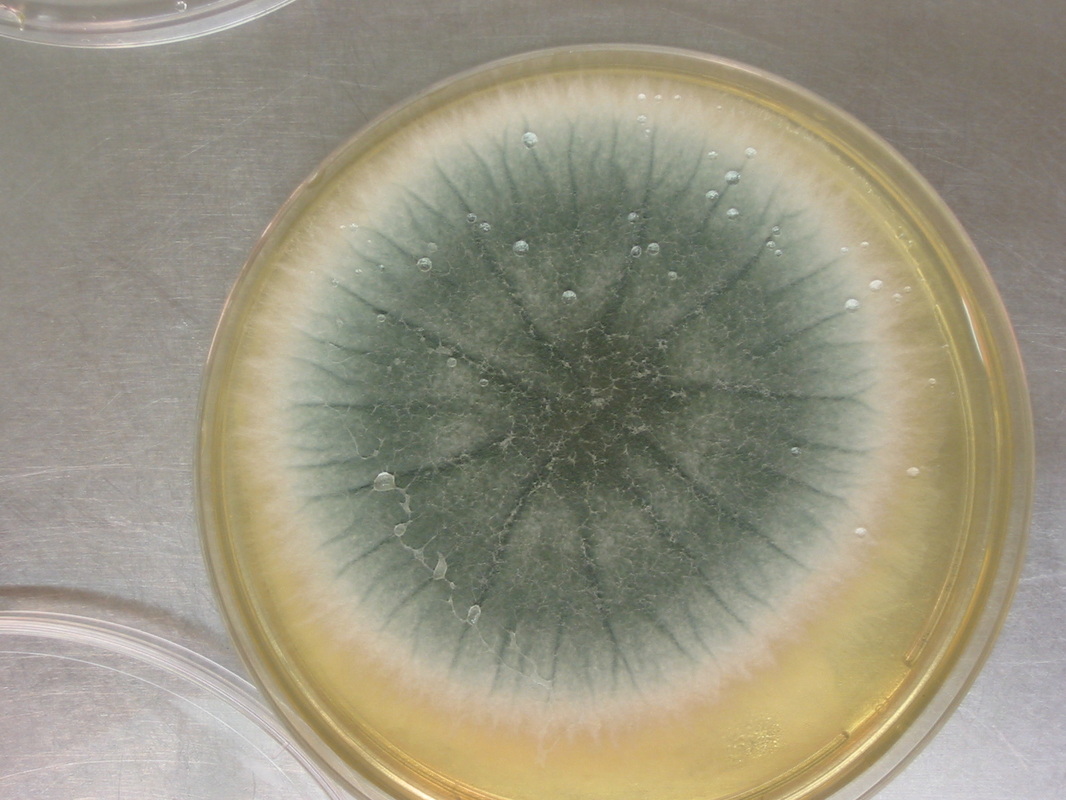
Aflatoxin production;Jankaan from nl [GFDL (http://www.gnu.org/copyleft/fdl.html) or CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/)], via Wikimedia Commons
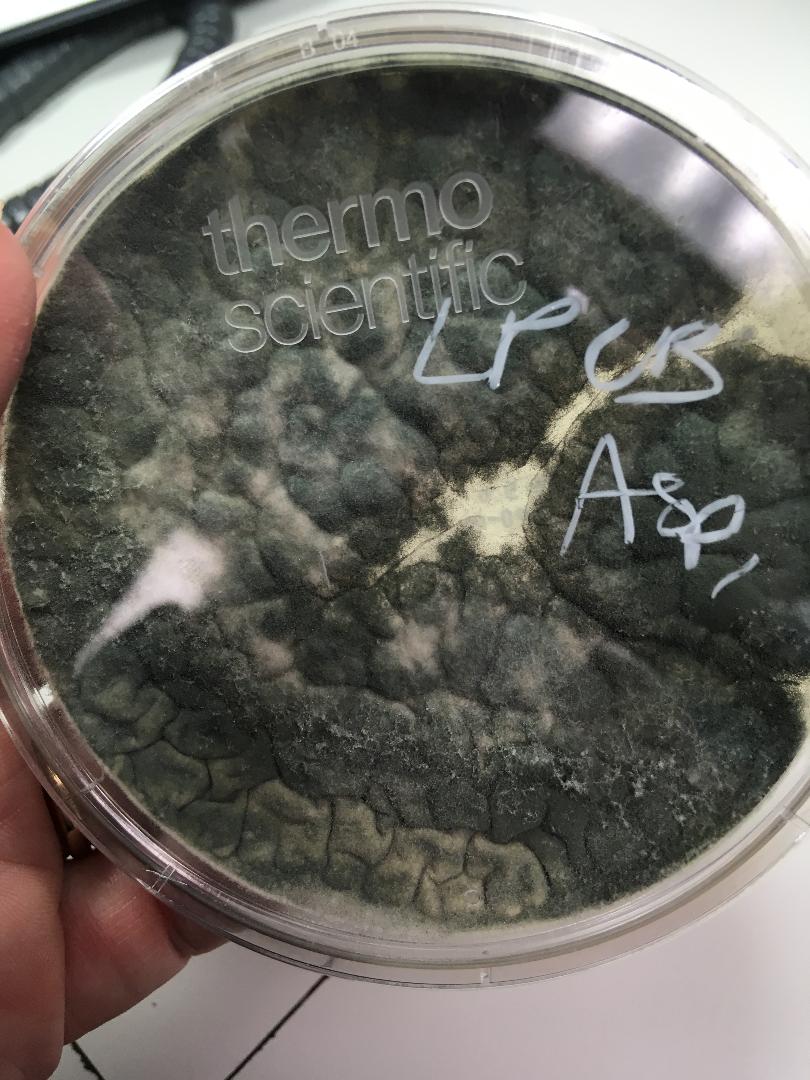
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist in a hospital laboratory
|
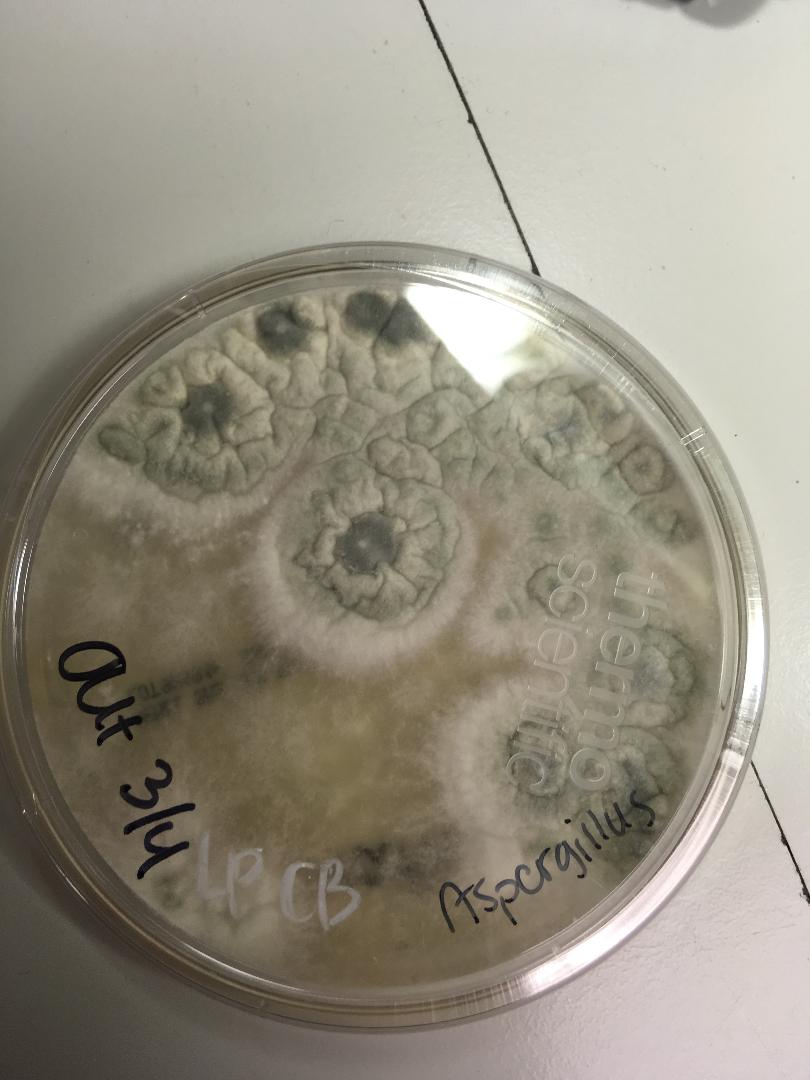
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist in a hospital laboratory
|
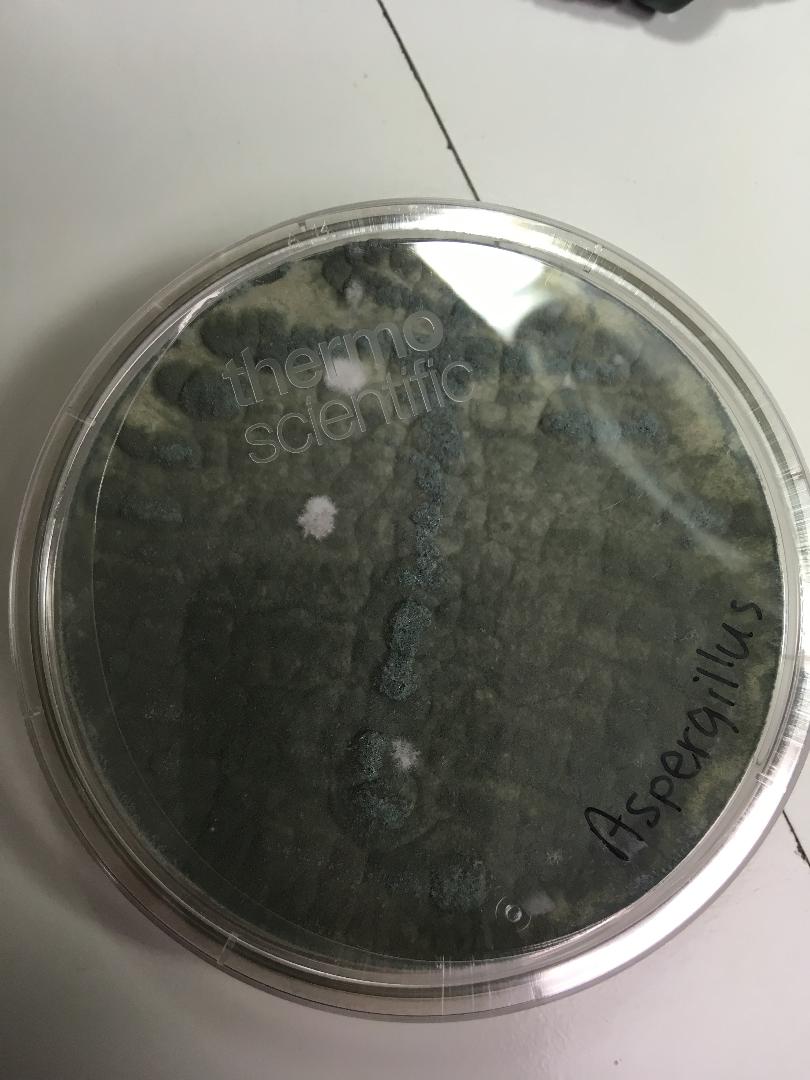
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist in a hospital laboratory
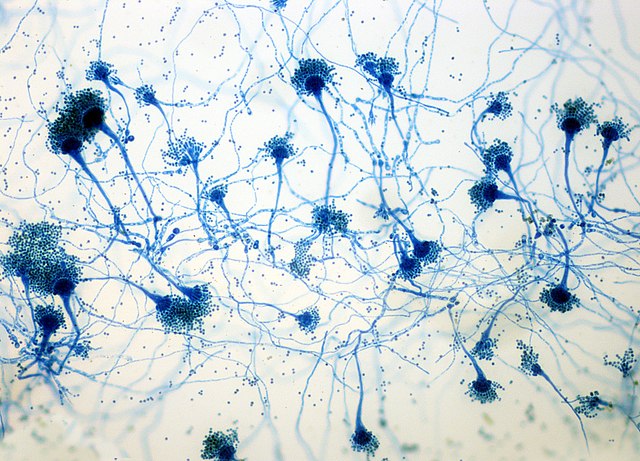
https://upload.wikimedia.org/wikipedia/commons/thumb/7/70/Aspergillus.spp.jpg/640px-Aspergillus.spp.jpg
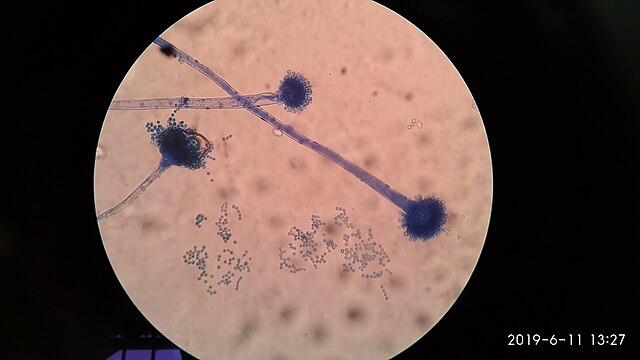
https://upload.wikimedia.org/wikipedia/commons/thumb/d/df/Conidia%2C_Strigma%2C_Vesicle%2C_and_Conidiophores_of_Aspergillus_in_LPCB_Tease_Mount_Microscopy.jpg/640px-Conidia%2C_Strigma%2C_Vesicle%2C_and_Conidiophores_of_Aspergillus_in_LPCB_Tease_Mount_Microscopy.jpg
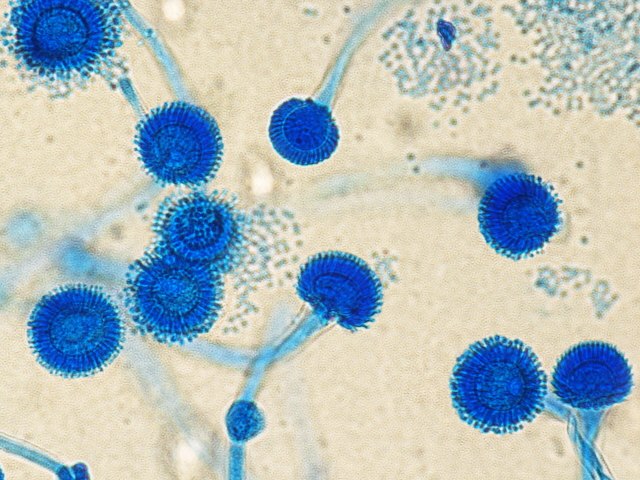
https://upload.wikimedia.org/wikipedia/commons/thumb/a/a3/Antonio_e_Biagio_e_Cesare_Arrigo_Aspergillus_fumigatus_01.jpg/640px-Antonio_e_Biagio_e_Cesare_Arrigo_Aspergillus_fumigatus_01.jpg
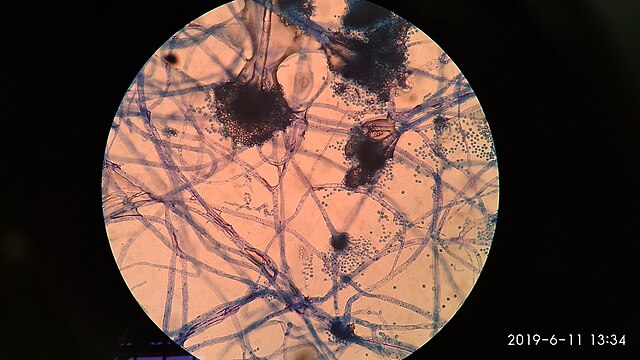
https://upload.wikimedia.org/wikipedia/commons/thumb/a/a5/Conidia%2C_sterigma%2C_vesicle%2C_conidiophores%2C_foot_cell%2C_hyphae%2C_and_mycelium_of_Aspergillus.jpg/640px-Conidia%2C_sterigma%2C_vesicle%2C_conidiophores%2C_foot_cell%2C_hyphae%2C_and_mycelium_of_Aspergillus.jpg
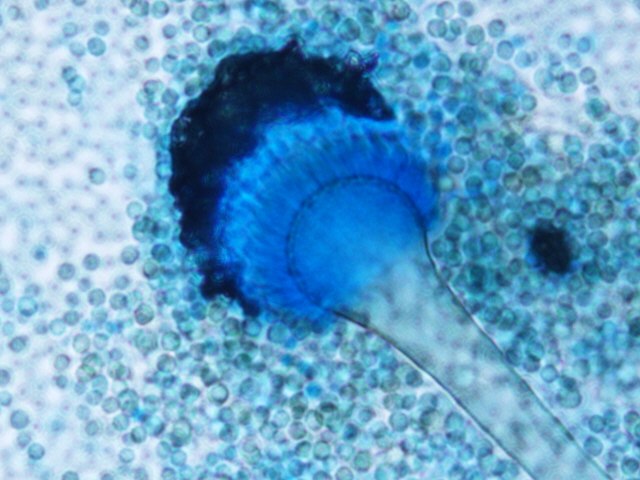
https://upload.wikimedia.org/wikipedia/commons/thumb/b/b0/Antonio_e_Biagio_e_Cesare_Arrigo_Aspergillus_fumigatus.jpg/640px-Antonio_e_Biagio_e_Cesare_Arrigo_Aspergillus_fumigatus.jpg
Aspergillus flavus:
A. flavus can be a contaminant, but it is also a causative agent of invasive aspergillosis in immunocompromised patients and patients with Cystic Fibrosis. It is also a potent allergen in those suffering from allergies and asthma. It can cause acute sinusitis of the paranasal sinuses as well. It produces aflatoxins.
Macroscopic Exam:
Microscopic Exam:
A. flavus can be a contaminant, but it is also a causative agent of invasive aspergillosis in immunocompromised patients and patients with Cystic Fibrosis. It is also a potent allergen in those suffering from allergies and asthma. It can cause acute sinusitis of the paranasal sinuses as well. It produces aflatoxins.
Macroscopic Exam:
- On agar, it grows well at 30 degrees Celsius in about one week as a flat, granular or floccose colony that is bright yellow-green with a cream reverse. It kind of looks like a lawn of mowed green grass.
Microscopic Exam:
- Microscopically, it has a rough stalk with a large head, and the conidia are oval and yellow-brown.
- Sporing heads have rough-walled conidiophores and globose vesicles with phialides in 1-2 rows over the whole surface and point out in all directions.
- Vesicles bear radiate or columnar spores.
- Conidia are round or elliptical and are rather large and numerous.
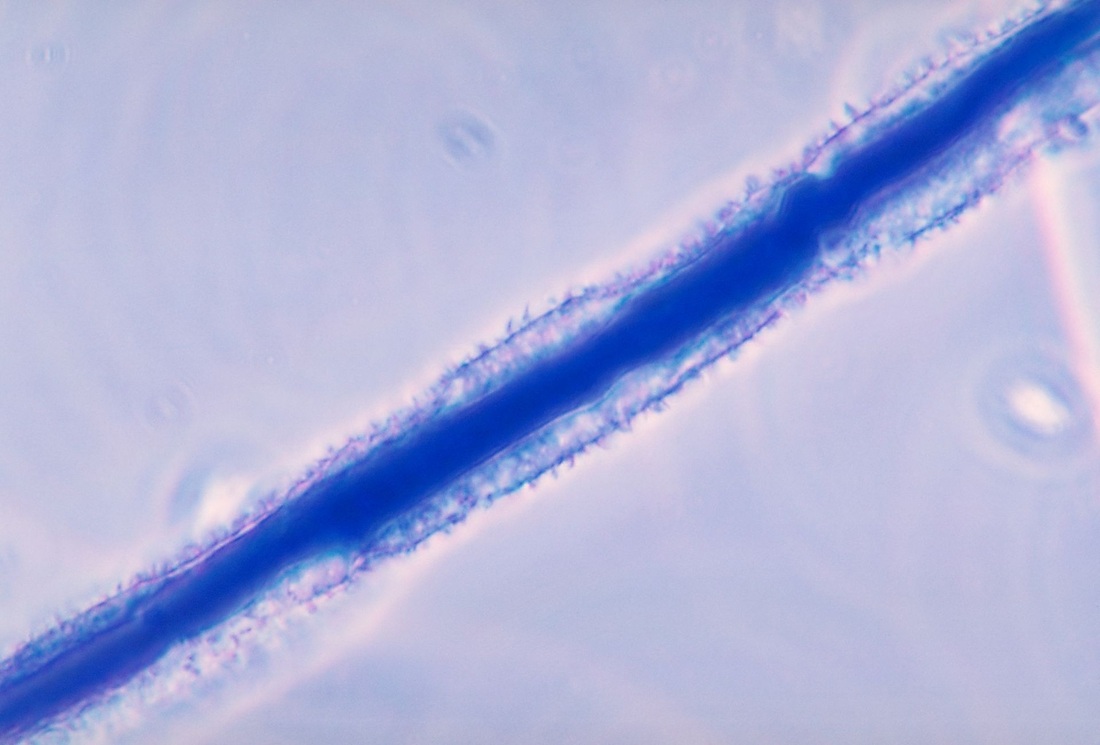
Colonies of A. flavus are velvety in texture, and color ranges from yellow to green or brown. The reverse is gold to red brown in color.By US gov - US gov, Public Domain, https://commons.wikimedia.org/w/index.php?curid=1860017
|
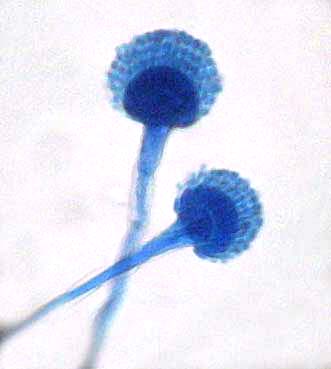
The phialides are uniserate and biseriate, and they cover the entire vesicle, pointing out in all directions.
This is seen in invasive pulmonary aspergillosis and allergic bronchopulmonary disease.
|
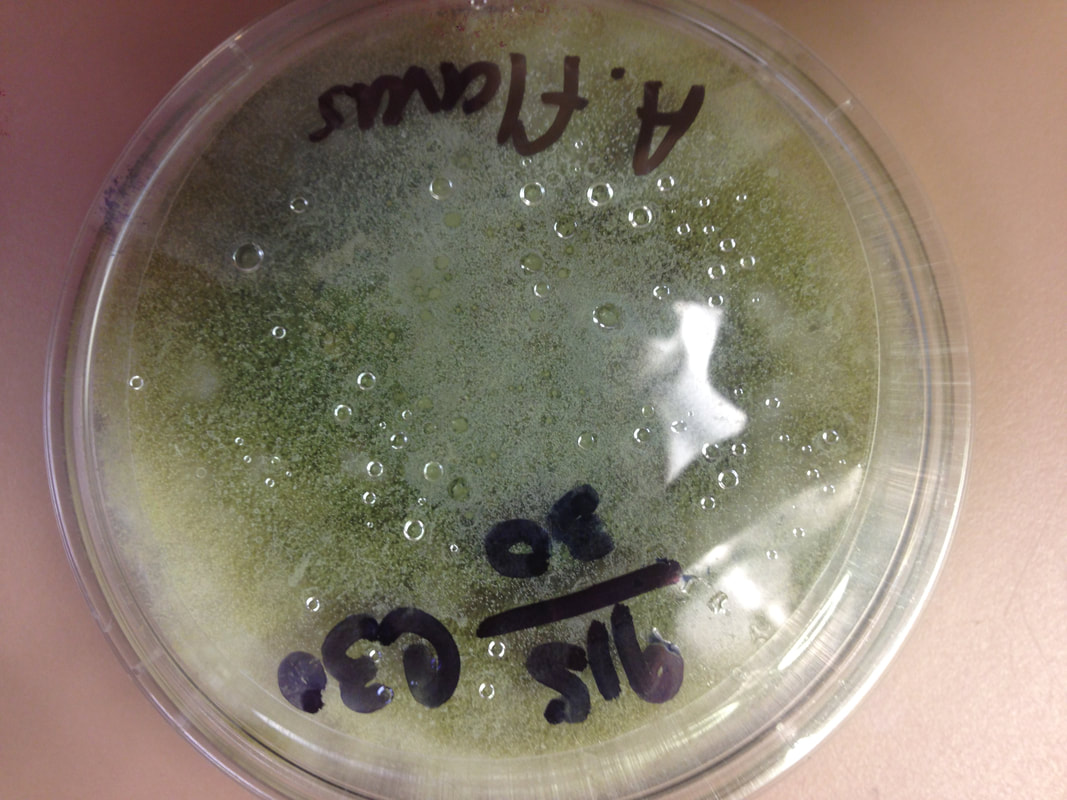
My own work by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|

My own work by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
A. flavus, image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|
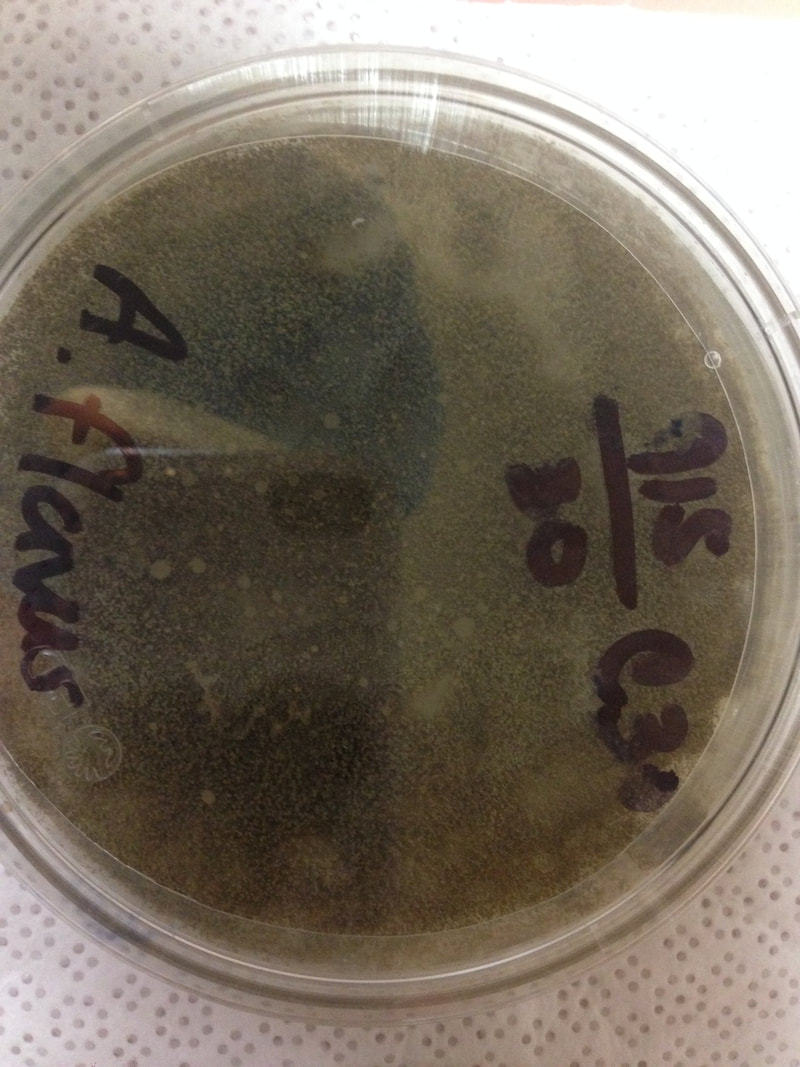
A. flavus, image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|

A. flavus, image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|
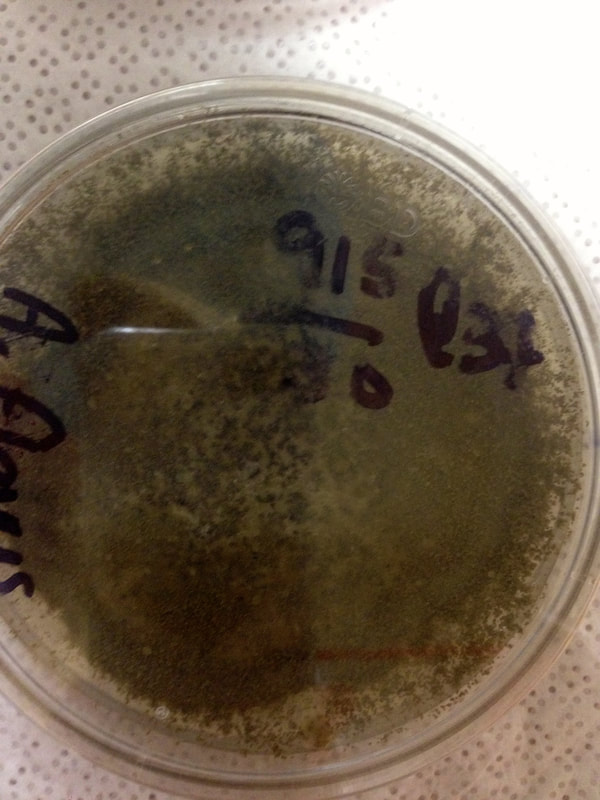
A. flavus, image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|
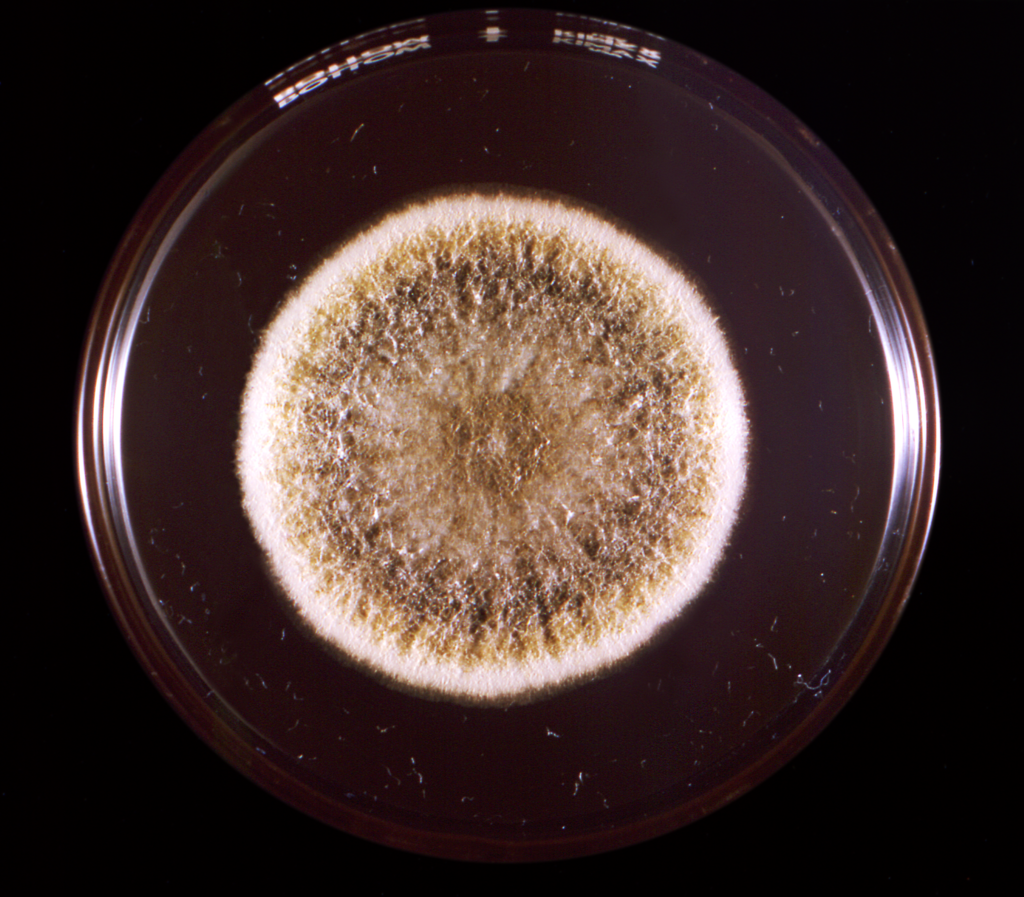
https://upload.wikimedia.org/wikipedia/commons/thumb/4/4a/Aspergillus_flavus_in_petri_dish.png/1024px-Aspergillus_flavus_in_petri_dish.png
|
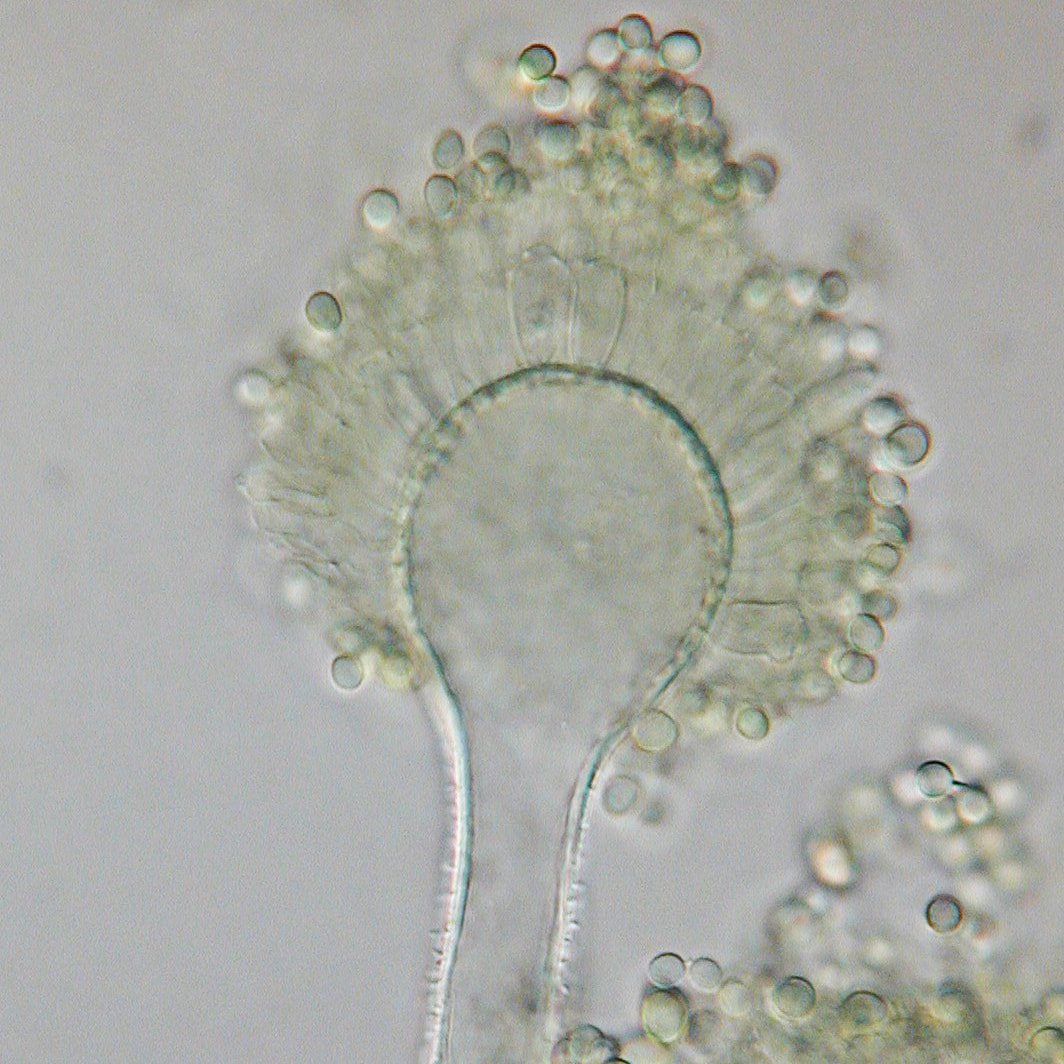
By Medmyco - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=51007285
|
Aspergillus niger:
A. niger is often a contaminant, however, it is also the most common cause of otomycosis, or outer ear infection, in individuals who are not immunocompromised. It typically does not perforate the tympanic membrane, however, its spores can be seen growing in the outer ear canal, resulting in pain, itching, swelling, redness, and scaling. In those who are immunocompromised, it can actually cause deep, invasive infections (rare; on occasion, has been known to cause fungus ball, but not as often as A. fumigatus).
Macroscopic Exam:
Microscopic Exam:
Macroscopic Exam:
- On agar, it grows in about a week at 30 degrees Celsius as a flat colony with radial folds and may be granular.
- It becomes woolly.
- It is white to yellow, developing a covering of black sporing heads, so it looks like "pepper and salt".
- The reverse is cream.
Microscopic Exam:
- Microscopically, it produces thick-walled conidiophores with smooth, colorless stalks bearing large, round vesicles with biseriate phialides and metulae over the entire radial surface forming a "radiate head".
- It resembles a dandelion.
- Conidia are round-to-oval and roughened.
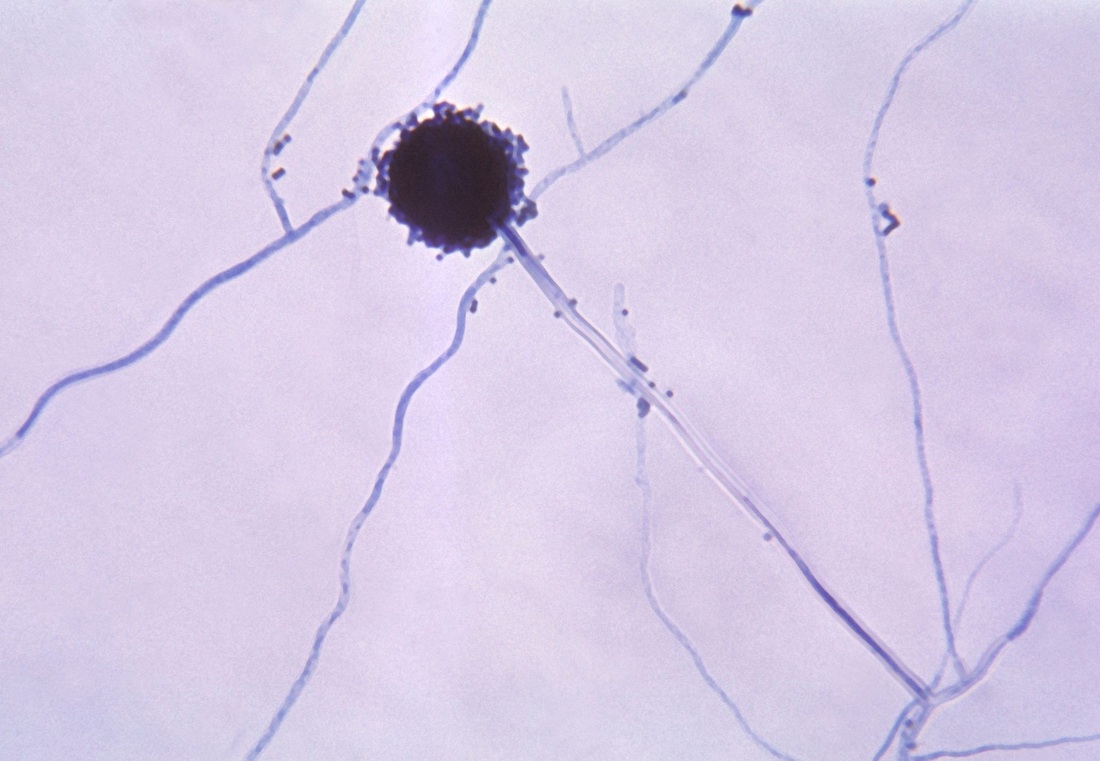
Conidiophores are long and smooth. Phialides are biseriate, and they cover the entire vesicle, forming a "radiating" head.Public Domain, https://commons.wikimedia.org/w/index.php?curid=1021866
|
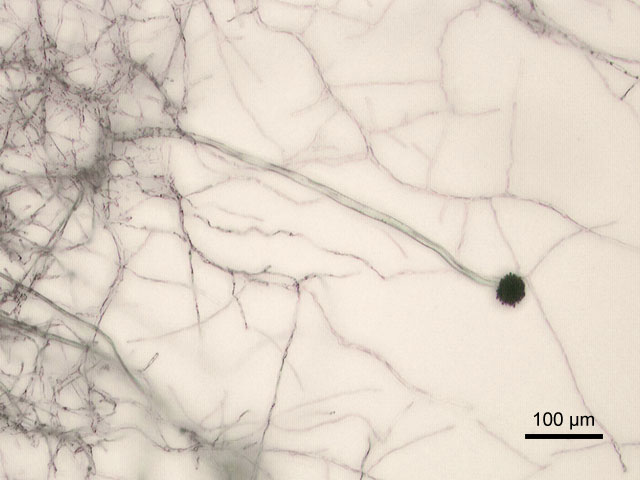
A. niger is associated with fungus ball production and otomycosis.By No machine-readable author provided. Y tambe assumed (based on copyright claims). [GFDL (http://www.gnu.org/copyleft/fdl.html) or CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/)], via Wikimedia Commons
|
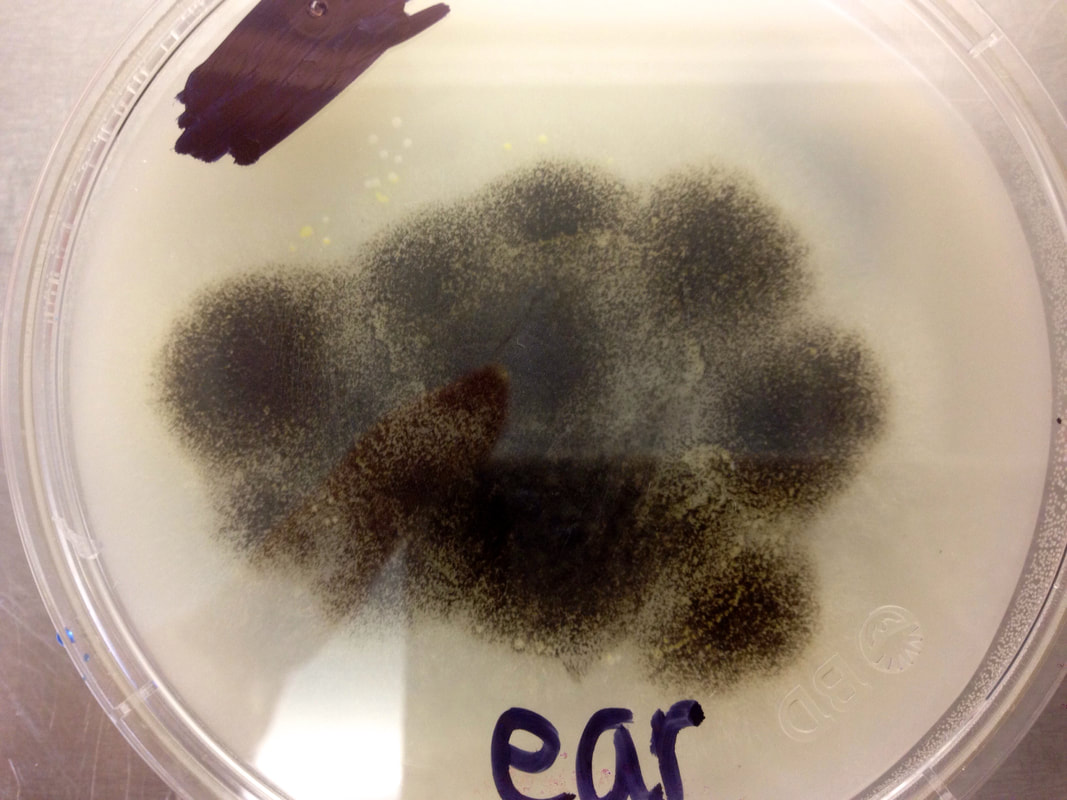
A. niger, image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|
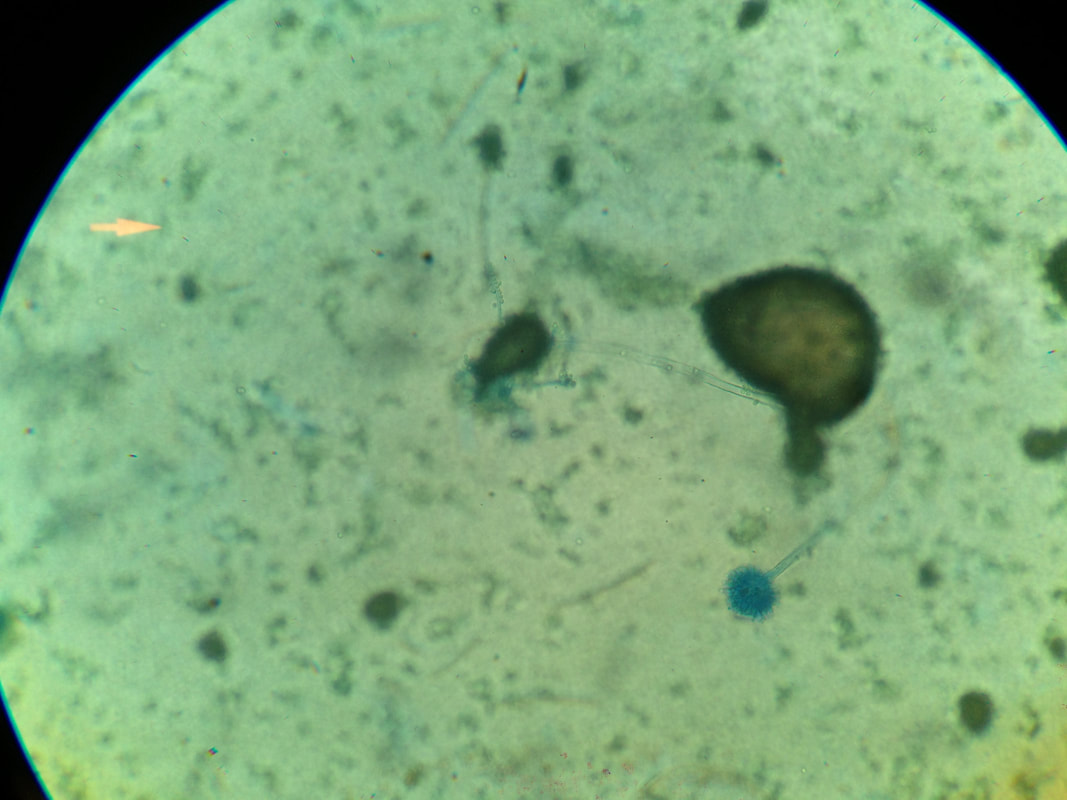
A. niger, image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|
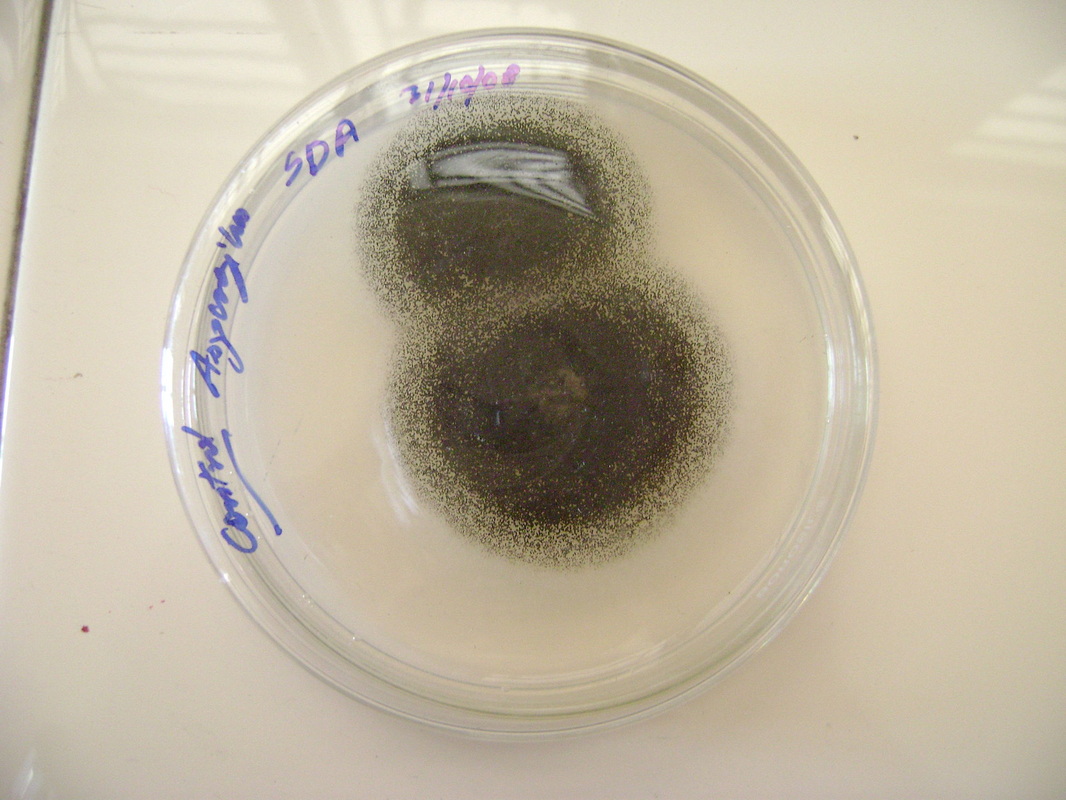
Colonies are woolly and they begin as white to yellow, turning to black with age, giving the colony a "salt and pepper" appearance. The reverse is white to yellow.By Proquence at English Wikipedia, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=16667258
|

This image shows A. niger colonies being inhibited by garlic.By Matthias M. - Flickr: IMG_8199, CC BY-SA 2.0, https://commons.wikimedia.org/w/index.php?curid=13619852
|

By Alextrevelian 006 at English Wikipedia - Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=21641846
|

The aerial and vegetative hyphae of A. niger.By Y_tambe (Y_tambe's file) [GFDL (http://www.gnu.org/copyleft/fdl.html) or CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
|

https://upload.wikimedia.org/wikipedia/commons/thumb/0/02/Aspergillus_niger_growth_on_SDA.jpg/640px-Aspergillus_niger_growth_on_SDA.jpg
|

https://upload.wikimedia.org/wikipedia/commons/thumb/5/55/Aspergillus_niger_2.jpg/1280px-Aspergillus_niger_2.jpg
|
Image of mixed molds on bread, including Aspergillus niger, taken by Jeanette Reynolds, MS-Biology, M-ASCP, MLS-AMT
Aspergillus nidulans:
A. nidulans is often considered a contaminant, however, it is also a rare cause of invasive infection in immunocompromised patients. It can also cause pale grain mycetoma.
Macroscopic Exam:
Microscopic Exam:
A. nidulans is often considered a contaminant, however, it is also a rare cause of invasive infection in immunocompromised patients. It can also cause pale grain mycetoma.
Macroscopic Exam:
- It grows in about a week at 30 degrees Celsius as a flat, velvety to powdery colony which is either dark green with yellow patches or start out as "salt and pepper" in color and turn green later.
- The reverse is deep red to purple.
Microscopic Exam:
- Microscopically, there are small, vesiculate conidiophores, large round ascocarps with red contents, and abundant Hulle cells.
- Conidiophores are smooth, brown-pigmented stalks that have distinct foot cells.
- Phialides are on the upper half and are biseriate.
- Cleistothecia may be seen within the yellow patches of Hulle cells.
- Conidia are round-to-oval.
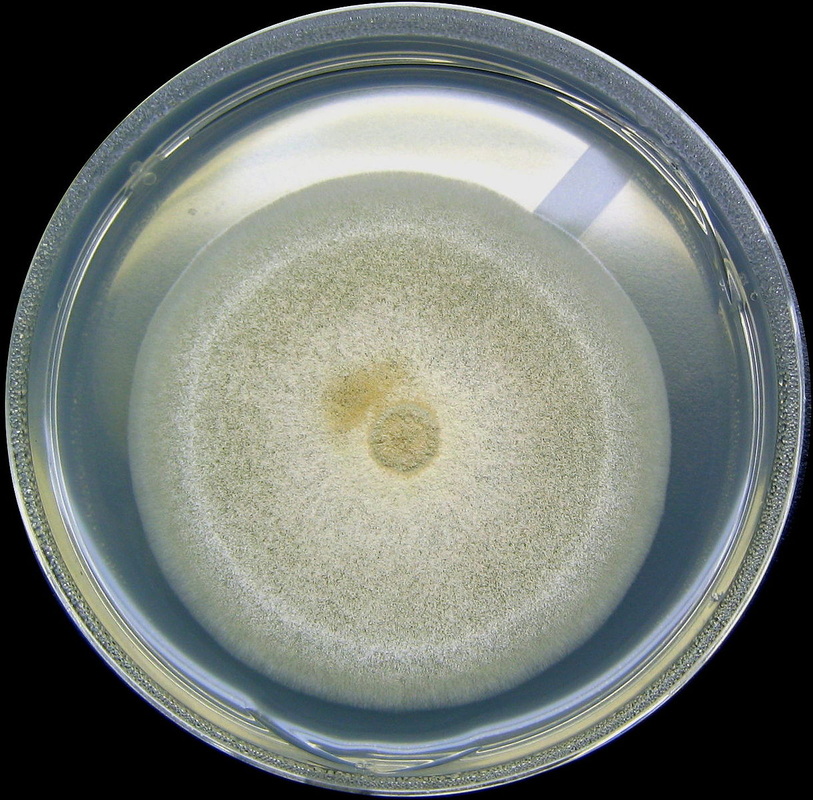
Colonies are velvety in texture, and typically green, buff to yellow in color. The reverse is purple-red, turning darker.By Plasmidmap - Transfer from English Wikipedia, CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=5563193
|

Conidiophores are short, smooth and brown. The phialides are biseriate, short columns, and cleistothecia are present and contain red-colored ascospores.By Plasmidmap (File:Aspergillus_nidulans.jpg) [CC BY 3.0 (http://creativecommons.org/licenses/by/3.0)], via Wikimedia Commons
|
The top 2 colonies on the agar plate above (PDA) are A. nidulans. The bottom 2 are A. orzye.By Adrian J. Hunter - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5832588
|
A. nidulans may also produce grass green, velvety colonies with central areas of yellow due to Cleistothecia production
|
By 222fjb - Photographed with a Panasonic DMC-FZ8, CC BY-SA 3.0, https://en.wikipedia.org/w/index.php?curid=35900210
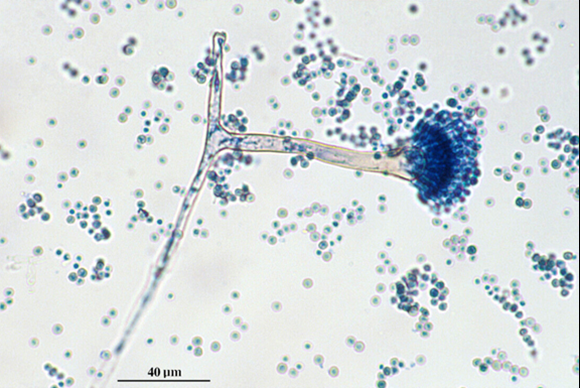
The stolon can be observed here, along with the rounded columnella

A. nidulans has thick hyphae and produces biserate phialides
|
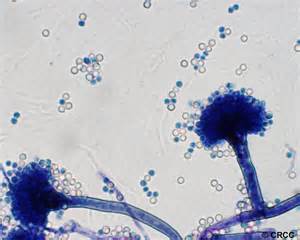
The hyphae of A. nidulans are septate
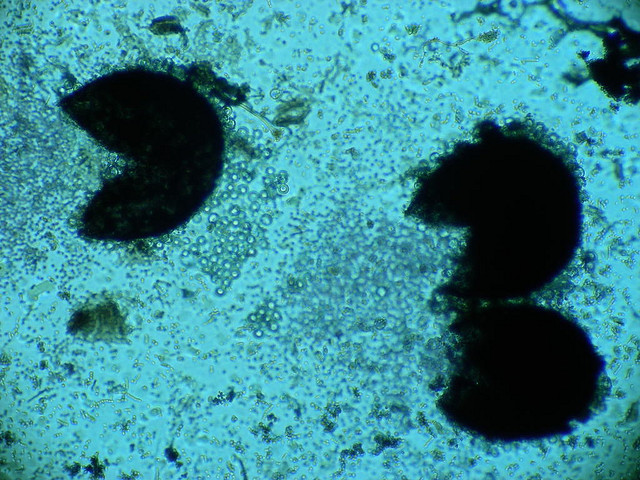
Large, open fruiting bodies of A. nidulans are seen here (Cleistothecia)
|
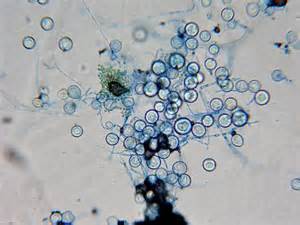
Unique to A. nidulans is the production of "Hulle cells", as seen in this image
Aspergillus terreus:
A. terreus is commonly considered a contaminant, however, it is also a common cause of onychomycosis (nail) and otomycosis (outer ear) infections. In individuals that are immunocompromised, it may cause invasive aspergillosis.
Macroscopic Exam:
Microscopic Exam:
A. terreus is commonly considered a contaminant, however, it is also a common cause of onychomycosis (nail) and otomycosis (outer ear) infections. In individuals that are immunocompromised, it may cause invasive aspergillosis.
Macroscopic Exam:
- Colonies are rapid growers and are flat, cinnamon brown to orange, granular to velvety, and have a yellow or pale brown reverse.
Microscopic Exam:
- The conidiophores are smooth, colorless stalks with dome-shaped vesicles that fan out, bearing long, cylindrical metulae and biseriate phialides on the upper 2/3rds, bearing smooth, round conidia that give it a fan-like appearance.

The conidiophores are short and smooth, and the phialides are biseriate, compact, columnar. They are round, hyaline cells supported by myecelium.
|
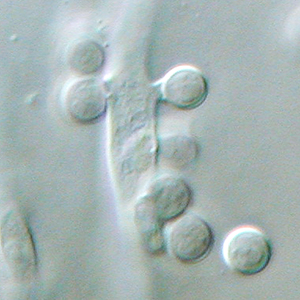
Colonies are velvety, cinnamon brown in color, and the reverse is white to brown.
|

A. terreus produces yellow-to-cinnamon colored colonies
|
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist at a hospital laboratory
Aspergillus versicolor:
Aspergillus versicolor is usually a contaminant, however, it is also a rare cause of human nail infections. It produces aflatoxins.
Macroscopic Exam:
Microscopic Exam:
Aspergillus versicolor is usually a contaminant, however, it is also a rare cause of human nail infections. It produces aflatoxins.
Macroscopic Exam:
- Colonies grow in about a week at 30 degrees Celsius and are flat, granular, floccose, or even velvety and are shades of green, yellow, light brown, or pink with a pale cream to red reverse.
Microscopic Exam:
- Microscopically, conidiophores are vesiculate with radiate heads.
- The conidiophore stalks are smooth, colorless, with round-to-oval "spoon-shaped" vesicles bearing biseriate phialades all around the entire surface.
- Conidia are round, slightly roughened, and may chain similarly to Penicillium species.
- Hulle cells may be produced.

Colonies are velvety, starting out as white, but progressing to yellow, orange, tan, green, or pink, and the reverse is white, yellow, orange or red. Conidiophores are long and smooth. The phialides are biseriate, loosely covering most of the vesicle.
|
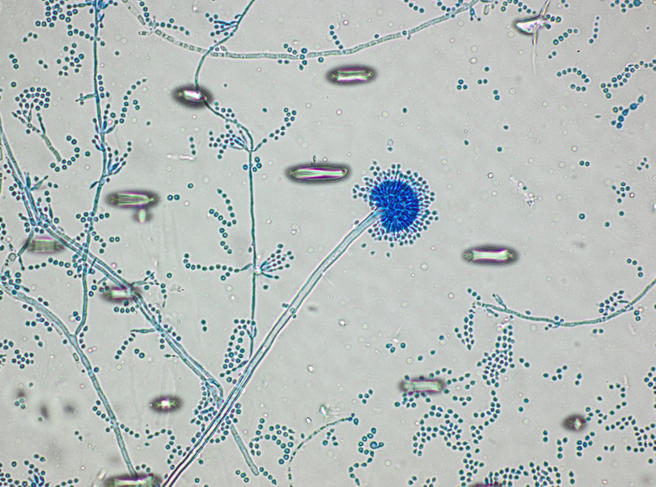
A. versicolor microscopic appearance with lactophenol cotton blue stain scotch tape prep
|
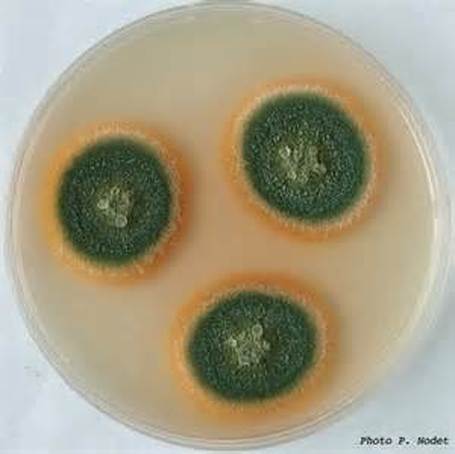
Mature A. versicolor colonies covered with green, white and orange pigmentation
|

Young A. versicolor colonies, rugose, blue-turning-green with orange pigmentation beginning in the center
|
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist at a hospital laboratory
Aspergillus candidus:
A. candidus is a rare cause of nail and ear infections. It grows as granular to floccose, white to pale cream colonies with a pale cream reverse. Colonies are flat or domed. Microscopically, there are large, vesiculate conidiophores with mixed vesiculate heads. Larger heads have large round vesicles with phialides and metulae covering the whole surface or on the upper 1/3rd only. Conidia are round-to-oval.
A. candidus is a rare cause of nail and ear infections. It grows as granular to floccose, white to pale cream colonies with a pale cream reverse. Colonies are flat or domed. Microscopically, there are large, vesiculate conidiophores with mixed vesiculate heads. Larger heads have large round vesicles with phialides and metulae covering the whole surface or on the upper 1/3rd only. Conidia are round-to-oval.

By Medmyco - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=61680001
Aspergillus clavatus:
This organism is commonly considered to be a contaminant.
Macroscopic Exam:
Microscopic Exam:
Macroscopic Exam:
- It produces wrinkled, felt-like colonies that are blue, green, or white.
- The reverse is white.
- Colonies may brown with age.
Microscopic Exam:
- Long, smooth conidiophores bear uniserate, closely crowded phialides on a big, clavate vesicle that resembles a cotton Q-tip.

Colonies are velvety, fernlike, blue or green. The reverse is white, becoming brown with age
|

The rugose, velvety colonies of A. clavatus, young growth. Colonies typically become more green with age.
|
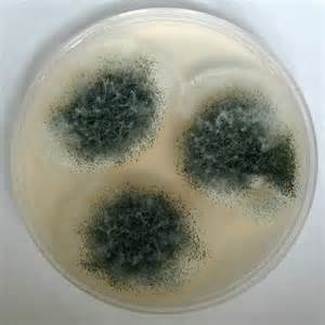
Mature A. clavatus colonies, fern-like, green, and "hairy"
|

A. clavatus colonies resembling Penicillium with the rugose green and white colonies seen above
|
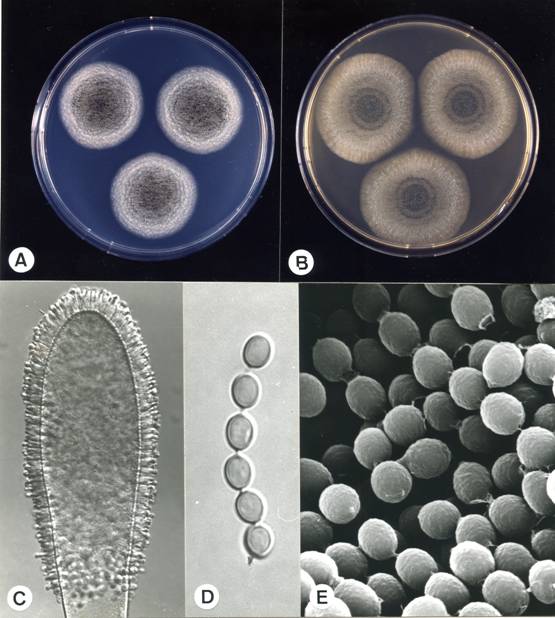
A. clavatus colonies and microscopic appearance (it resembles cotton "Q-tips")
Aspergillus glaucus:
A. glaucus group is a common environmental mold group that occasionally causes human infection.
Macroscopic Exam:
Microscopic Exam:
A. glaucus group is a common environmental mold group that occasionally causes human infection.
Macroscopic Exam:
- Colonies grow in about a week at 30 degrees Celsius, and are flat, powdery to densely floccose, and range from pale-blue-green to brown-green.
- Yellow ascocarps may also be present.
- The reverse is cream or yellow to marroon.
Microscopic Exam:
- The vesicles are thin-walled and club-shaped to round, bearing uniserate phialides that cover the entire surface of the vesicle.
- Conidiophores are vesiculate and round-to-oval with numerous small conidia.
- Ascocarps are typically present.

Colonies are feltlike, and colored green with yellow areas, occasionally brown as seen here. The reverse is yellow to maroon. Conidiophores vary in length and are smooth. Phialides are uniseriate, radiate to very loosely columnar and they cover the whole vesicle.
|
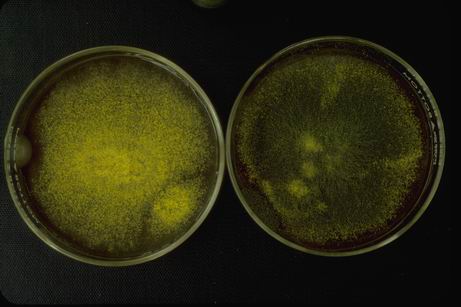
A. glaucus may grow as velvety green colonies with yellow centers due to the production of cleistothecia, which are fruiting bodies
|

This is an example of A. glaucus growth at 42 degrees Celsius. It grows at this temperature, but not as abundantly as growth at 30 and 37 degrees Celsius on SAB dextrose agar.
|
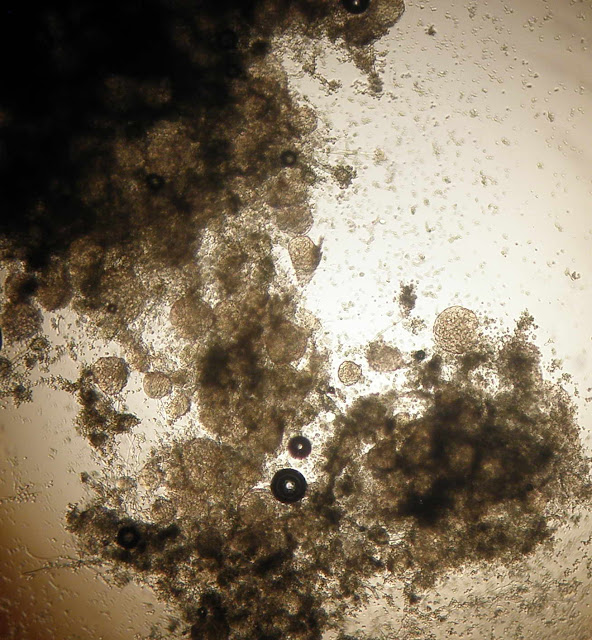
Cleistothecia production
|
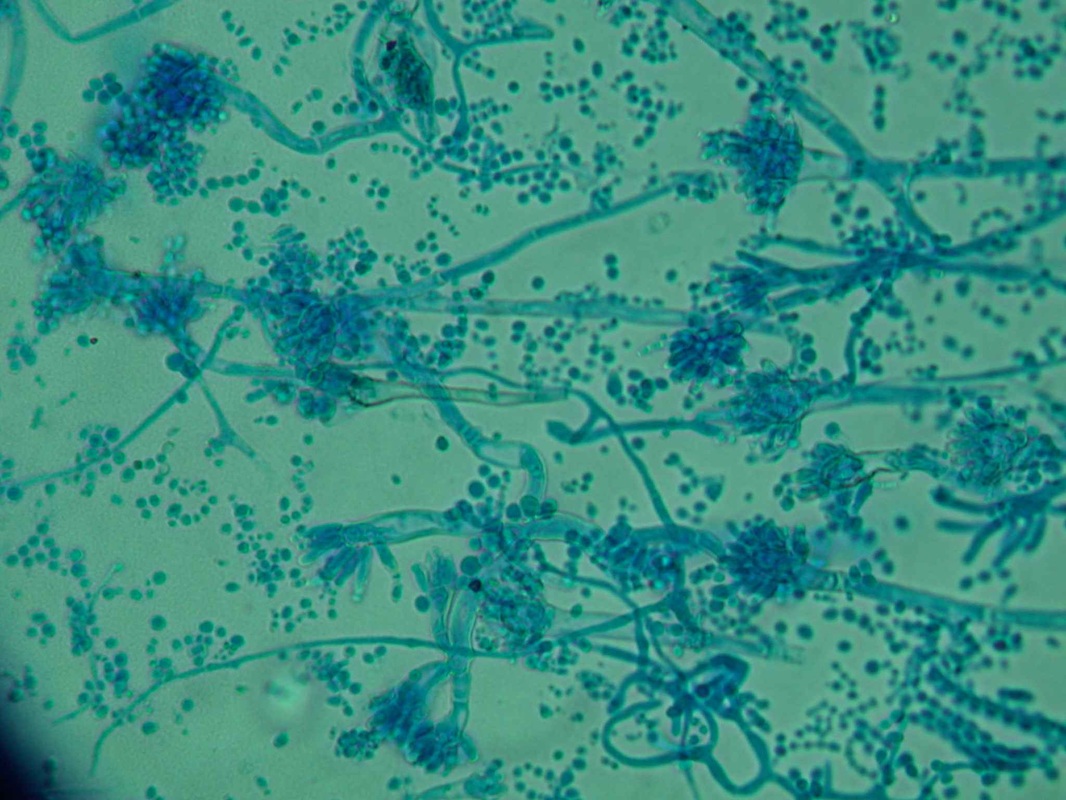
|
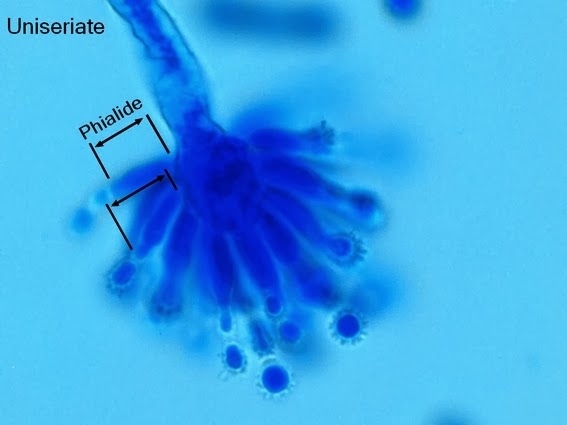
The "bowling pin" shaped uniseriate phialides of A. glaucus
|
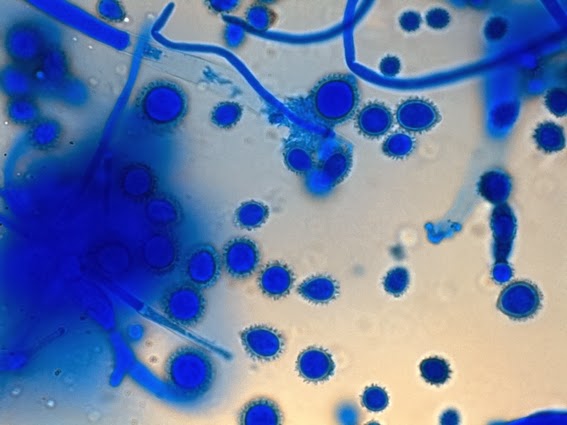
|
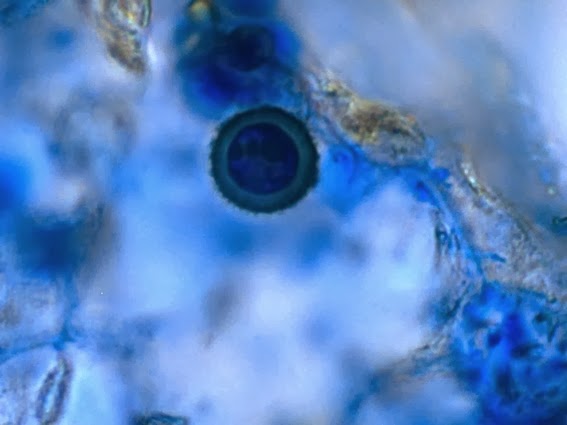
|

|
Aspergillus terreus:
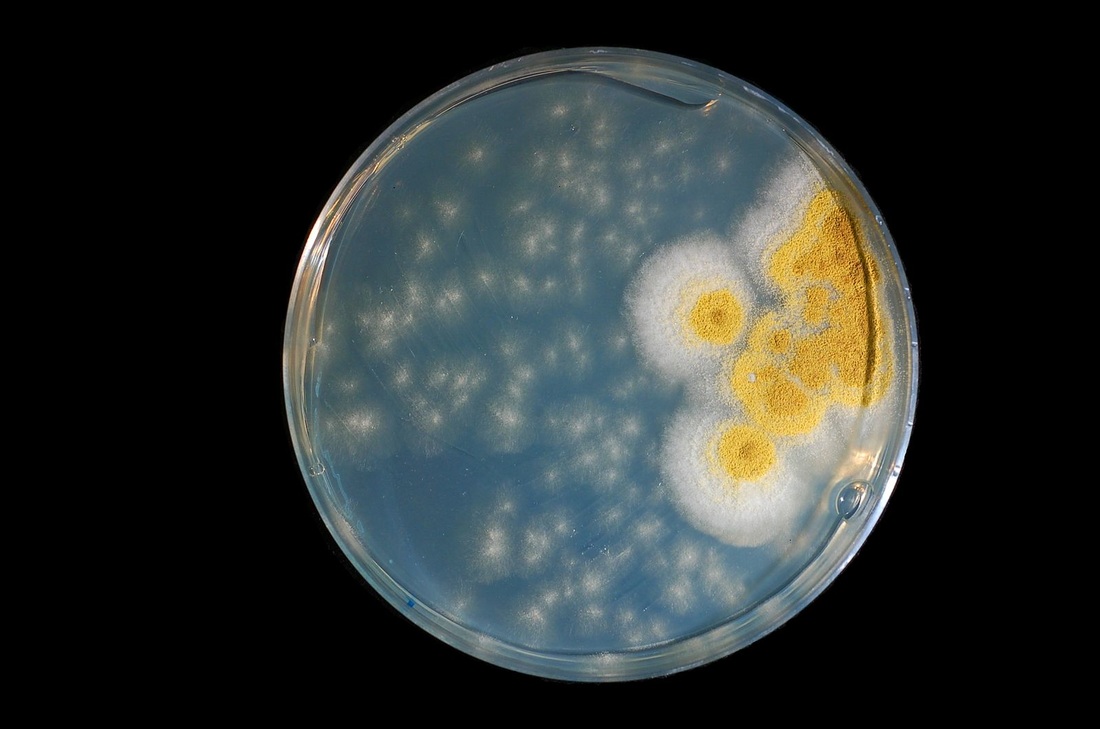
Aspergillus terreus, which produces an orange-tan colored pigment on PDA, is observed here
Aspergillosis:
Aspergillosis is a fungal illness caused by the inhalation of conidia (spores). Starting as a pulmonary disease, Aspergillus produces granulomas, which are granulomatous lesions in the lungs and/or in the bronchi. From here, the disease may become invasive, invading the surrounding blood vessels, and disseminating to other parts of the body, including the brain, gastrointestinal tract, or the kidneys, from which it is usually acute and fatal.
There is no tissue invasion in otomycosis (external ear infection) or fungus ball formation (abscess). In sensitized individuals, allergic reactions and asthma attacks may be precipitated. This is referred to as allergic bronchopulmonary disease. Other types of aspergillosis may include the following: myocarditis, meningitis, osteomyelitis, mycetoma, burn infection, nasal sinus invasion, onychomycosis, keratomycosis, and GI involvement due to toxin ingestion from eating contaminated foods.
Aspergillosis is a fungal illness caused by the inhalation of conidia (spores). Starting as a pulmonary disease, Aspergillus produces granulomas, which are granulomatous lesions in the lungs and/or in the bronchi. From here, the disease may become invasive, invading the surrounding blood vessels, and disseminating to other parts of the body, including the brain, gastrointestinal tract, or the kidneys, from which it is usually acute and fatal.
There is no tissue invasion in otomycosis (external ear infection) or fungus ball formation (abscess). In sensitized individuals, allergic reactions and asthma attacks may be precipitated. This is referred to as allergic bronchopulmonary disease. Other types of aspergillosis may include the following: myocarditis, meningitis, osteomyelitis, mycetoma, burn infection, nasal sinus invasion, onychomycosis, keratomycosis, and GI involvement due to toxin ingestion from eating contaminated foods.
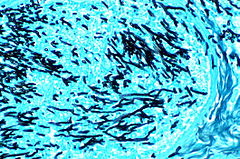
|
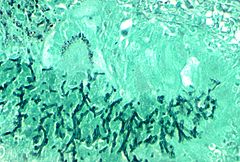
|
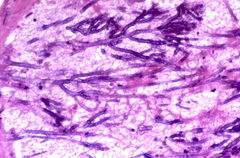

Onychomycosis, nail fungal infection, may be caused by a number of fungi, Aspergillus spp being one of many that can cause it

Otomycosis (chronic) caused by Aspergillus spp
|

Chronic Otomycosis (ear infections) caused by Aspergillus spp
|
Chrysosporium spp:
This has rarely been called a pathogen and rarely causes any type of infection. It is good to differentiate it from potential pathogens.
Macroscopic Exam:
Microscopic Exam:
This has rarely been called a pathogen and rarely causes any type of infection. It is good to differentiate it from potential pathogens.
Macroscopic Exam:
- It produces heaped, velvety, buff-colored colonies on SABHI agar at room temperature rapidly.
- It forms a white, yellow, or red-brown reverse.
Microscopic Exam:
- It forms single, round or club-shaped, smooth or rough conidia on top of short conidiophores or directly off the hyphae.
- It may form swollen arthroconidia.
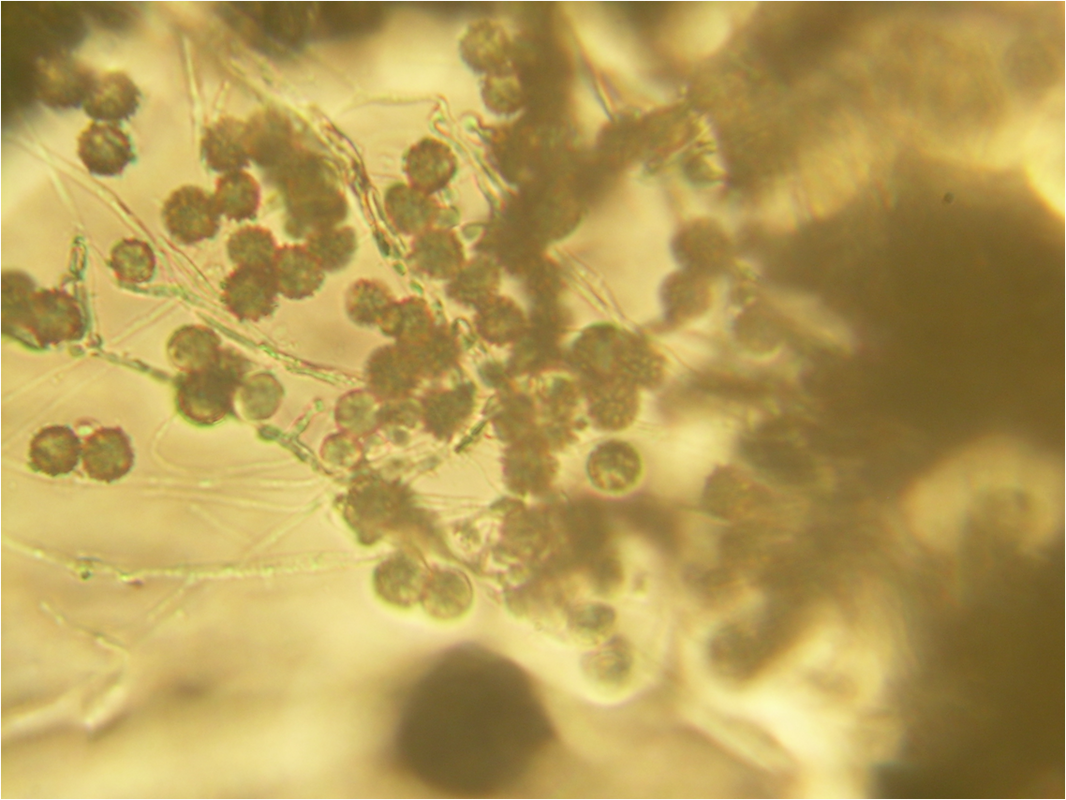
At room temperature, on SABHI agar, colonies rapidly grow as buff-colored, velvety, heaped forms. The reverse is white, yellow, or red-to-brown. Microscopically, this mold grows single, spherical-to-club-shaped, smooth or rough conidia that are supported by short conidiophores. Conidia are also able to develop right off of the hyphae. Arthroconidia that are swollen may also be present.
|

Chrysosporium colony on SAB dextrose agar
|
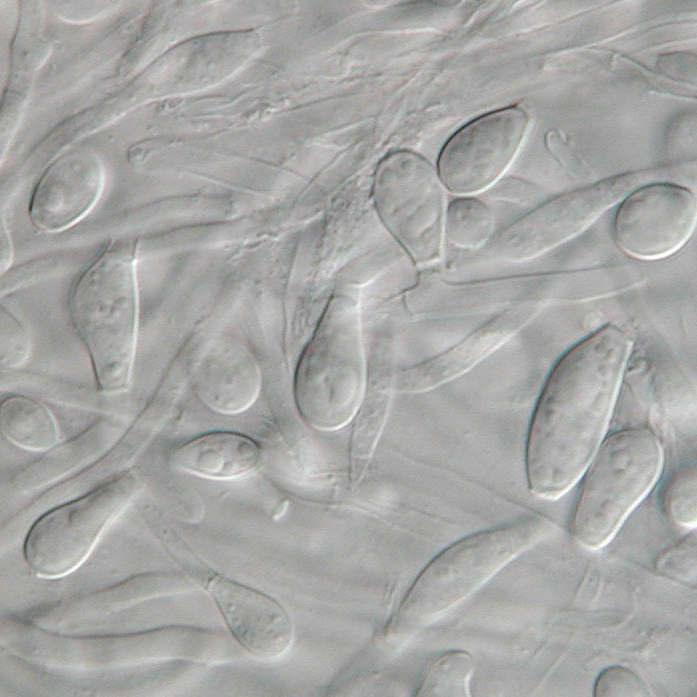
Fusarium spp:
This is a soil inhabitant, but it is also the most common cause of keratomycosis (eye infection, typical of cornea). It has also been linked to skin lesion infections in burn patients, onychomycosis (nail infections), otomycosis (ear infections), corneal infections, varicose ulcers, mycetoma, osteomyelitis with traumatic injury, and disseminated/systemic infection. It produces mycotoxins that have contaminated cereal crops, and can harm human health if they enter the food chain.
Macroscopic Exam:
Microscopic Exam:
This is a soil inhabitant, but it is also the most common cause of keratomycosis (eye infection, typical of cornea). It has also been linked to skin lesion infections in burn patients, onychomycosis (nail infections), otomycosis (ear infections), corneal infections, varicose ulcers, mycetoma, osteomyelitis with traumatic injury, and disseminated/systemic infection. It produces mycotoxins that have contaminated cereal crops, and can harm human health if they enter the food chain.
Macroscopic Exam:
- It grows as a fluffy, cottony or woolly, white mold, with tinges of pink-to-lavender color on SABHI agar at room temperature.
- It produces a light reverse.
Microscopic Exam:
- Microscopically, it produces 2-5-celled, sickle/banana/canoe-shaped macroconidia on septate hyphae with foot cells.
- Conidiophores are single or branching and occasionally produce whorls.
- The conidiophores end in tapered phialides.
- Microphialoconidia are tiny one-celled, oval spores that occur in balls at the end of tapered conidia.

The reverse is light.
|
On SABHI at room temperature, this colony is rapidly-growing and white at first, cottony or woolly, becoming lavender with age, as seen in the center of the colony here. Sometimes, it becomes yellow or orange with maturity. Colonies may be granular, and sometimes mature into pink-to-salmon color.
|
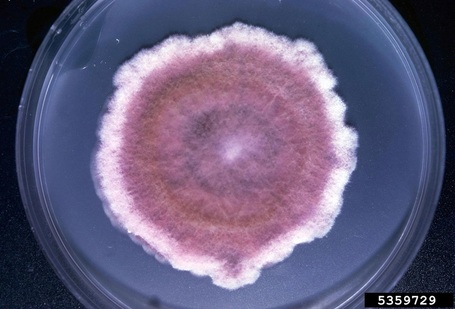
|
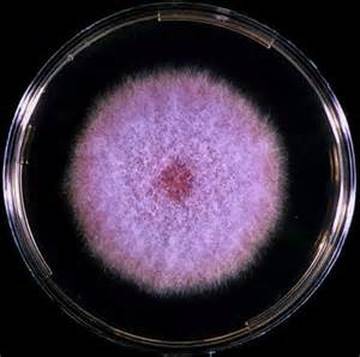
|
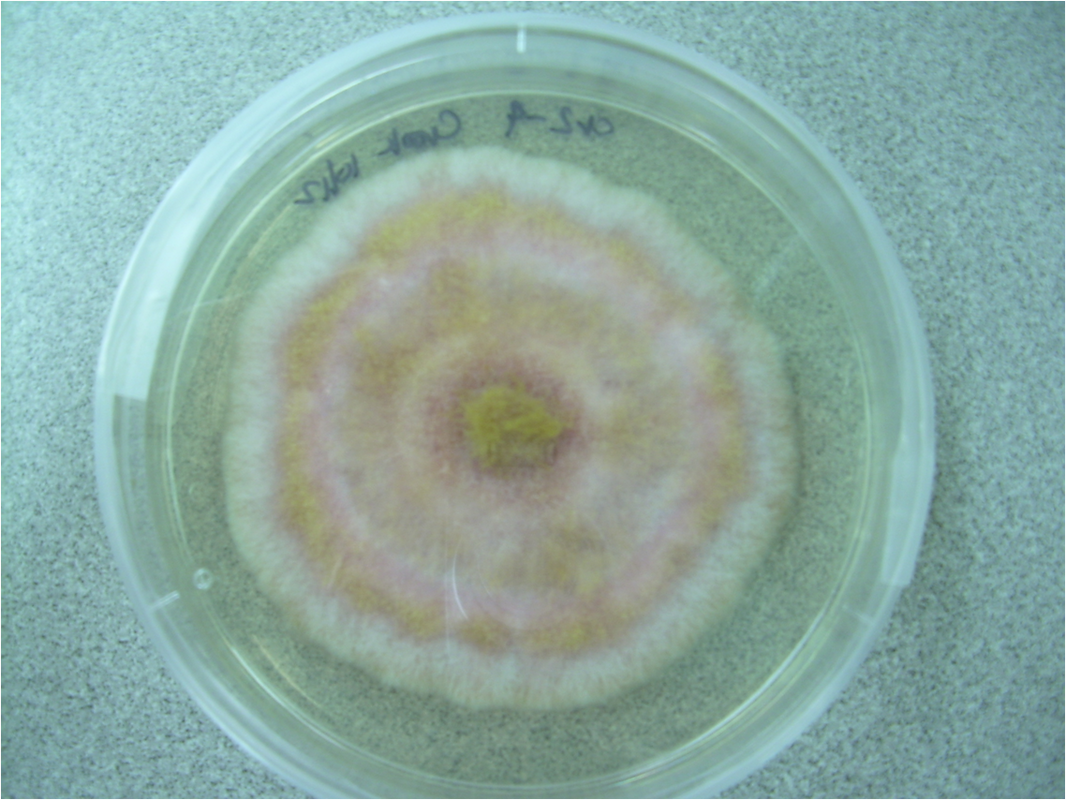
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist
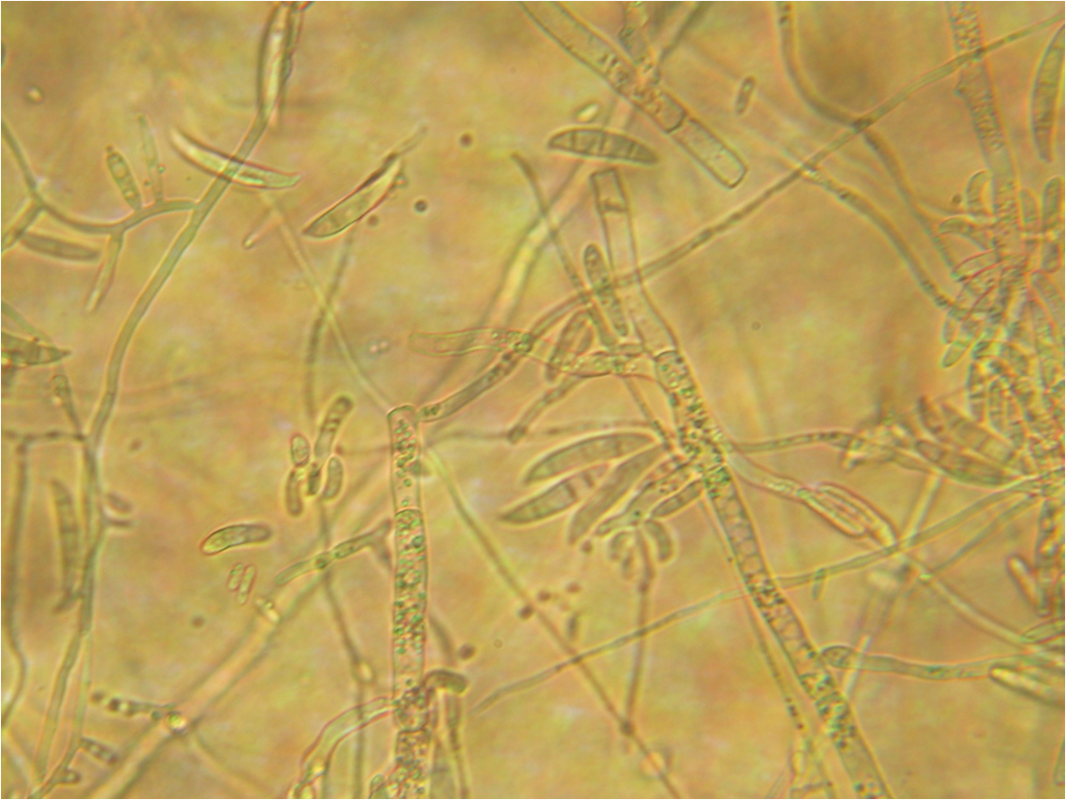
Fusarium spp mycelium have septate hyphae, with branching or unbranching conidiophores, terminating in phialides that taper. Balls of one-celled microphialoconidia also exist. Macrophialoconidia are 2 to 5-celled banana, crescent, sickle or cylindrical-shaped with a characteristic foot cell at the point of attachment.By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6658991
|
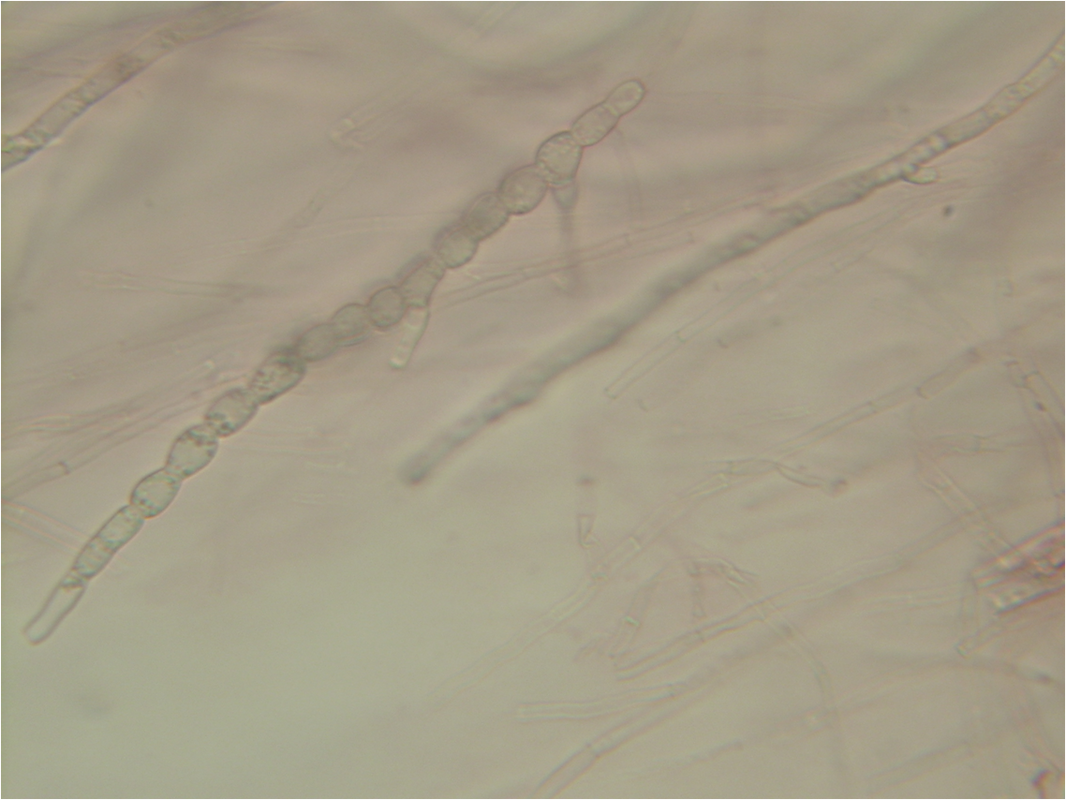
By Ninjatacoshell (Own work) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0) or GFDL (http://www.gnu.org/copyleft/fdl.html)], via Wikimedia Commons
|
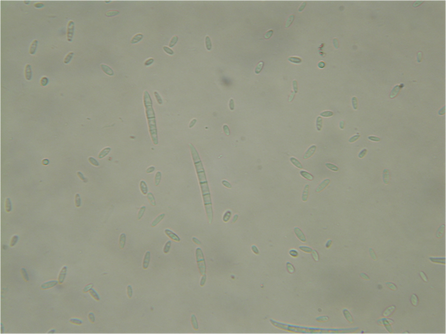
Fusarium spp macroconidia
|

"Sickle" appearance of Fusarium spp;By Fred Brooks from United States University of Hawaii at Manoa - Fusarium solani (Mart.) Sacc., CC BY 3.0 us, https://commons.wikimedia.org/w/index.php?curid=34027562
|
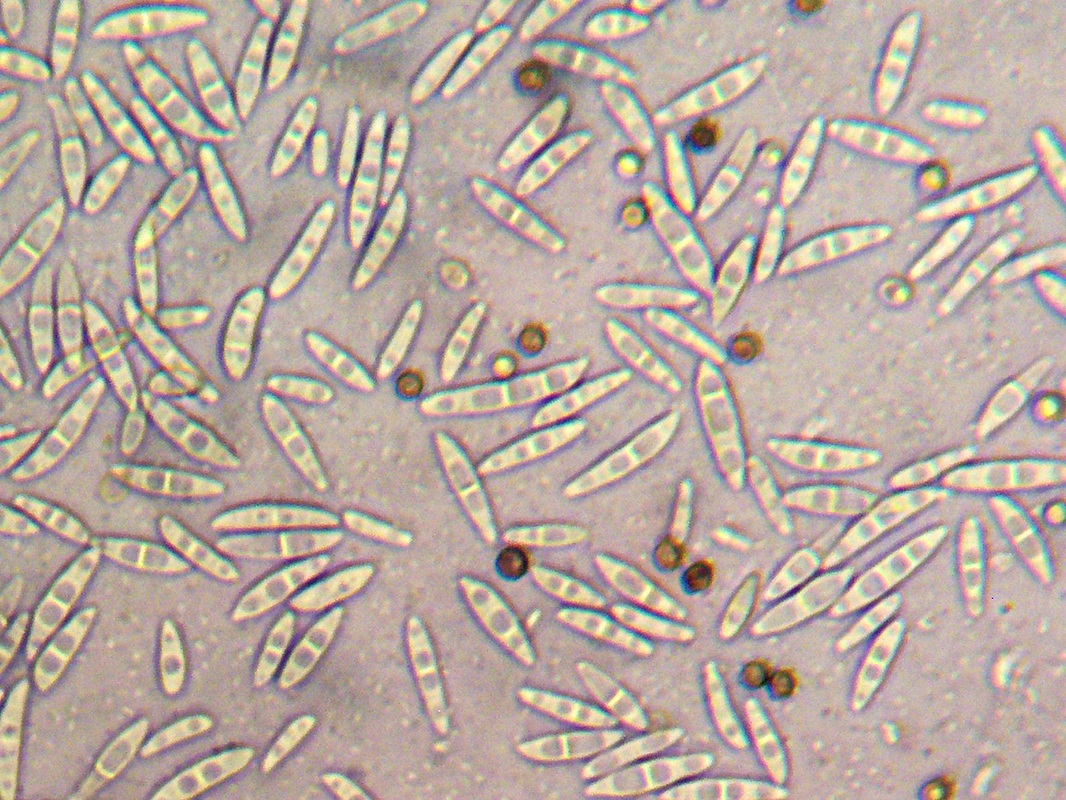
Fusarium spp macroconidia
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist at a hospital laboratory
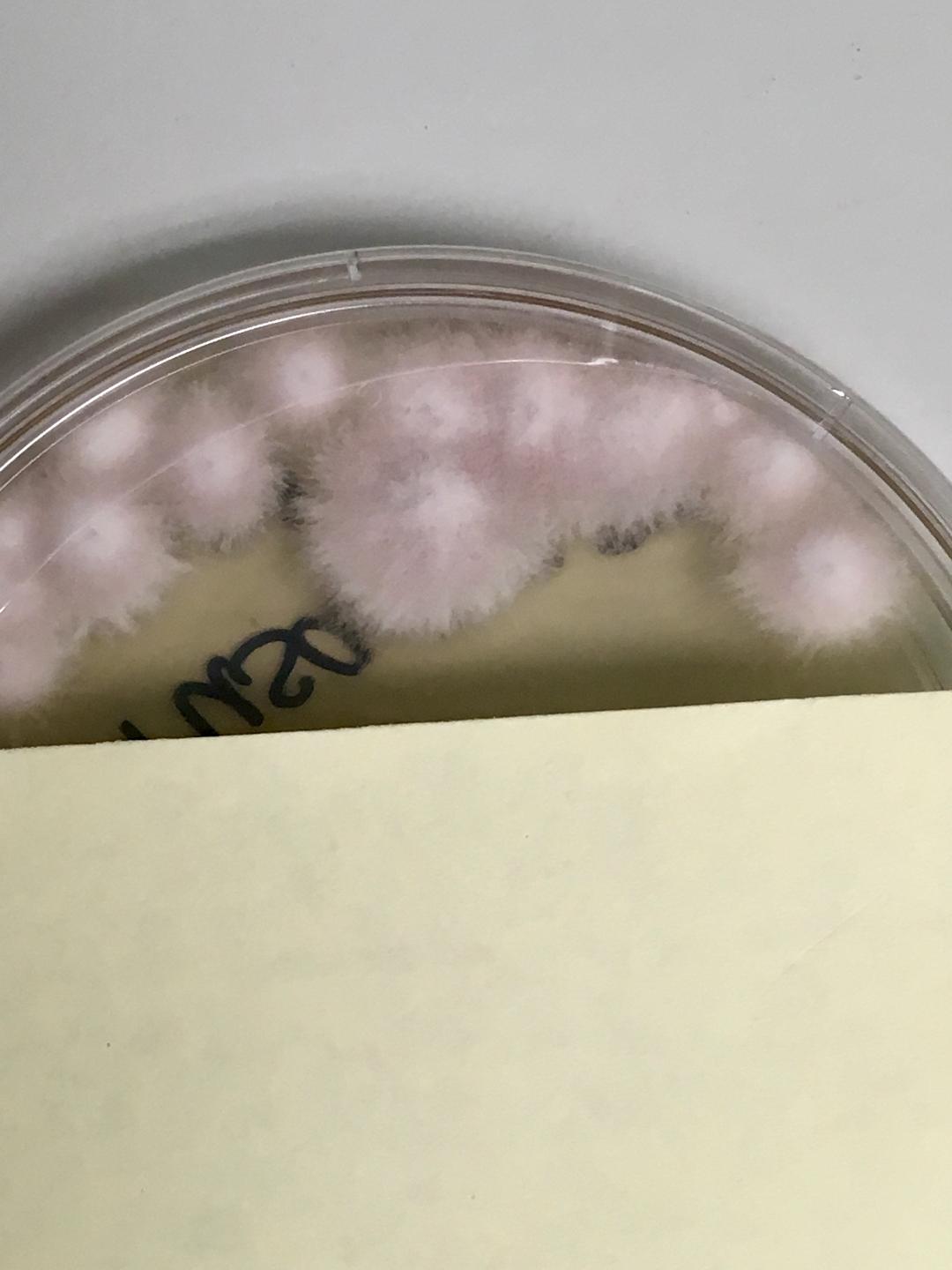
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist at a hospital laboratory

https://upload.wikimedia.org/wikipedia/commons/thumb/f/f9/K7725-1-sm.jpg/1024px-K7725-1-sm.jpg
Gliocladium spp:
This is not known to be pathogenic to humans and is commonly known as a contaminant.
Macroscopic Exam:
Microscopic Exam:
This is not known to be pathogenic to humans and is commonly known as a contaminant.
Macroscopic Exam:
- On SABHI agar at room temperature, colonies are initially white, but they quickly grow and mature to fill the plate with furry, green growth that looks like a green grass lawn.
- A few strains may actually remain white, or they may turn a rose color.
- The reverse is white.
Microscopic Exam:
- Microscopically, brushlike conidiophores bear vase-shaped phialiades that produce terminal masses of phialoconidia ranging from hyaline to green in color.
- They are held together in a large ball by a gelatinous matrix.

Paecilomyces spp:
This organism is the causative agent of penicilliosis, endophthalmitis, endocarditis, pleural effusion, or skin lesions.
Macroscopic Exam:
Microscopic Exam:
This organism is the causative agent of penicilliosis, endophthalmitis, endocarditis, pleural effusion, or skin lesions.
Macroscopic Exam:
- At room temperature on SABHI agar, colonies grow as cottony, powdery or velvety and quickly mature to an olive tan, brown or violet color.
Microscopic Exam:
- This is microscopically similar to Penicillium spp, however, it has metulae supporting elongated, flat phialides bearing chains of lemon/oval-shaped conidia and is "daintier" than Penicillium spp.
- Resembles a "paintbrush"

Elongated phialides (single, whorled or penicillus-like) bear chains of smooth or rough, hyaline to pigmented oval-shaped conidia.
|
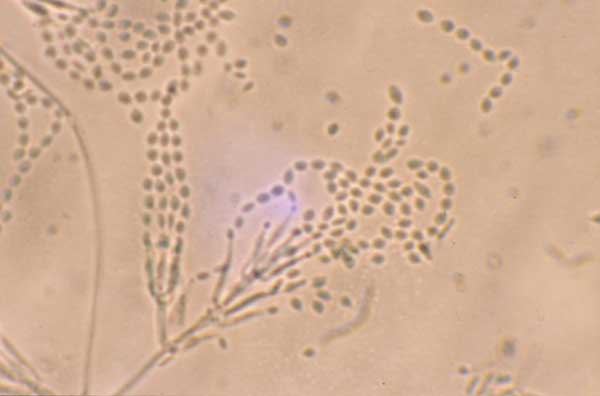
By Author not explicitly stated. Article is by Jeanne Carey, Ron D’Amico, Deanna A. Sutton, and Michael G. Rinald - "Paecilomyces lilacinus Vaginitis in an Immunocompetent Patient". Emergin Infectious Diseases. Volume 9, Number 9, September 2003, Public Domain, https://commons.wikimedia.org/w/index.php?curid=5725171
|
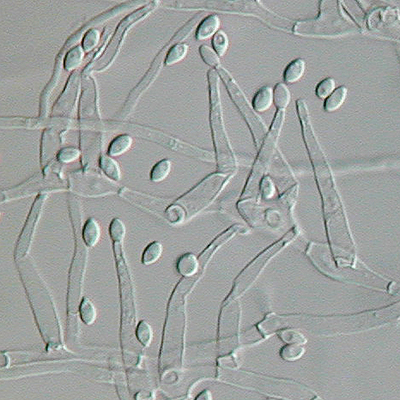
By Medmyco at English Wikipedia - Transferred from en.wikipedia to Commons., CC0, https://commons.wikimedia.org/w/index.php?curid=30364183
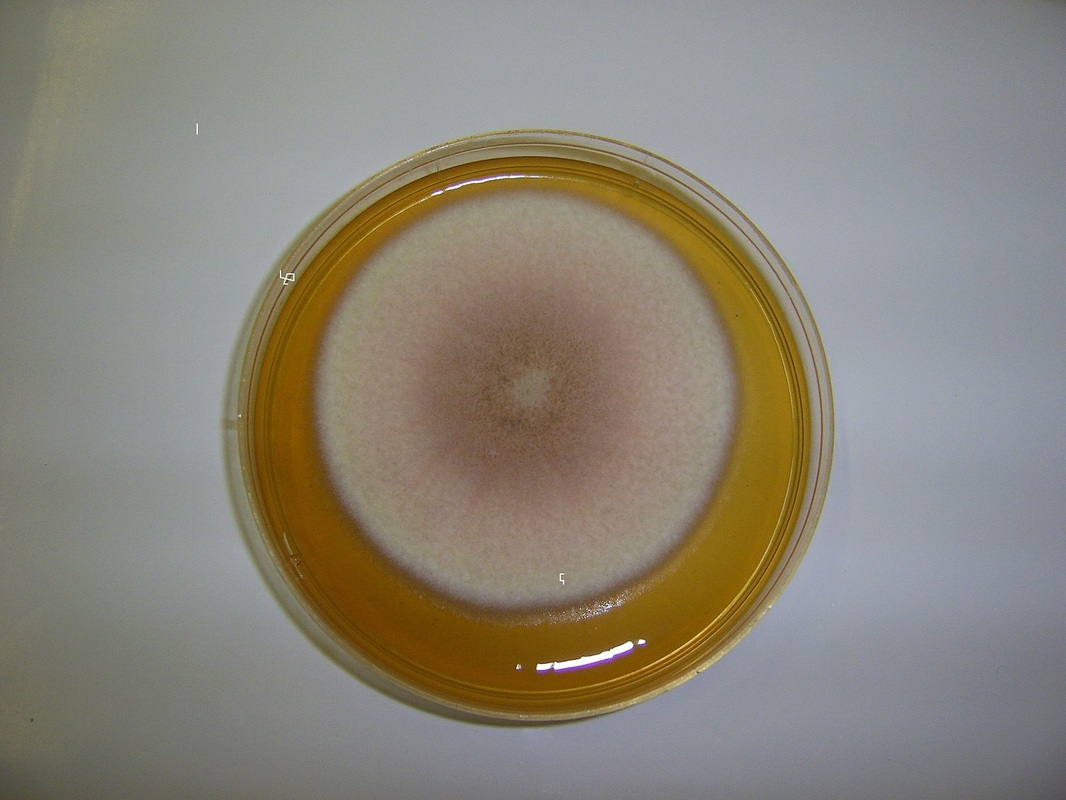
By Чхиквадзе Василий Мауглиевич - Own work, GFDL, https://commons.wikimedia.org/w/index.php?curid=22767994
Penicillium spp:
This is commonly considered a contaminant, but can be a causative agent of keratomycosis, penicilliosis, otomycosis, onychomycosis, respiratory, urinary tract infections, endocarditis, and deep infections (rarely).
Macroscopic Exam:
Microscopic Exam:
P. marneffei causes a dissimenated type of penicilliosis, particularly in AIDS patients, and can be fatal, or disseminated infections in those who have traveled to endemic areas. It is the only strain that produces a red pigment that diffuses into the agar. Some strains are toxin-producers.
Penicilliosis:
This is commonly considered a contaminant, but can be a causative agent of keratomycosis, penicilliosis, otomycosis, onychomycosis, respiratory, urinary tract infections, endocarditis, and deep infections (rarely).
Macroscopic Exam:
- They are known for production of velvety, rugose blue-green colonies with narrow white borders on PDA and SAB agars.
Microscopic Exam:
- Microscopically, they are on septate hyphae with foot cells, bearing metulae resembling bones of "skeleton hands" or "brushes" or "witch's brooms".
- The Latin term "penicillus" means "paintbrush".
P. marneffei causes a dissimenated type of penicilliosis, particularly in AIDS patients, and can be fatal, or disseminated infections in those who have traveled to endemic areas. It is the only strain that produces a red pigment that diffuses into the agar. Some strains are toxin-producers.
Penicilliosis:
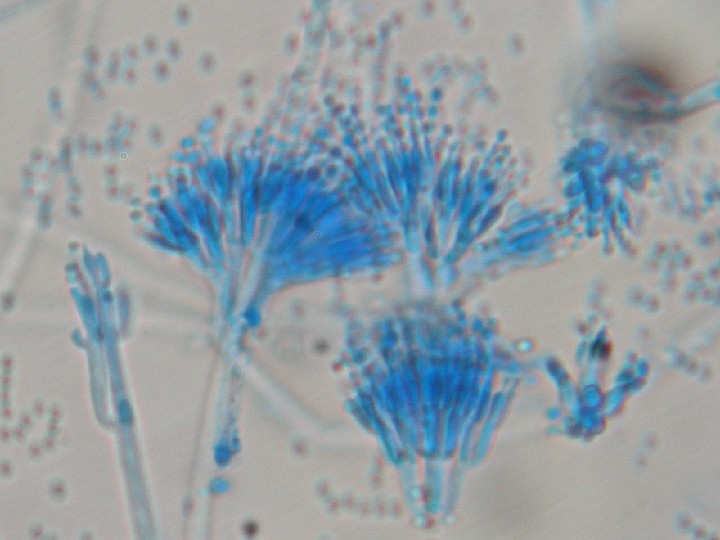
Colonies mature on SABHI agar within 4 days, with a very powdery, white and bluish-green surface with a white border. The reverse is typically white, but can also be red or brown. P. marneffei produces a red reverse and diffuses pigment into the agar and exhibits thermal dimorphism.By Carlos de Paz from A Coruña, España - Penicillium, CC BY-SA 2.0, https://commons.wikimedia.org/w/index.php?curid=24260551
|

Characteristic "penicillus"/"brush" appearance of Penicillium spp.By CDC/Dr. Lucille K. Georg [Public domain], via Wikimedia Commons
|
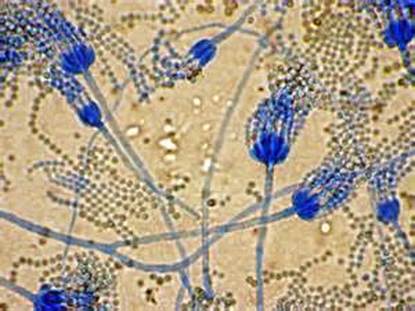
Septate hyphae with conidiophores that may or may not be branched, and secondary branches called metulae characterize Penicillium spp. On the metulae lie flask-shaped phialides arranged in whirls that bear chains of round conidia (unbranched, single chains that are smooth or rough in texture).
|
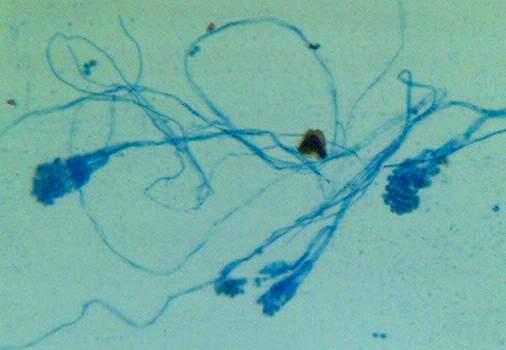
By Microrao (Own work) [Public domain], via Wikimedia Commons
|
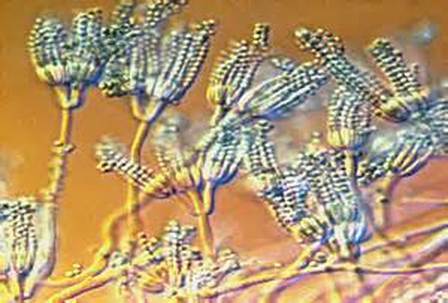
|
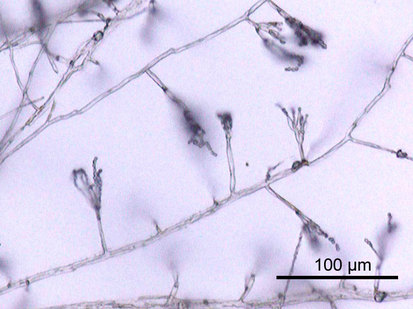
By Y_tambe (Y_tambe's file) [GFDL (http://www.gnu.org/copyleft/fdl.html), CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/) or CC BY-SA 2.5-2.0-1.0 (https://creativecommons.org/licenses/by-sa/2.5-2.0-1.0)], via Wikimedia Commons
|
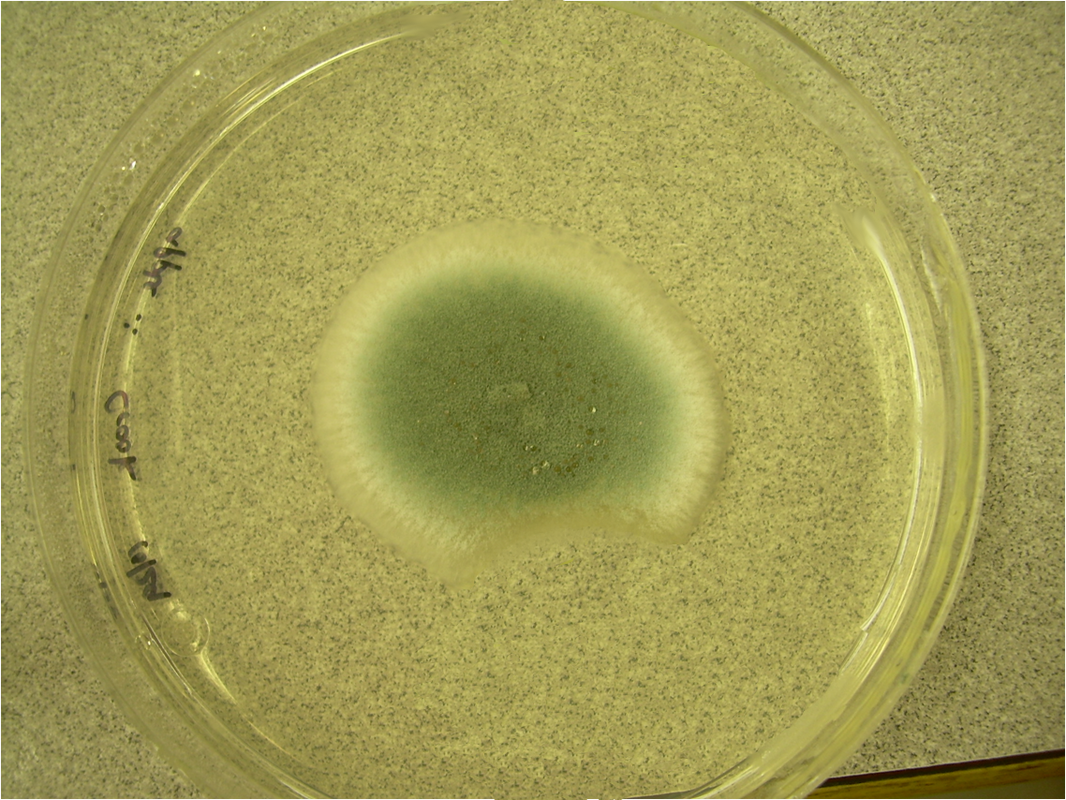
Penicillium digitatum;By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6694313
|
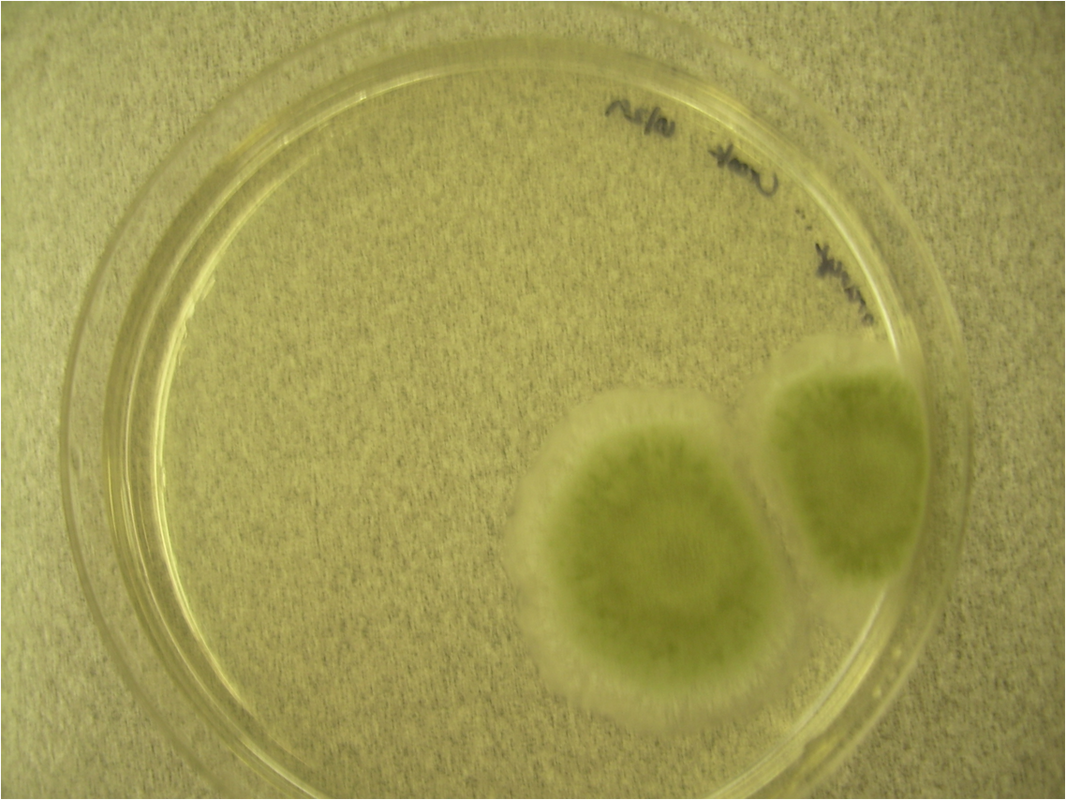
Penicillium expansum;By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6771479
|
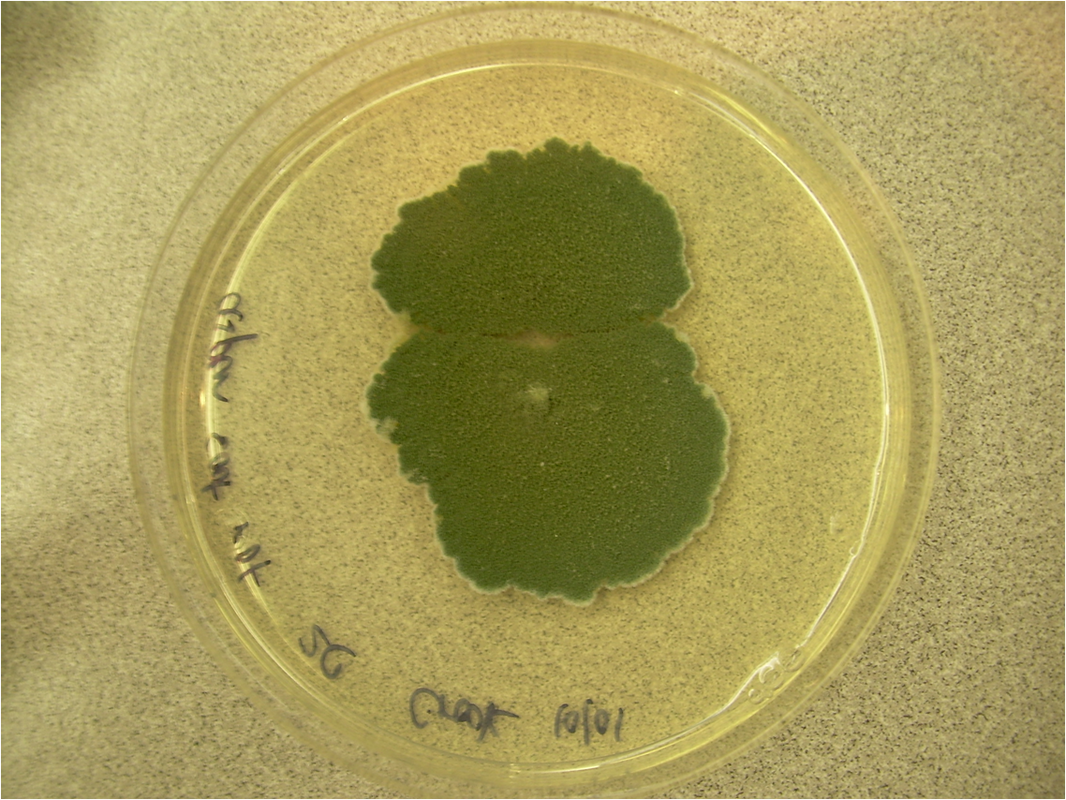
By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6694264
|
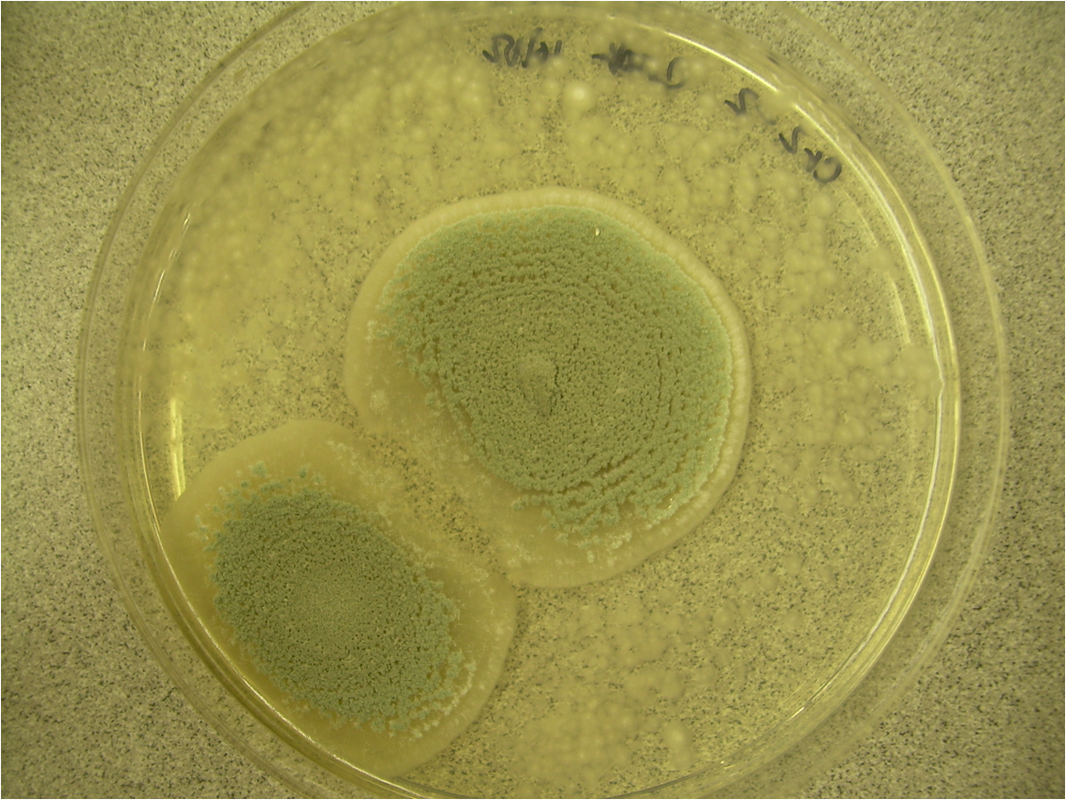
By Ninjatacoshell - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6694303
|

Penicillium notatum;By Crulina 98 - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=8406610
|
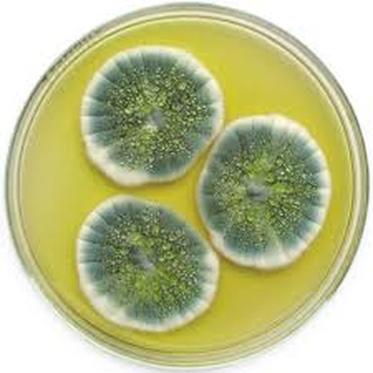
Penicillium notatum
|
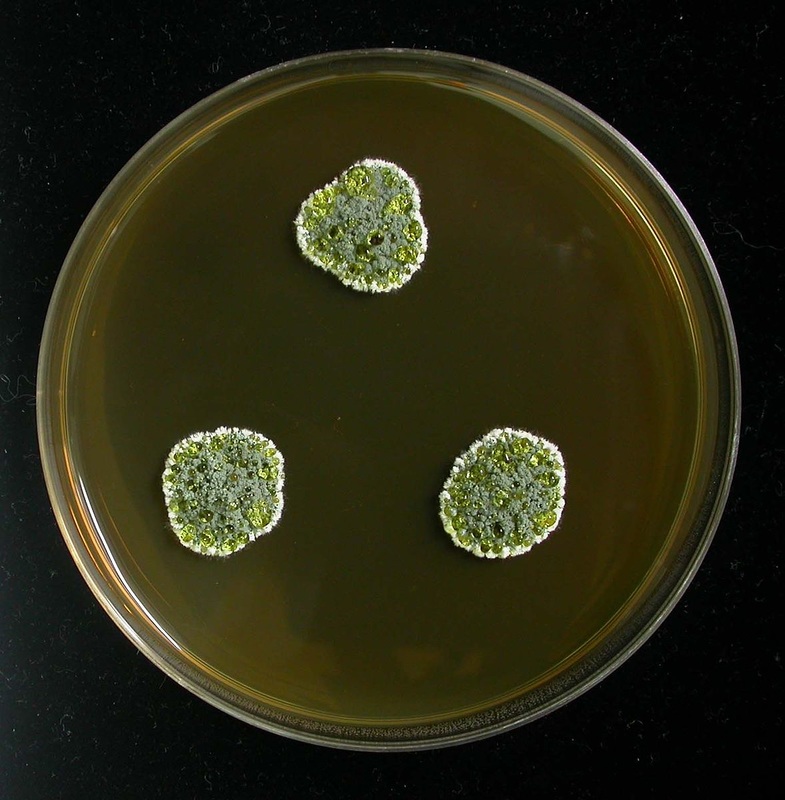
Penicillium glandicola;By sagar (yvsagar2003) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
|
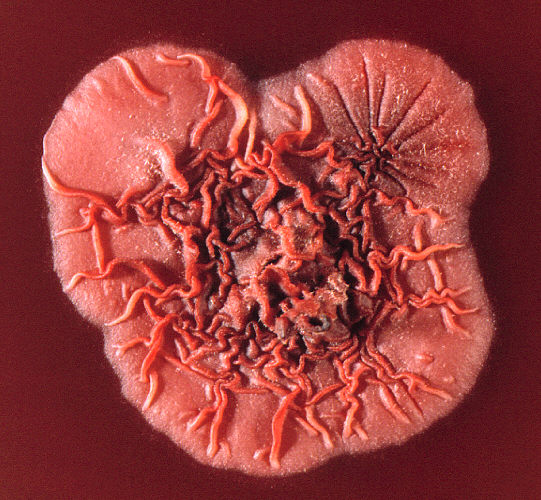
Penicillium marneffei;By James Gathany - Centers for Disease Control and Prevention, Public Domain, https://commons.wikimedia.org/w/index.php?curid=17358246
|

Image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
|
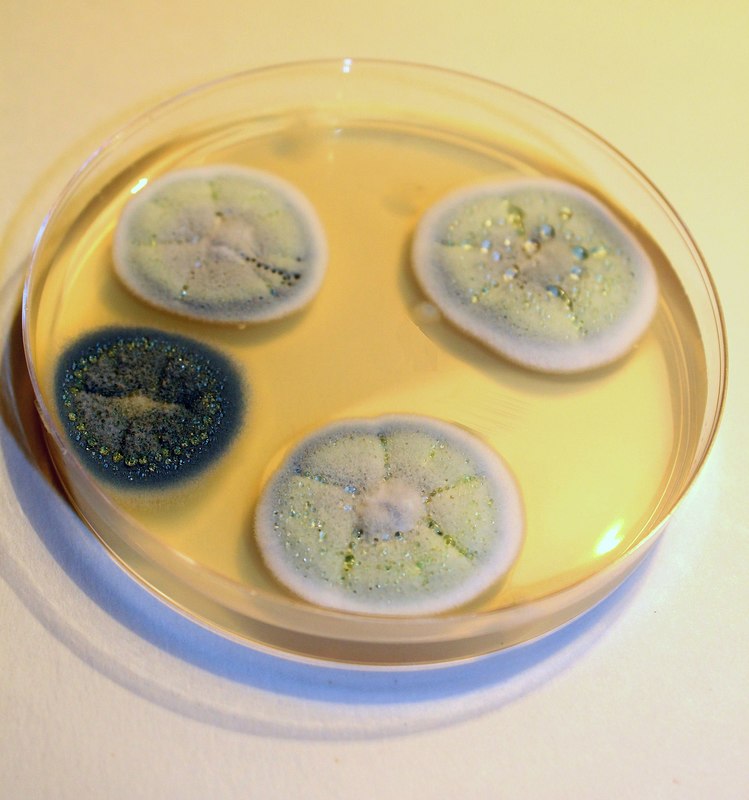
Penicillium commune and P. chrystogenum;By Convallaria majalis - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=64184244
|

Image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work

Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist at a hospital laboratory
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist at a hospital laboratory
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist
Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology, Microbiologist
the microscopic images below of penicillium spp were taken by jeanette reynolds, ms-biology, mls-amt, m-ascp:
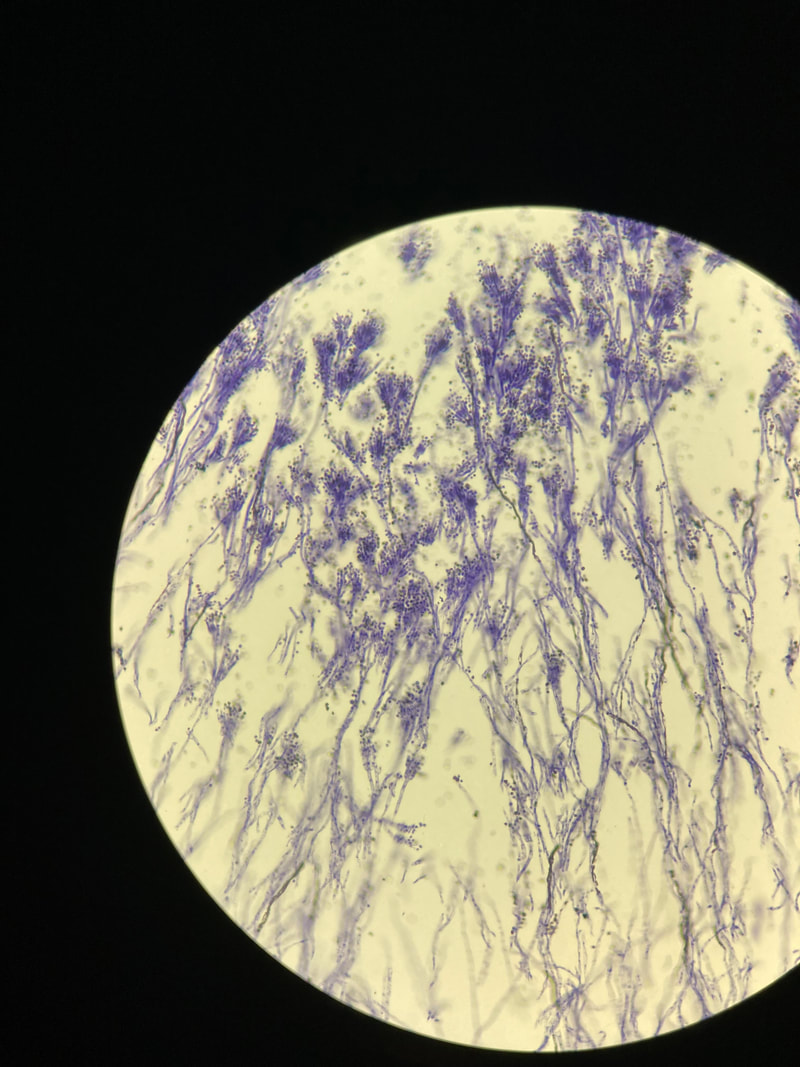
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
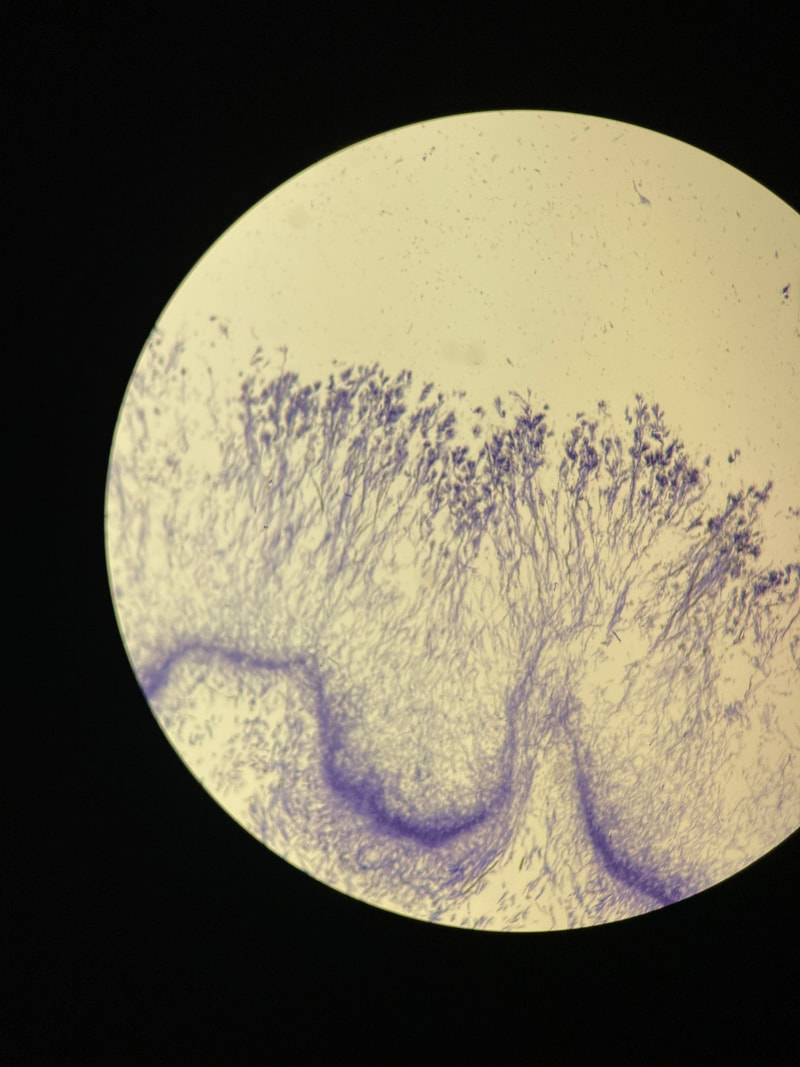
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
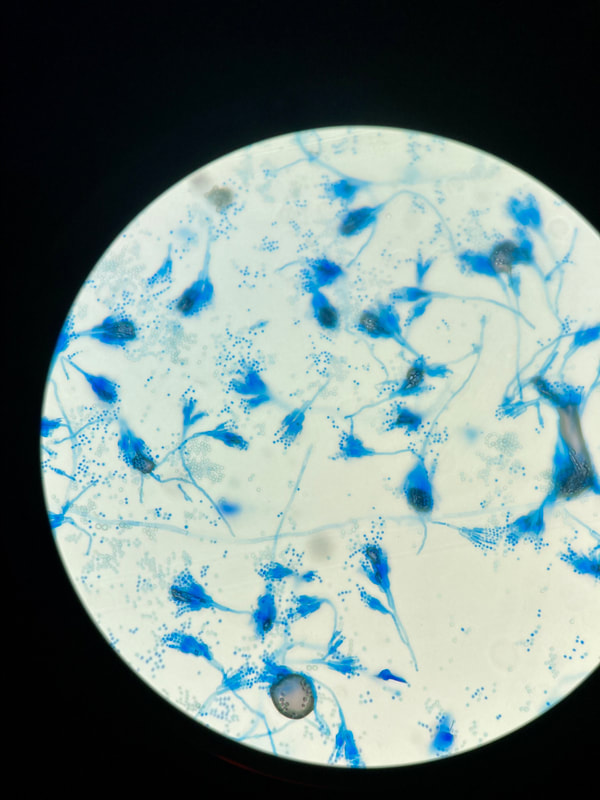
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
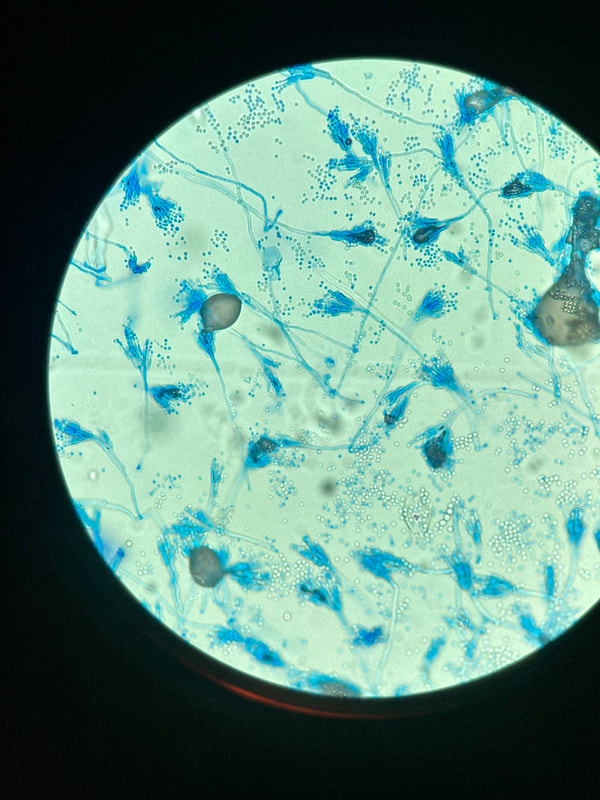
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
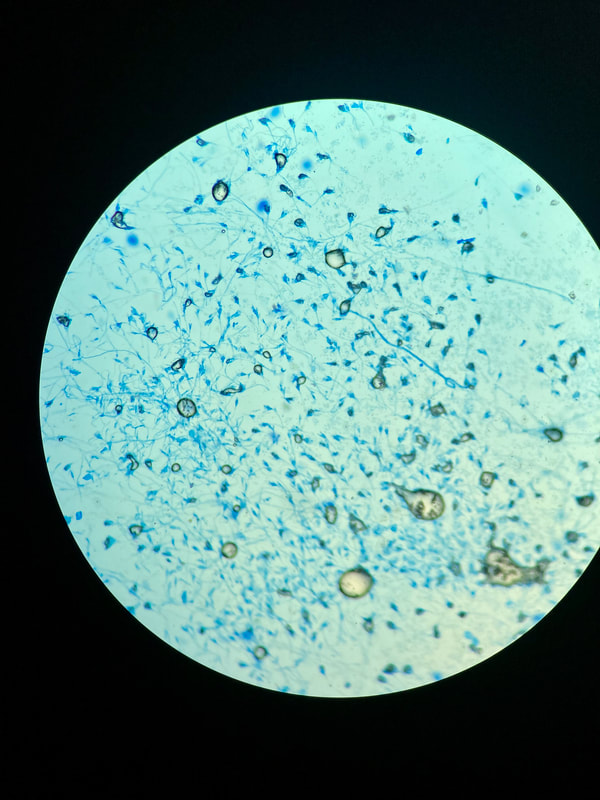
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|

Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
Scopulariopsis spp:
Most of the time, this is considered to be a contaminant. It can, however, be a causative agent of keratomycosis, occasional bronchopulmonary disease (penicilliosis), otomycosis, onychomycosis, inguinal ulcer, or skin lesion infections in immunocompromised patients.
Macroscopic Exam:
Microscopic Exam:
Most of the time, this is considered to be a contaminant. It can, however, be a causative agent of keratomycosis, occasional bronchopulmonary disease (penicilliosis), otomycosis, onychomycosis, inguinal ulcer, or skin lesion infections in immunocompromised patients.
Macroscopic Exam:
- On SABHI agar at room temperature, this is a rapid-grower, producing oclonies that are velvety, rugose, and white, becoming light tan or brown with age.
- It produces a tan reverse.
Microscopic Exam:
- Septate mycelium
- Single, unbranching or penicillus-style annellophores (stalks) bear flask-shaped or bowling pin-shaped annellides.
- Annellides support large lemon-shaped, rough annelloconidia in chains (echinulate, or spiny).
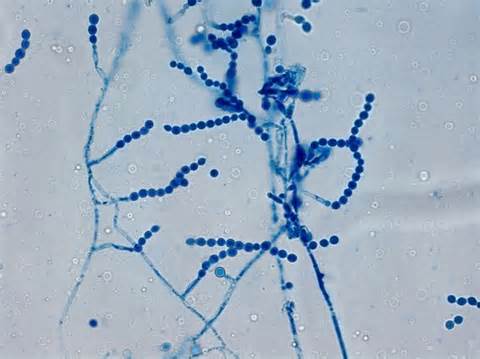
On SABHI agar at room temperature, at first, the surface appears white and glabrous in topography, changing to a powdery texture that is light brown characterized by a light tan periphery. The reverse is a brown center surrounded by tan. Hyphae are septate.
|
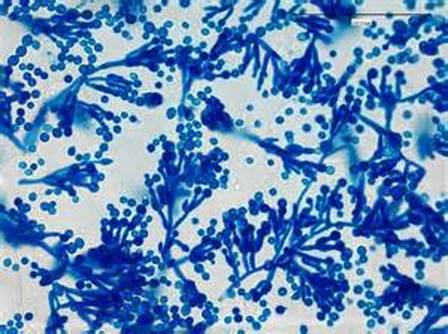
Conidiophores seen here are short and simple, with annellides bearing conidia that are large and thick-walled, round-to-lemon shaped structures that cut off at the base to form a short neck. As they mature, conidia become "spiky", "spiny" and rough.
|

|
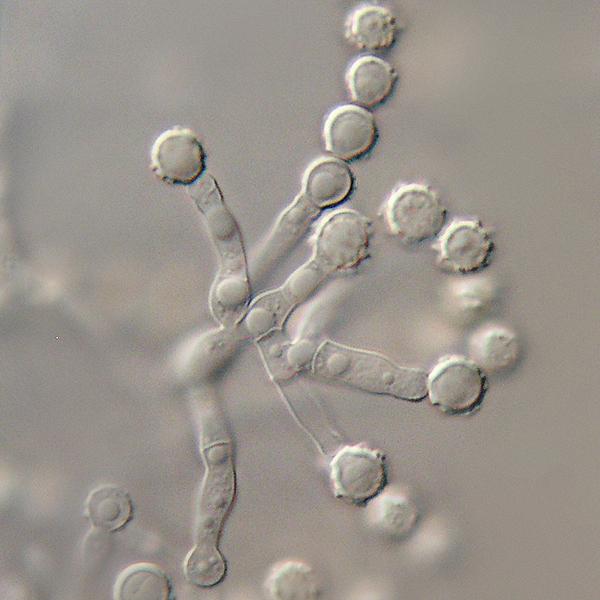
|
Sepedonium spp:
Not known to be a human pathogen. It is a common contaminant.
Macroscopic Exam:
Microscopic Exam:
Not known to be a human pathogen. It is a common contaminant.
Macroscopic Exam:
- On SABHI at room temperature, it produces waxy and white colonies that quickly turn velvety and lemon-colored with a peripheral fringe.
- White reverse
Microscopic Exam:
- Single or clusters of thick-walled, smooth or rough macroconidia at the ends of simple or branched conidiophores
- Not dimorphic

This species quickly matures within 1 week with colonies that are waxy and white, transforming into fluffy, mature, yellow colonies at 25 degrees Celsius. The reverse is simply white. Septate hyphae bear simple or branched conidiophores with large, thick-walled, spherical, rough and "knob-like" conidia.
|
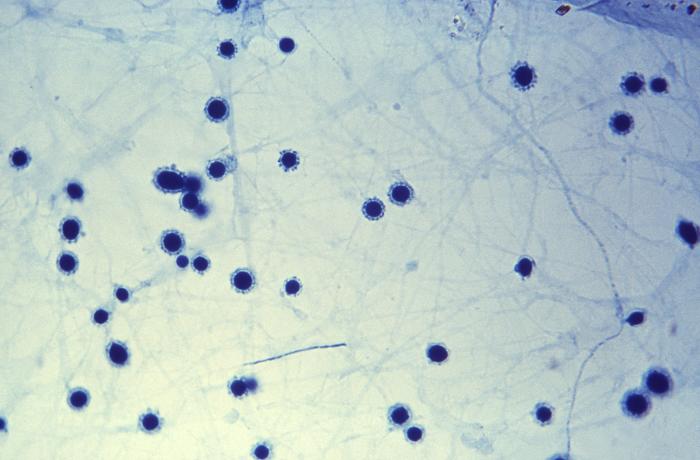
|
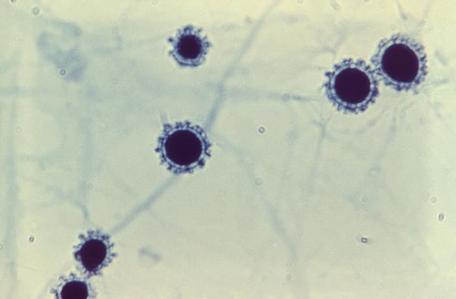
|
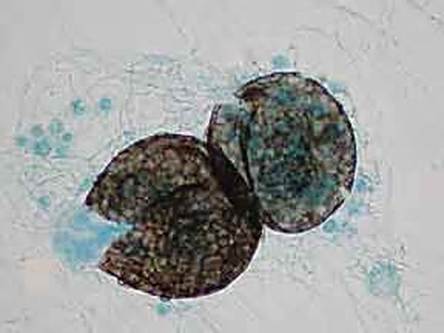
|
Keratomycosis: Eye infection (Also called mucormycosis, phyomycosis, zygomycosis if it affects the eye(s))
Otomycosis: Outer ear infection
Sinusitis: Sinus infection
Onychomycosis: Nail infection
Otomycosis: Outer ear infection
Sinusitis: Sinus infection
Onychomycosis: Nail infection

Periorbital mucormycosis (fungal eye infection caused by the mould Rhizopus mucor spp mucor)

Zygomycotic eye infection and rhinocerebral infection that has spread to infect the eye muscles and is affecting eye motion/movement
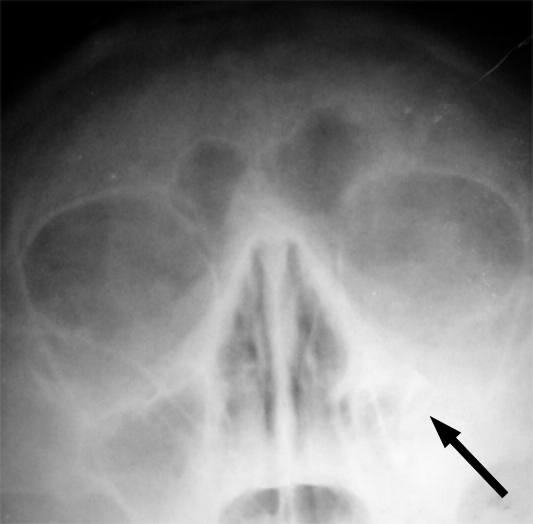
We have a variety of sinuses in our facial structure, and the maxillary sinus is one of them. Here is an example of left-sided maxillary sinusitis, which may be caused by fungi or an allergic reaction to a fungus or mould.
|

Aspergillus-caused otomycosis, outer ear infection (chronic)

Onychomycosis is a fungal nail infection
|
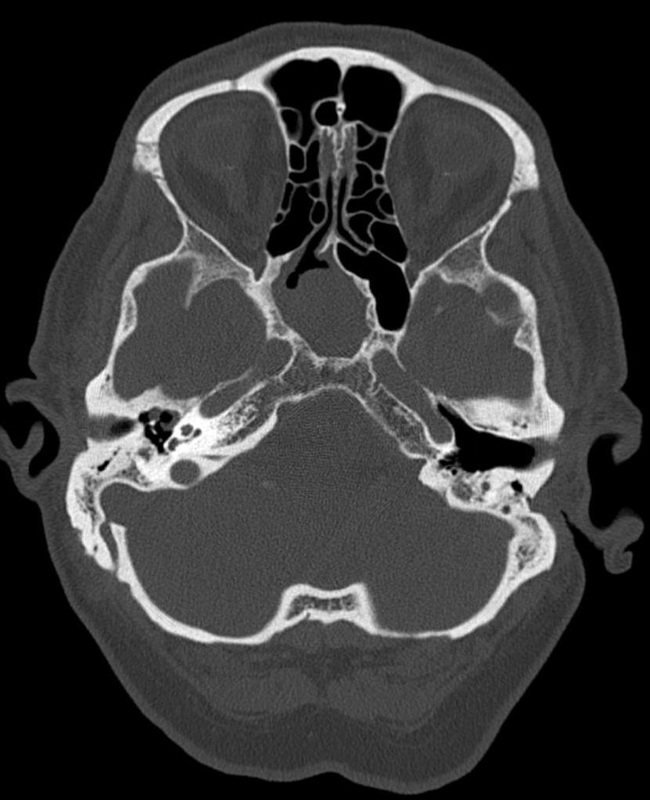
Sphenoidal sinusitis (middle, left)
superficial fungi:
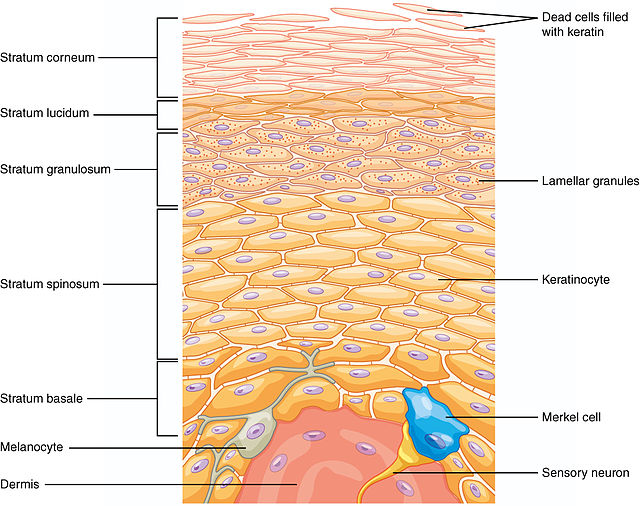
The epidermis is the superficial layer of skin, consisting of these sublayers; https://upload.wikimedia.org/wikipedia/commons/thumb/f/f9/502_Layers_of_epidermis.jpg/640px-502_Layers_of_epidermis.jpg
Superficial mycoses: These fungi only infect or colonize the outer layer of the skin
Cutaneous mycoses: These fungi infect multiple layers of the skin
Dermatomycoses: These fungi infect the dermal layer of the skin
Tinea: Discolorations (keratinized layer of skin)
Dermatophytosis: These fungi penetrate the deeper levels of the dermis and below
SUPERFICIAL ORGANISMS: Remember the acronym (PMET): Piedraia hortai, Malassezia furfur, Exophiala werneckii, Trichosporon beigleii
Exophiala (Hortaea) spp:
This organism is the causative agent of tinea nigra (brown-to-black, nonscaling patches that form mainly on the palms of the hands and grow larger over a period of months to years), and can also cause mycetoma, brain infections, eye infections, cutaneous and subcutaneous tissue infections. The infections resemble birthmarks, cafe' au lait spots, or large age spots. The organism primarily affects the palms of the hands and patches grow larger with time if left untreated. Most cases in the USA occur in the southeastern USA. Daily treatment with a topical antifungal causes the patches to disappear in approximately 2-4 weeks.
Macroscopic Exam:
Microscopic Exam:
Cutaneous mycoses: These fungi infect multiple layers of the skin
Dermatomycoses: These fungi infect the dermal layer of the skin
Tinea: Discolorations (keratinized layer of skin)
Dermatophytosis: These fungi penetrate the deeper levels of the dermis and below
SUPERFICIAL ORGANISMS: Remember the acronym (PMET): Piedraia hortai, Malassezia furfur, Exophiala werneckii, Trichosporon beigleii
Exophiala (Hortaea) spp:
This organism is the causative agent of tinea nigra (brown-to-black, nonscaling patches that form mainly on the palms of the hands and grow larger over a period of months to years), and can also cause mycetoma, brain infections, eye infections, cutaneous and subcutaneous tissue infections. The infections resemble birthmarks, cafe' au lait spots, or large age spots. The organism primarily affects the palms of the hands and patches grow larger with time if left untreated. Most cases in the USA occur in the southeastern USA. Daily treatment with a topical antifungal causes the patches to disappear in approximately 2-4 weeks.
Macroscopic Exam:
- On SABHI agar at room temperature, this organism produces a black, yeast-like colony and it is a slow-grower.
- Later, the yeast-like colony becomes covered with short, olive-gray mycelium.
- The reverse is dark.
Microscopic Exam:
- The yeast-like colony produces dark, 1 or 2-celled blastoconidia.
- The more mature mold-like colonies covered with mycelium produce hyphae with 1 or 2- celled dark blastoconidia in big clusters.
- The very old colonies produce annellides bearing clusters or chains of 1 or 2-celled dark annelloconidia.

https://upload.wikimedia.org/wikipedia/commons/thumb/4/4d/Tinea_nigra.jpg/640px-Tinea_nigra.jpg

Exophiala dermatiditis (Wangiella dermatiditis) is a slow-grower that takes up to 3 weeks to mature. After about 10 days, growth begins as "yeast-like". Colonies are shiny, moist, black, and "yeast-like" but after about 3-4 weeks, they develop aerial hyphae that appear as olive-gray in color at the periphery and near the center with a dark reverse. As seen above, dark oval, budding, yeast-like cells may be observed on dark, septate hyphae with vase-shaped or cylindrical phialides bearing round and/or oval conidia at the tips and on the sides of the conidiophores.
|
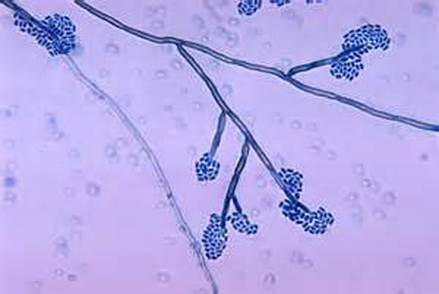
Exophiala jeanselmei (now classified as Hortaea werneckii) is a slow-grower that takes 14 days to mature at 25-30 degrees Celsius and may not even grow at all at 37 degrees Celsius. Colonies start out as brownish-black or green-black and smooth, later developing grayish hyphae that appear velvety and short like velour. The reverse is black. At first, young growth appears microscopically as yeast-like budding cells. With maturity, septation forms with many slim, tube-like, branched and unbranched annellides that come to a point at their ends. Oval-shaped conidia in clusters form at the tip and on the sides of the conidiophores and in areas along the hyphae. This species grows well on cornmeal agar or potato dextrose agar.
|

Hortaea werneckii;By CDC/Dr. Lucille K. Georg - Public Health Image Library (PHIL) -- image #3935, Public Domain, https://commons.wikimedia.org/w/index.php?curid=61753490
|
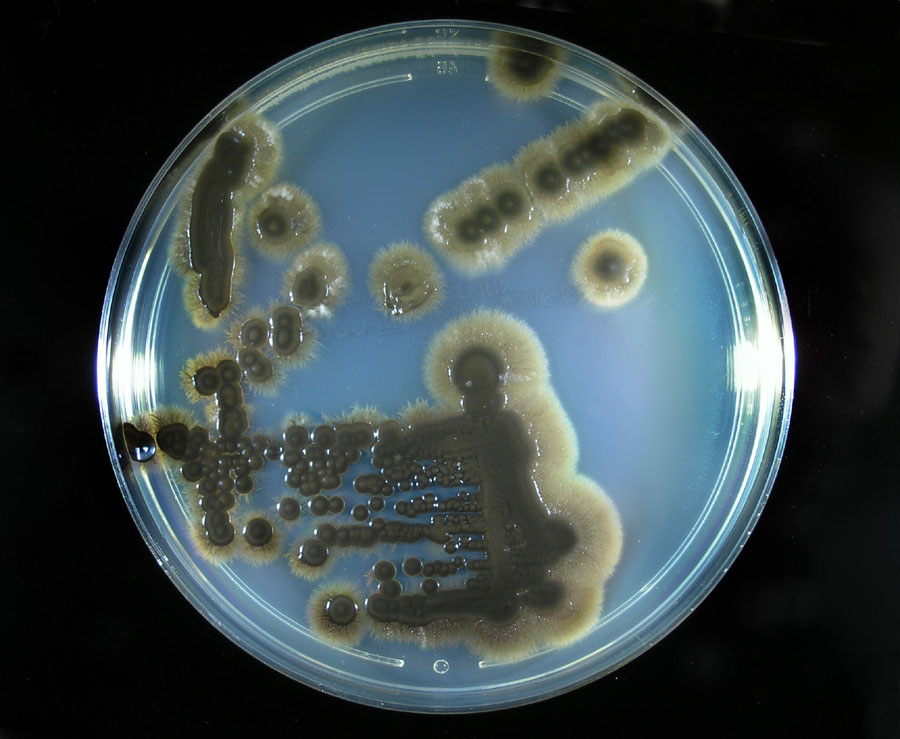
|

|
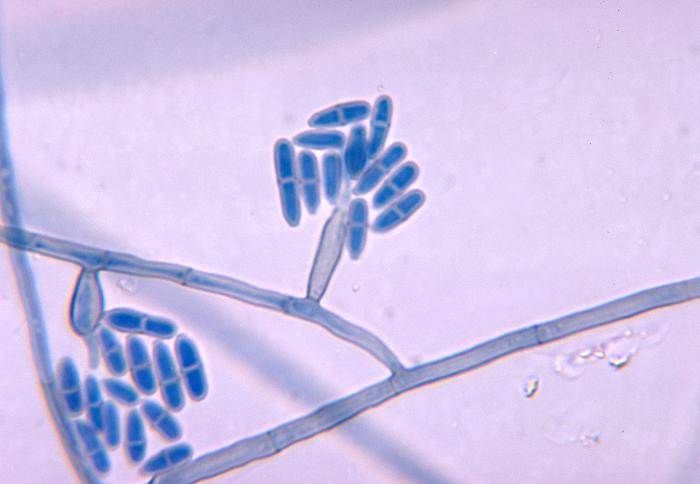
|
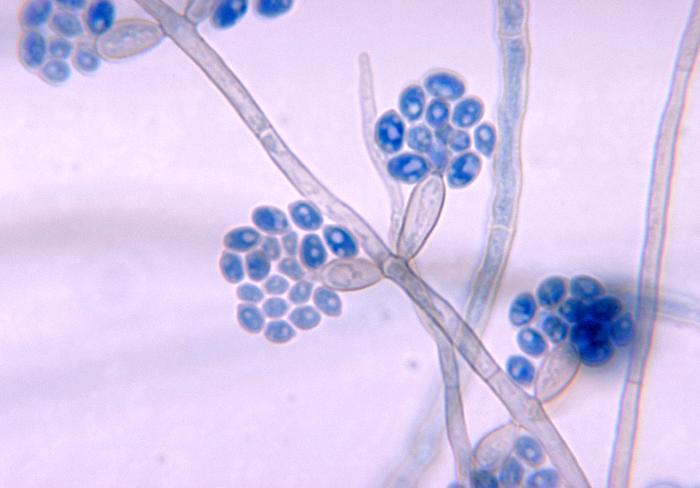
|

|
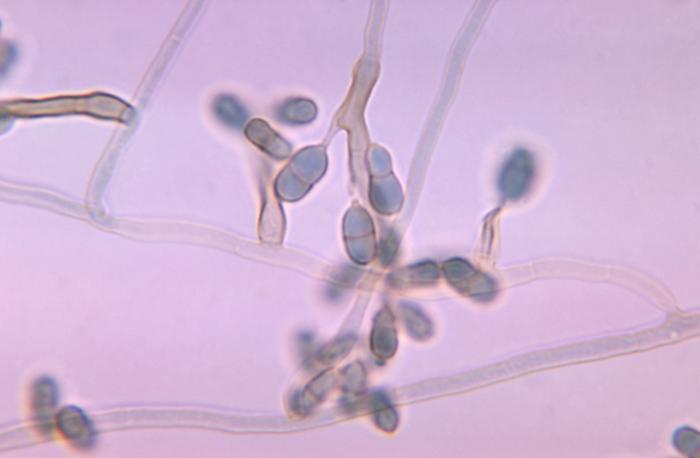
|

|
Exophiala xenobiotica, image by Jeanette Reynolds, MS-Biology, M-ASCP (cm), MT-AMT, certified instructor, certified in emerging diseases, MLS II, Microbiology Lab/Mycology/AFB
|
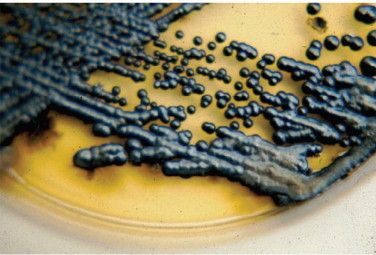
|
Malassezia furfur:
Causative agent of pityriasis versicolor (tinea versicolor), an asymptomatic, superfical skin infection that is characterized by scaly patches ranging in color from pale to red to reddish-brown, brown, and the patches fluoresce under Wood's lamp. With a sterile olive oil overlay, this organism thrives and will grow even better.
It is occasionally linked to sinusitis, folliculitis, blocked tear ducts and intravenous line sepsis, particularly in neonates and adults who are receiving nutritional therapy in the form of intravenous lipids. This organism may also produce pneumonia in these patients. Immunocompromised or immunosuppressed patients are also at risk for developing peritonitis, septic arthritis, mastitis, sinusitis from this organism. In healthy adults, this organism typically causes no problems and is, in fact, a part of the normal commensal skin flora in >90% of the adult population.
The organism thrives in warm, humid, moist environments and patients are prone to opportunistic infection if they become overheated, such as if being in a sauna for an extended period of time, exercise, hot weather, or if the patient lives in a hot, humid environment. The fungus is thought to thrive on the oils that live on the skin, lipids, and dead skin cells.
Macroscopic Exam:
Microscopic Exam:
Treatment consists of administration of 2.5% selenium sulfide in a topical application medication, which can be found in Selson Blue shampoo. Because recurrence is common in patients who are prone to this infection, a good idea is to periodically treat the skin with a natural antifungal agent, such as tea tree oil, or selenium sulfide, which can also be applied as a shampoo left on the skin for 10 minutes and then rinsed off daily for 2 weeks. Pyrathidadine zinc is also effective. If these treatments fail to clear the fungus, then a cream formulation of clotrimazole, miconazole, or ketoconazole can be used. If infection is systemic, ketoconazole is usually effective, but it can be combined or substituted with Amp B. It is resistant to flucytosine.
Causative agent of pityriasis versicolor (tinea versicolor), an asymptomatic, superfical skin infection that is characterized by scaly patches ranging in color from pale to red to reddish-brown, brown, and the patches fluoresce under Wood's lamp. With a sterile olive oil overlay, this organism thrives and will grow even better.
It is occasionally linked to sinusitis, folliculitis, blocked tear ducts and intravenous line sepsis, particularly in neonates and adults who are receiving nutritional therapy in the form of intravenous lipids. This organism may also produce pneumonia in these patients. Immunocompromised or immunosuppressed patients are also at risk for developing peritonitis, septic arthritis, mastitis, sinusitis from this organism. In healthy adults, this organism typically causes no problems and is, in fact, a part of the normal commensal skin flora in >90% of the adult population.
The organism thrives in warm, humid, moist environments and patients are prone to opportunistic infection if they become overheated, such as if being in a sauna for an extended period of time, exercise, hot weather, or if the patient lives in a hot, humid environment. The fungus is thought to thrive on the oils that live on the skin, lipids, and dead skin cells.
Macroscopic Exam:
- Smooth, cream-colored-to-yellowish-brown colonies produced by M. furfur mature quickly in about 5 days at 30-37 degrees Celsius, and rarely grow, if at all, at 25 degrees Celsius.
- Later, with maturity, colonies dry out and become more lackluster and slightly wrinkled.
- Because the organism needs long-chain fatty acids in order to thrive, overlaying your media with a thin layer of olive oil, oleic acid or Tween 80 will provide the organism with the nutrition it needs to grow.
- The best way to recover the fungus from patients is to collect blood cultures taken through the lipid infusion catheter in order to insure recovery of the organism.
- Isolator tubes are also a good way to recover the organism from patients.
- KOH wet prep is also a good way to identify the organism, as is fluoresence of the skin patches under Wood's lamp.
Microscopic Exam:
- Under the microscope, stained slides or those treated with KOH from skin disease with this organism will appear as "spaghetti and meatballs" in structure.
- In patients who have sepsis, the fungus can rarely be observed on smears of peripheral blood.
- When cultured, budding yeast cells are observed, which can be stained with calcofluor white stain.
Treatment consists of administration of 2.5% selenium sulfide in a topical application medication, which can be found in Selson Blue shampoo. Because recurrence is common in patients who are prone to this infection, a good idea is to periodically treat the skin with a natural antifungal agent, such as tea tree oil, or selenium sulfide, which can also be applied as a shampoo left on the skin for 10 minutes and then rinsed off daily for 2 weeks. Pyrathidadine zinc is also effective. If these treatments fail to clear the fungus, then a cream formulation of clotrimazole, miconazole, or ketoconazole can be used. If infection is systemic, ketoconazole is usually effective, but it can be combined or substituted with Amp B. It is resistant to flucytosine.
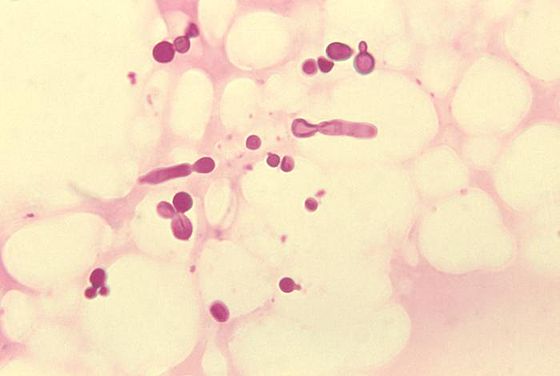
M. furfur resembles "spaghetti and meatballs". Yeast-like cells are also seen, which are actually phialides with small collarettes, which are difficult to see with routine microscopy.By http://phil.cdc.gov/phil_images/20030610/22/PHIL_3938_lores.jpg, Public Domain, https://commons.wikimedia.org/w/index.php?curid=763104

Malessezia furfur-caused tinea versicolor, fluorescing under Wood's lamp (UV)
|

Tinea versicolor
|

Tinea versicolor with folliculitis; https://upload.wikimedia.org/wikipedia/commons/thumb/3/3d/Pityriasis_versicolor_frontal_retouche.jpg/640px-Pityriasis_versicolor_frontal_retouche.jpg

https://upload.wikimedia.org/wikipedia/commons/thumb/d/dd/Pytriasis_amanticae_new_image.jpg/640px-Pytriasis_amanticae_new_image.jpg
|

https://upload.wikimedia.org/wikipedia/commons/thumb/7/79/Tinea.jpg/640px-Tinea.jpg
|
Piedraia hortaii
This organism is the causative agent of black piedra, a condition which consists of firmly attached hard, black nodules surrounding the outside of the scalp hairs (ectothrix). This type of infection is typically seen in tropical climates. The only way to treat it is to shave all the hairs in the infected area.
Macroscopic Exam:
Microscopic Exam:
This organism is the causative agent of black piedra, a condition which consists of firmly attached hard, black nodules surrounding the outside of the scalp hairs (ectothrix). This type of infection is typically seen in tropical climates. The only way to treat it is to shave all the hairs in the infected area.
Macroscopic Exam:
- On SABHI agar at room temperature, this organism forms a small, green-black, heaped, glabrous colony. It is a slow-grower.
Microscopic Exam:
- Under the microscope, dark, thick-walled hyphae will be seen with swellings.
- Asci containing ascospores may be observed.

This fungus is a slow-grower that matures in 21 days. THe colonies are small, sticky, slightly raised, and range in color from dark brown to black. Their topography is either glabrous or velvety. Some strains produces a reddish-brown pigment that diffuses into the agar. The reverse is black. Microscopically, the organism produces septate hyphae that are dark and thick-walled. The hyphae bear quite a few intercalary chlamydoconidium-like cells.
|
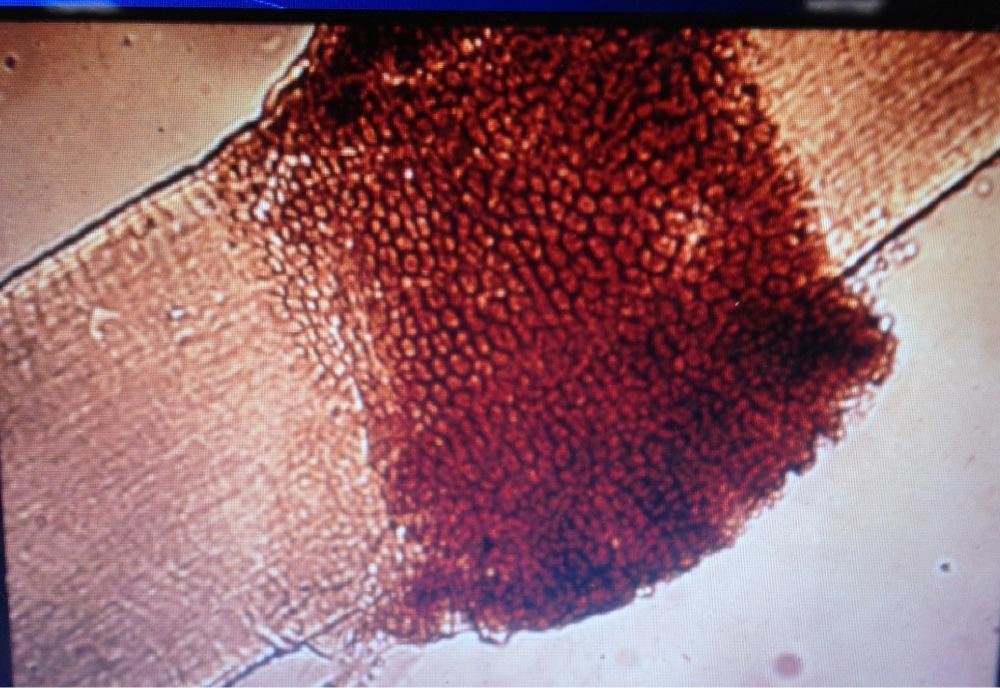
Ectothrix is seen on a hair shaft, where the spores are growing on the outside of the hair shaft
|
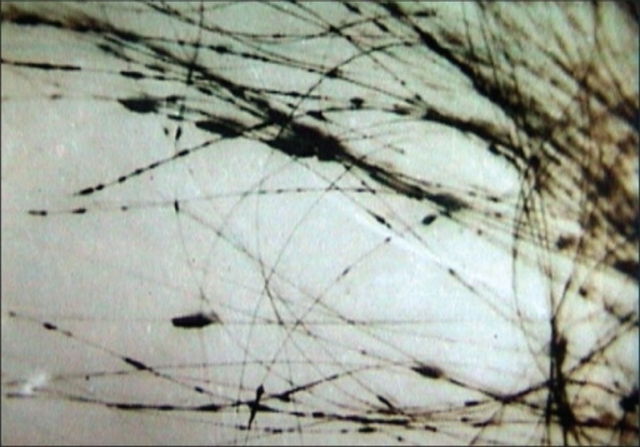
https://upload.wikimedia.org/wikipedia/commons/thumb/a/ad/Piedra_Negra_Micosis.png/640px-Piedra_Negra_Micosis.png
Trichosporon beigelii:
This organism is the causative agent of white piedra, a condition consisting of light brown, soft nodules around the hairs of the beard and mustache, which are loosely attached. It resembles nits, or lice eggs, which stick to the hairs. It causes classic, chronic dandruff. Invasive disease can occur, however, and disseminate in immunocompromised patients, affecting the blood, kidneys, lungs, and skin, with production of fever, pulmonary infiltrates, and cutaneous lesions.
Macroscopic Exam:
Microscopic Exam:
Treatment consists of cutting or shaving all the hairs in the infected area, followed by applying topical clotrimazole cream or Amp B lotion. If it is disseminated, it is resistant to Amp B and can cause serious infection.
This organism is the causative agent of white piedra, a condition consisting of light brown, soft nodules around the hairs of the beard and mustache, which are loosely attached. It resembles nits, or lice eggs, which stick to the hairs. It causes classic, chronic dandruff. Invasive disease can occur, however, and disseminate in immunocompromised patients, affecting the blood, kidneys, lungs, and skin, with production of fever, pulmonary infiltrates, and cutaneous lesions.
Macroscopic Exam:
- On SABHI agar at room temperature, it will grow a cream-colored, wrinkled, glabrous colony.
- Growth occurs in approximately 5 days.
Microscopic Exam:
- If you grow this organism on cornmeal agar, you can view the cornmeal agar under the microscope, and you will observe hyaline hyphae with blastoconidia and arthroconidia.
- It can also be stained with lactophenol cotton blue stain.
Treatment consists of cutting or shaving all the hairs in the infected area, followed by applying topical clotrimazole cream or Amp B lotion. If it is disseminated, it is resistant to Amp B and can cause serious infection.

https://upload.wikimedia.org/wikipedia/commons/thumb/1/15/Piedra_Blanca_Micosis.jpg/640px-Piedra_Blanca_Micosis.jpg
|

https://upload.wikimedia.org/wikipedia/commons/thumb/7/78/Excessive_dandruff.jpg/640px-Excessive_dandruff.jpg
|

https://upload.wikimedia.org/wikipedia/commons/thumb/d/d6/Trichosporon_asteroides_culture.jpg/640px-Trichosporon_asteroides_culture.jpg

White piedra affecting a hair, consisting of light brown, soft nodules covering the outside of the hair shaft. This is referred to as "ectothrix".
|
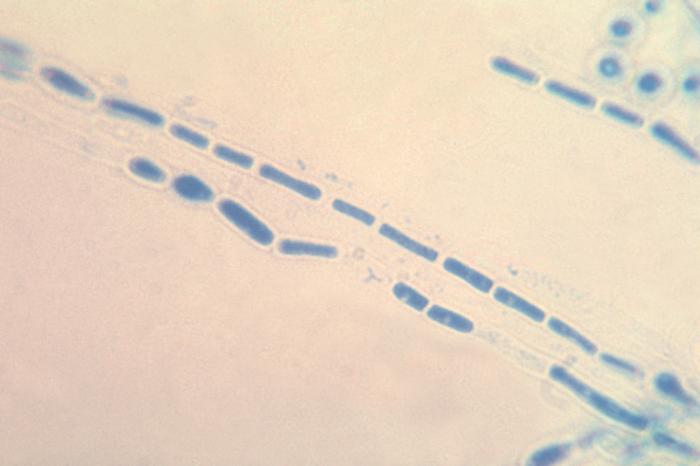
Trichosporon beigelii, a rapid-grower that matures in 5 days, produces cream-colored, yeast-like colonies that are soft and moist, which transform into finely wrinkled colonies with heaped, darkened centers. Microscopically, true hyphae and pseudohyphae may be seen with single or short-chained blastoconidia. Arthroconidia form on cultures that are older.
|
dermatophytes and zygomycosis:
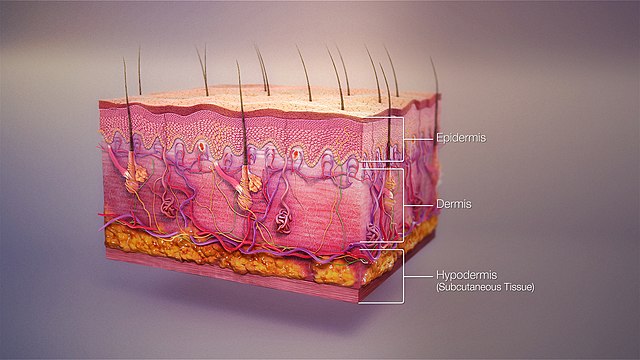
https://upload.wikimedia.org/wikipedia/commons/thumb/f/f0/3D_medical_animation_skin_layers.jpg/640px-3D_medical_animation_skin_layers.jpg
Dermatophytes: (Remember the acronym MET)
1) Microsporum: Infects skin and ectothrix hair
2) Epidermophyton: Infects skin, nails, and ectothrix hair
3) Trichophyton: Infects skin, nails, and endothrix hair
The dermatophytes are characterized by their ability to invade the skin, hair and nails, digesting and gaining nutrients from the protein keratin. These fungi typically colonize the outermost layer of the skin, nails or hair (because they are keratinized). The result is illness, displaying as ringworm or tinea, which is actually a result of the host's immune reaction to the release of fungal enzymes during the invasion and digestive process. These, in essence, are a "parasitic" type of fungi, dependent upon the host for nutrients and for survival.
Endothrix Invasion: Invades the inside of the hair shaft (penetrates the hair shaft)
Ectothrix Invasion: Invades only the outside of the hair shaft
Dermatophyte Test Medium:
Hair Fluorescence: Fluorescence under Wood's Lamp (UV):
Dermatophytoses:
1) Tinea capitis: scalp (Microsporum spp, Trichophyton spp, rarely Exophiala werneckii)
2) Tinea corporis: body (M. audouinii, M. canis, M. gypseum, T. mentagrophytes, T. rubrum, T. verrucosum, T. violaceum, T. tonsurans, T. schoenleinii)
3) Tinea barbae: beard, barber's itch (M. canis, T. mentagrophytes, T. rubrum, T. verrucosum, T. violaceum)
4) Tinea cruris: groin, jock itch (E. floccosum, T. mentagrophytes, T. rubrum, C. albicans, E. werneckii)
5) Tinea pedis: foot, athlete's foot (E. floccosum, T. mentagrophytes, T. rubrum, C. albicans, T. tonsurans, T. violaceum, E. werneckii)
6) Tinea manuum: infection of the hand
7) Onychomycosis: infection of the nailbed
8) Tinea unguium: nail, onychomycosis (E. floccosum, T. mentagrophytes, T. rubrum, C. albicans, T. tonsurans, T. violaceum, T. schoenleinii, M. canis, E. werneckii)
9) Tinea versicolor: discolorations of the skin due to fungi
10) Tinea nigra: discolored patches of the skin due to fungi
Dermatophytosis is treated by topical ointments if the infection is not widespread and does not involved the hair or nails. Imidazole, tolnaftate, terbinafine, amorolfine, or cyclopiroxolamine are ointments that are very good and treatment ranges from 7 days to 4 weeks. Oral therapy, such as itraconazole, is indicated for tinea cruris or tinea corporis (1 week), tinea pedis (2 weeks) or nail infections (1 week/month for 2-4 months). Ketoconazole is another option for long-term therapy for nail disease. Griseofulvin is often prescribed for skin diseases and some nail diseases.
Microsporum spp:
Microsporum canis: This dermatophyte is zoophilic, because it often spreads from domestic pets to family members. It is linked to scalp infections and skin ringworm, and is also more prevalent in kids than adults. It has also been linked to widespread epidemics of tinea capitis. It causes ectothrix hair infections and damages them from the outside in.
Microsporum cookei spp complex: *NOTE: This has been renamed to Paraphyton cookei spp complex
This dermatophyte is found in the soil and it is only occasionally linked to human infection.
Microsporum ferrugineum: This species mainly causes tinea capitis in kids.
Microsporum gallinae: *NOTE: This has been renamed to Lophophyton gallinae:
This dermatophyte causes tinea capitis and tinea corporis and it also affects birds and chickens.
Microsporum gypseum: *NOTE: This has been renamed to Nannizzia gypsea spp complex
This dermatophyte produces infection of the scalp and skin.
Epidermophyton floccosum:
There is just this one species of this organism. It was first isolated in 1870 by Carl Otto Harz, but it was identified again later in 1905 and 1907 by Castellani and Sabouraud, and later named in 1930. It is the 3rd most common cause of tinea pedis. It infects skin and nails as well, and is linked to jock itch, ringworm, and onychomycosis, but does not infect the hair.
Trichophyton species:
When it comes to hair fluorescence, hairs that fluoresce do so because they are infected with a fungus that produces a metabolite known as pteridine, which is a pigment, and it produces a bright green-yellow fluorescence under a Wood's Lamp (366 nm). The dermatophytes that produce fluorescence include:
The rate of growth differs for all three of these organisms, which aids in differentiating them from one another. The quickest growers need about 6-10 days to grow and include:
Slow-growers need about 11-21 days go grow, and include:
The most critical means of identification is the microscopic characteristics displayed by each type of dermatophyte. It is best to subculture these fungi to potato dextrose agar to promote conidia formation and sporulation. Fresh isolates on SABHI agar produce the following characteristics:
Differentiating tests can be used in addition to the macroscopic and microscopic exam and include the urease test. The urease test can be used to differentiate T. mentagrophytes from T. rubrum. T. mentagrophytes produces the enzyme urease, which will produce a positive urease test, turning the urease gel agar tube test from yellow to bright fuschsia in color, whereas T. rubrum does not produce the enzyme, so the test will be negative and there will be no color change.
1) Microsporum: Infects skin and ectothrix hair
2) Epidermophyton: Infects skin, nails, and ectothrix hair
3) Trichophyton: Infects skin, nails, and endothrix hair
The dermatophytes are characterized by their ability to invade the skin, hair and nails, digesting and gaining nutrients from the protein keratin. These fungi typically colonize the outermost layer of the skin, nails or hair (because they are keratinized). The result is illness, displaying as ringworm or tinea, which is actually a result of the host's immune reaction to the release of fungal enzymes during the invasion and digestive process. These, in essence, are a "parasitic" type of fungi, dependent upon the host for nutrients and for survival.
Endothrix Invasion: Invades the inside of the hair shaft (penetrates the hair shaft)
Ectothrix Invasion: Invades only the outside of the hair shaft
Dermatophyte Test Medium:
Hair Fluorescence: Fluorescence under Wood's Lamp (UV):
Dermatophytoses:
1) Tinea capitis: scalp (Microsporum spp, Trichophyton spp, rarely Exophiala werneckii)
2) Tinea corporis: body (M. audouinii, M. canis, M. gypseum, T. mentagrophytes, T. rubrum, T. verrucosum, T. violaceum, T. tonsurans, T. schoenleinii)
3) Tinea barbae: beard, barber's itch (M. canis, T. mentagrophytes, T. rubrum, T. verrucosum, T. violaceum)
4) Tinea cruris: groin, jock itch (E. floccosum, T. mentagrophytes, T. rubrum, C. albicans, E. werneckii)
5) Tinea pedis: foot, athlete's foot (E. floccosum, T. mentagrophytes, T. rubrum, C. albicans, T. tonsurans, T. violaceum, E. werneckii)
6) Tinea manuum: infection of the hand
7) Onychomycosis: infection of the nailbed
8) Tinea unguium: nail, onychomycosis (E. floccosum, T. mentagrophytes, T. rubrum, C. albicans, T. tonsurans, T. violaceum, T. schoenleinii, M. canis, E. werneckii)
9) Tinea versicolor: discolorations of the skin due to fungi
10) Tinea nigra: discolored patches of the skin due to fungi
- T. mentagrophytes: common cause of athlete's foot
- T. rubrum: THE MOST COMMON CAUSE OF ATHLETE'S FOOT
- T. tonsurans is the main cause of scalp ringworm
Dermatophytosis is treated by topical ointments if the infection is not widespread and does not involved the hair or nails. Imidazole, tolnaftate, terbinafine, amorolfine, or cyclopiroxolamine are ointments that are very good and treatment ranges from 7 days to 4 weeks. Oral therapy, such as itraconazole, is indicated for tinea cruris or tinea corporis (1 week), tinea pedis (2 weeks) or nail infections (1 week/month for 2-4 months). Ketoconazole is another option for long-term therapy for nail disease. Griseofulvin is often prescribed for skin diseases and some nail diseases.
Microsporum spp:
- Spindle-shaped macroconidia (numerous, rough, thick-walled)
- Teardrop-shaped microconidia borne along the hyphae (except M. audouinii)
Microsporum canis: This dermatophyte is zoophilic, because it often spreads from domestic pets to family members. It is linked to scalp infections and skin ringworm, and is also more prevalent in kids than adults. It has also been linked to widespread epidemics of tinea capitis. It causes ectothrix hair infections and damages them from the outside in.
Microsporum cookei spp complex: *NOTE: This has been renamed to Paraphyton cookei spp complex
This dermatophyte is found in the soil and it is only occasionally linked to human infection.
Microsporum ferrugineum: This species mainly causes tinea capitis in kids.
Microsporum gallinae: *NOTE: This has been renamed to Lophophyton gallinae:
This dermatophyte causes tinea capitis and tinea corporis and it also affects birds and chickens.
Microsporum gypseum: *NOTE: This has been renamed to Nannizzia gypsea spp complex
This dermatophyte produces infection of the scalp and skin.
Epidermophyton floccosum:
There is just this one species of this organism. It was first isolated in 1870 by Carl Otto Harz, but it was identified again later in 1905 and 1907 by Castellani and Sabouraud, and later named in 1930. It is the 3rd most common cause of tinea pedis. It infects skin and nails as well, and is linked to jock itch, ringworm, and onychomycosis, but does not infect the hair.
Trichophyton species:
- Trichophyton mentagrophytes: Infects hair and nails and is a common cause of tinea pedis and onychomycosis and rare severe infections
- Trichophyton rubrum: Infets the skin and nails and only rarely infects the hair (beard or scalp hairs) and is one of the most common causes of dermatophytosis and of onychomycosis and tinea pedis
- Trichophyton tonsurans: Infects the scalp, skin and nails and causes tinea capitis in kids, particularly in urban areas
- Trichopnyton terrestre (NOW renamed to Arthroderma terrestre spp complex): This is not known to cause infection in humans, but is found in the soil and closely resembles other Trichophyton spp
- Trichophyton megininii: Infects the beard (tinea barbae) but can also cause scalp and skin infetions
- Trichophyton soudanense: Primarily infects the scalp and hair but it can also spread to other parts of the body; Rare in the USA
- Trichophyton schoenleinii: Causes an infection known as "favus", which is severe, chronic, and a persistent and recurrent scalp infection that can lead to hair loss; It can also infect the skin and nails
- Trichophyton verrucosum: This dermatophyte is carried by animals, particularly cows; In humans, it can infect the beard, scalp, nails, or skin and rarely spread to other parts of the body
- Trichophyton violaceum: This dermatophyte penetrates the hairs, causing endothrix infection, but can also infect the scalp, the skin and the nails, and it is one of the most common causes of tinea capitis in North Africa and in West Asia.
- Trichophyton ajelloi (NOW renamed to Arthroderma uncinatum): This dermatohpyte is a rare cause of infection in humans.
When it comes to hair fluorescence, hairs that fluoresce do so because they are infected with a fungus that produces a metabolite known as pteridine, which is a pigment, and it produces a bright green-yellow fluorescence under a Wood's Lamp (366 nm). The dermatophytes that produce fluorescence include:
- Microsporum canis
- Microsporum audouinii
- Microsporum distortum
- Microsporum ferrugineum
The rate of growth differs for all three of these organisms, which aids in differentiating them from one another. The quickest growers need about 6-10 days to grow and include:
- Epidermophyton floccosum
- Microsporum canis
- Microsporum gypseum (Now Nannizzia gypsea spp complex)
- Trichophyton mentagrophytes
Slow-growers need about 11-21 days go grow, and include:
- Microsporum audouinii
- Trichophyton rubrum
- Trichophyton schoenleinii
- Trichophyton tonsurans
- Trichophyton verrucosum
- Trichophyton violaceum
The most critical means of identification is the microscopic characteristics displayed by each type of dermatophyte. It is best to subculture these fungi to potato dextrose agar to promote conidia formation and sporulation. Fresh isolates on SABHI agar produce the following characteristics:
- Microsporum spp
- Many rough-walled, elliptical/spindle-shaped, thick or thin, 3-7-celled macroconidia
- A few club-shaped, single microconidia borne along the hyphae
- Exception: M. audouinii rarely produces either
- Epidermophyton floccosum
- May smooth-walled, club-shaped, thin-walled, 2-4-celled macroconidia
- NO microconidia are produced
- Trichophyton spp
- Rare, smooth, pencil-shaped, thin-walled, 3-8-celled macroconidia
- Numerous or a few round, oval or club-shaped microconidia borne singly or in grapelike clusters
- Exceptions: T. schoenleinii, T. violaceum do not grow macroconidia and rarely form microconidia
Differentiating tests can be used in addition to the macroscopic and microscopic exam and include the urease test. The urease test can be used to differentiate T. mentagrophytes from T. rubrum. T. mentagrophytes produces the enzyme urease, which will produce a positive urease test, turning the urease gel agar tube test from yellow to bright fuschsia in color, whereas T. rubrum does not produce the enzyme, so the test will be negative and there will be no color change.
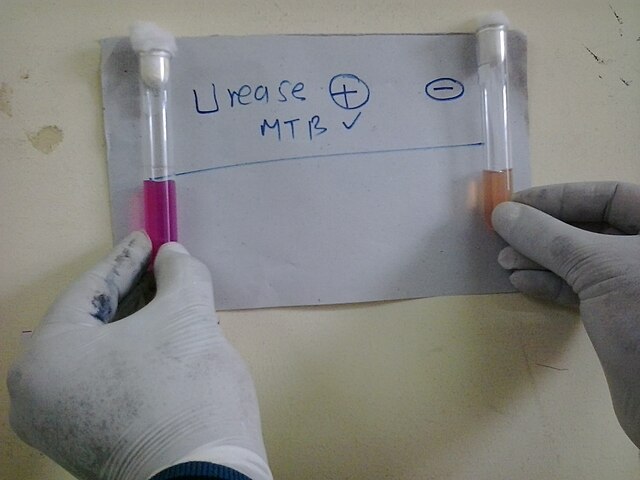
Example of a positive urease test (left) and negative urease test (right). This test is also used for some bacteria and some yeasts, so it is important to make sure that the molds are pure when subculturing them to the urease tube. https://upload.wikimedia.org/wikipedia/commons/thumb/4/4d/Urease_positive_Mycobacterium_tuberculosis.jpg/640px-Urease_positive_Mycobacterium_tuberculosis.jpg
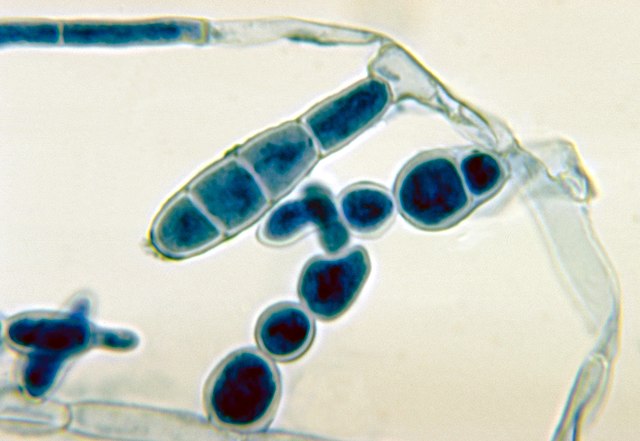
Club-shaped macroconidia with 2-4 cells of Epidermophyton floccosum are seen here. There are no microconidia. https://upload.wikimedia.org/wikipedia/commons/thumb/4/49/Epidermophyton_floccosum_01.jpg/640px-Epidermophyton_floccosum_01.jpg

Microsporum produces rough-walled, eliiptical/spindle-shaped, 3-7-celled macroconidia as seen in this image. https://upload.wikimedia.org/wikipedia/commons/thumb/5/5f/Microsporum_canis_1.JPG/640px-Microsporum_canis_1.JPG

Trichophyton spp produces smooth, pencil-shaped, 3-8-celled macroconidia and numerous blastoconidia in clusters; https://upload.wikimedia.org/wikipedia/commons/thumb/5/5c/Trichophyton_mentagrophytes_PHIL22306.png/640px-Trichophyton_mentagrophytes_PHIL22306.png
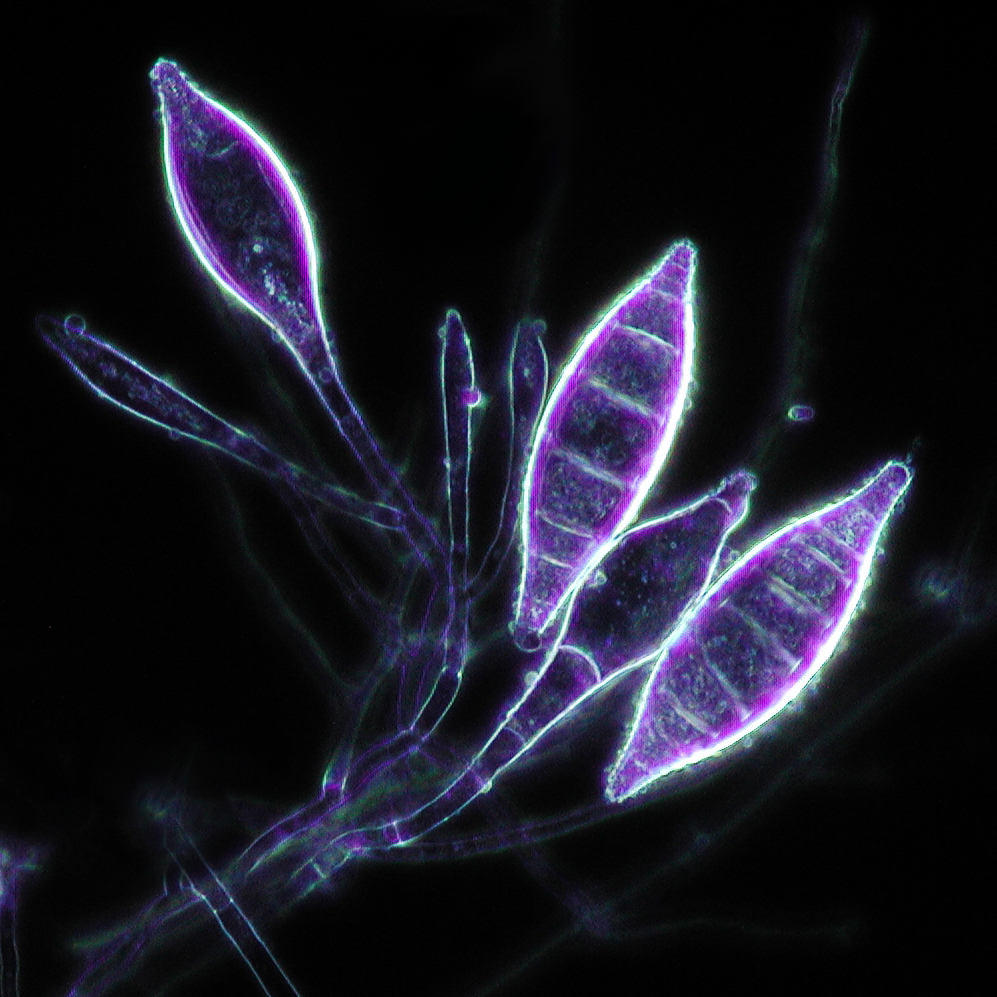
Wood's Lamp fluorescence; https://upload.wikimedia.org/wikipedia/commons/1/19/Mcanis036.JPG
Microsporum species:
- M. gypseum
- Found in the soil
- Opportunistic infections in humans: face, trunk, limbs
- Produces numerous thin-walled, rough-walled macroconidia that are elliptical-shaped (fusiform) with 4-6 cells
- Produces a few club-shaped microconidia
- Colonies are powdery and cinnamon or buff-colored with a tan reverse
- Found in the soil
- M. canis
- Found on cats and dogs
- Opportunistic infections in humans: scalp, face, trunk, limbs
- Fluorescent in Wood's Lamp
- Most infections occur in kids
- Produces numerous thick-walled, spindle-shaped macroconidia that are tapered at the ends and contain 6-15 cells
- Produces a few club-shaped microconidia
- Produces powdery tan or cinnamon-colored colonies with a bright yellow or yellow-orange reverse
- Found on cats and dogs
- M. equinum
- Found on horses
- Opportunistic infections in humans: scalp, face, trunk, limbs
- Found on horses
- M. fulvum
- Found in the soil
- Opportunistic infections in humans: face, trunk, limbs
- Found in the soil
- M. persicolor
- Found on rodents
- Opportunistic infections in humans: face, trunk, limbs
- Rapid-growing colonies with a thick surface texture, powdery center, white, cream or pink (after 7-14 days)
- Deep pink color on 1% peptone agar
- Numerous microconidia
- Slender, fusiform macroconidia with slightly rough walls
- M. audouinii
- Slow-growing, flat, velvety or cottony, matted, spreading colonies with the surface growth and silky texture
- Reverse is has a pink pigment the color of salmon, which turns orange-brown with age in 1-2 weeks
- Elongated microconidia along the hyphae
- Distorted, bizarre-shaped macroconidia, if seen, containing 2-9 cells
- Fluoresces under Wood's Lamp
- Causes outbreaks in children sometimes (scalp infection) and mostly affects children
- Grows poorly on rice grains, differentiating it from the others
- M. rivalieri is a variant form
- White folded colonies with a matte texture resembling ground glass
- Comb-like projections on the hyphae (pectinate)
- M. rivalieri is a variant form
- Slow-growing, flat, velvety or cottony, matted, spreading colonies with the surface growth and silky texture
Microsporum gypseum: *NOW RENAMED (Nannizzia gypsea spp complex)
Macroscopic Exam:
Microscopic Exam:
1. Microscopically, it produces lots of rough, thin-walled, elliptical macroconidia with 4-6 cells and a few club-shaped conidia along the hyphae.
This fungus can cause inflammatory dermatophytosis of the body or scalp. It is found in the soil and infections comes from contact with infected soil.
- This organism produces a powdery, buff-to-cinnamon colored colony with a tan reverse.
- The surface is flat and it spreads.
- The texture is powdery to granular.
- It typically develops a fringe around the border.
- It grows fairly quickly in just one week.
Microscopic Exam:
1. Microscopically, it produces lots of rough, thin-walled, elliptical macroconidia with 4-6 cells and a few club-shaped conidia along the hyphae.
This fungus can cause inflammatory dermatophytosis of the body or scalp. It is found in the soil and infections comes from contact with infected soil.
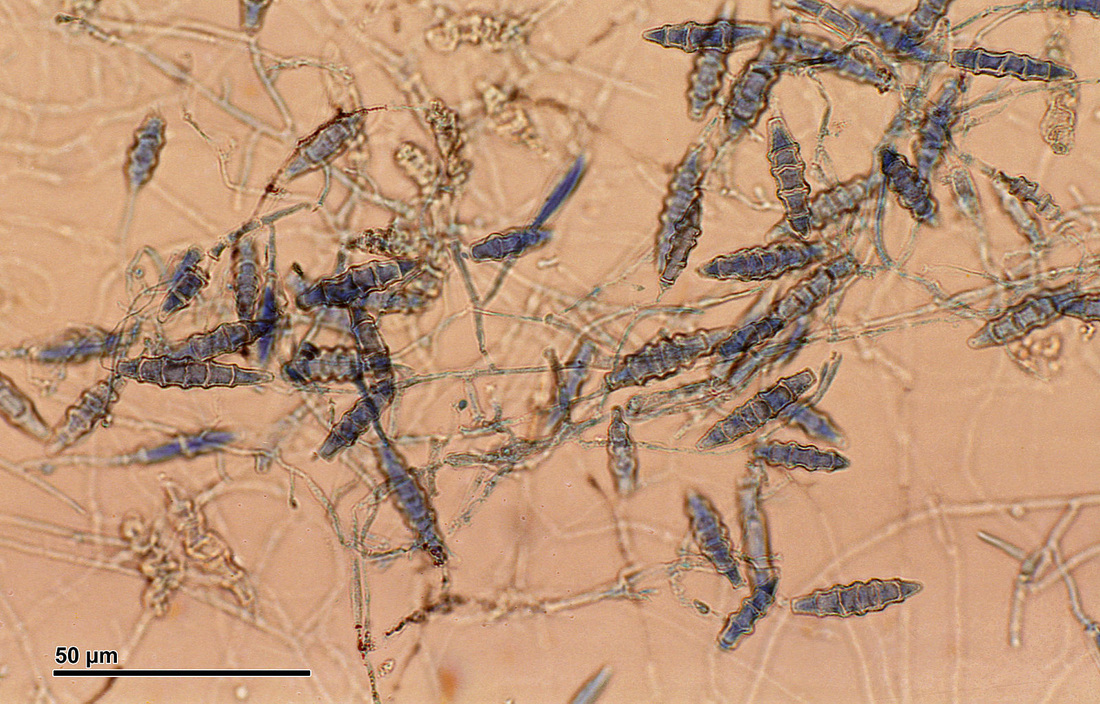
This moderately rapid grower matures in about 6 days, with a flat, spreading, powdery-to-granular surface and irregular border. The color ranges from buff to tan to brown, with a white border or cottony white center. The reverse may be a range of different colors. Microscopically, septate hyphae are observed with numerous macroconidia (4-6 celled), which are large, rough, thin-walled, and have a maximum of 6 compartments.By Doc. RNDr. Josef Reischig, CSc. - Author's archive, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=31556127
|
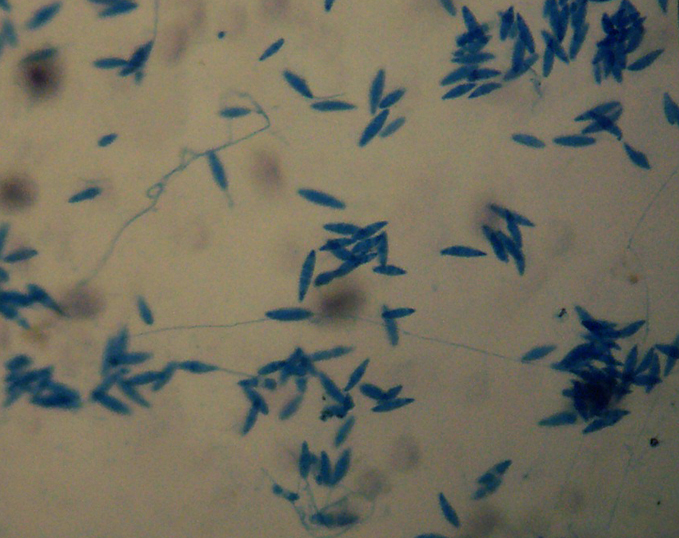
M. gypseum macroconidia have rounded, not pointed, ends;By Microrao - Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=7633551
|
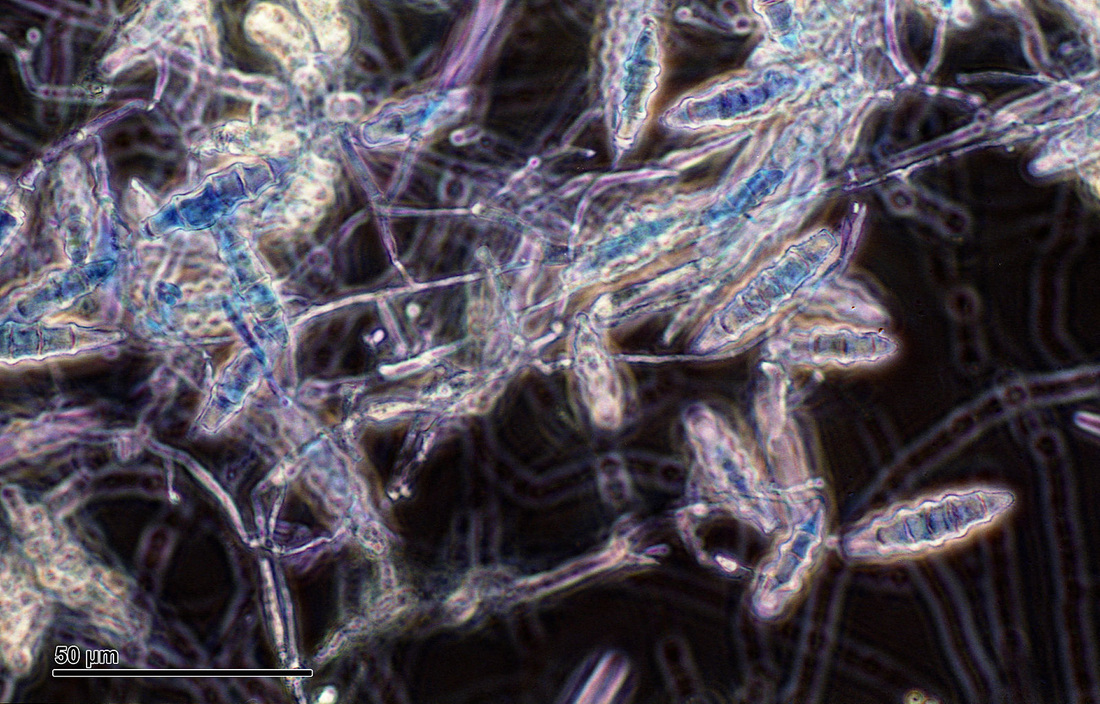
Microconidia are present along the hyphae, and they are shaped like clubs;By Doc. RNDr. Josef Reischig, CSc. - Author's archive, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=31556119
|
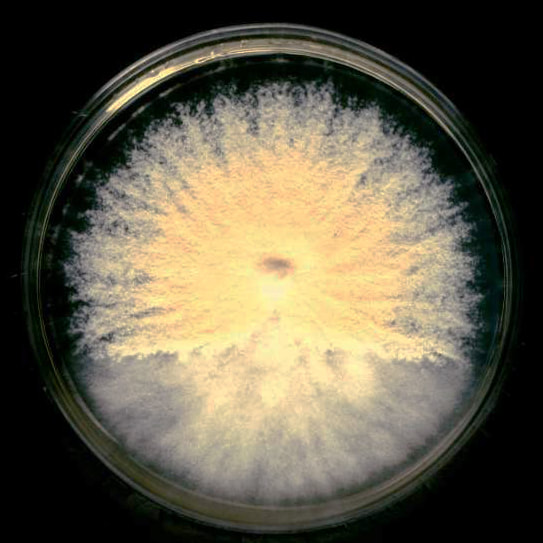
https://upload.wikimedia.org/wikipedia/commons/a/a1/Microsporum_gypseum_colony.JPG
|

Ringworm of the skin;By James Heilman, MD - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=19051050
|

By Medmyco at English Wikipedia - Transferred from en.wikipedia to Commons., CC0, https://commons.wikimedia.org/w/index.php?curid=48280468
|
Microsporum canis:
This fungus is a causative agent for scalp and skin infections, mainly in children. It also periodically causes nail infections.
Macroscopic Exam:
Microscopic Exam:
This fungus is a causative agent for scalp and skin infections, mainly in children. It also periodically causes nail infections.
Macroscopic Exam:
- Infected hairs fluoresce in Wood's Lamp. Cats and dogs serve as vectors or hosts from which humans acquire the infection.
- It produces rapid-growing colonies within 5 days with a flat surface with lots of aerial hyphae that start out as whitish and are fluffy or hairlike, silky or furlike, and often produce a yellowish pigment at the periphery.
- The center becomes buff-colored with age with a yellow-to-orange pigment seen on the reverse.
- There is also a glabrous form of the fungi, in which colonies are smooth and waxy in texture, feathery, with lots of growth at the edges.
Microscopic Exam:
- Fusiform, rough-walled, spindle-shaped macroconidia with tapered ends, containing 6-15 cells, are viewed borne on hyphae.
- There may be a few club-shaped microconidia.
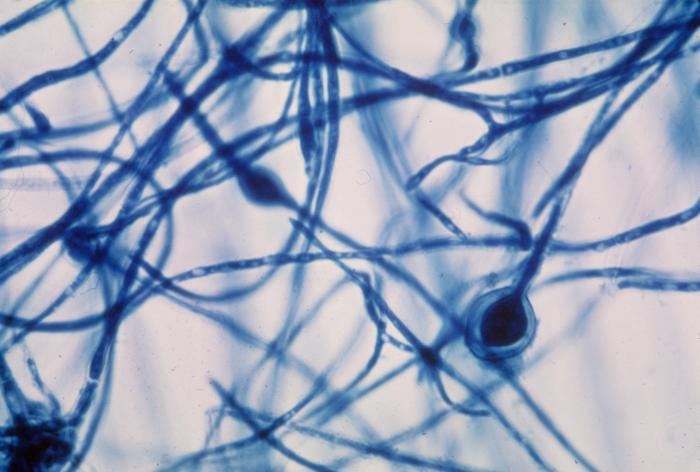
CDC/Dr. Lucille K. Georg - http://phil.cdc.gov/phil_images/20030129/25/PHIL_3054_lores.jpg
|

Spindle-shaped macroconidia
|

Macroconidia produced by M. canis are pointed at the ends, they are long, and the ends are characteristically tapered and "knob-like". The surface of the macroconidia are rough. Macroconidia typically have >6 compartments. Sometimes a few club-shaped microconidia along the hyphae may be seen as well;By Joel Mills (Own work) [GFDL (http://www.gnu.org/copyleft/fdl.html), CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/) or CC BY-SA 2.5-2.0-1.0 (https://creativecommons.org/licenses/by-sa/2.5-2.0-1.0)], via Wikimedia Commons

Hyphae are septate in M. canis;https://upload.wikimedia.org/wikipedia/commons/thumb/b/b0/Macroconidia_Microsporum_canis.JPG/1920px-Macroconidia_Microsporum_canis.JPG
|
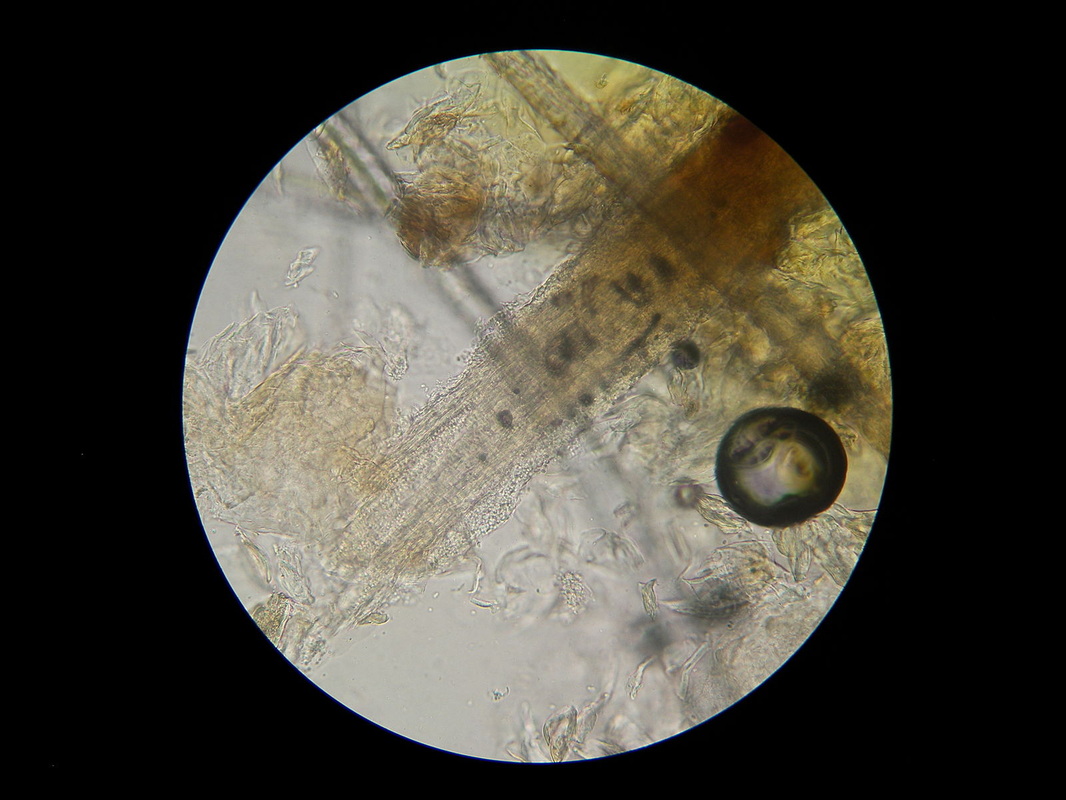
Hair invasion caused by M. canis;By Fourrure - http://www.flickr.com/photos/21345015@N06/8507416787/, CC BY-SA 2.0, https://commons.wikimedia.org/w/index.php?curid=24865286

Ringworm
|
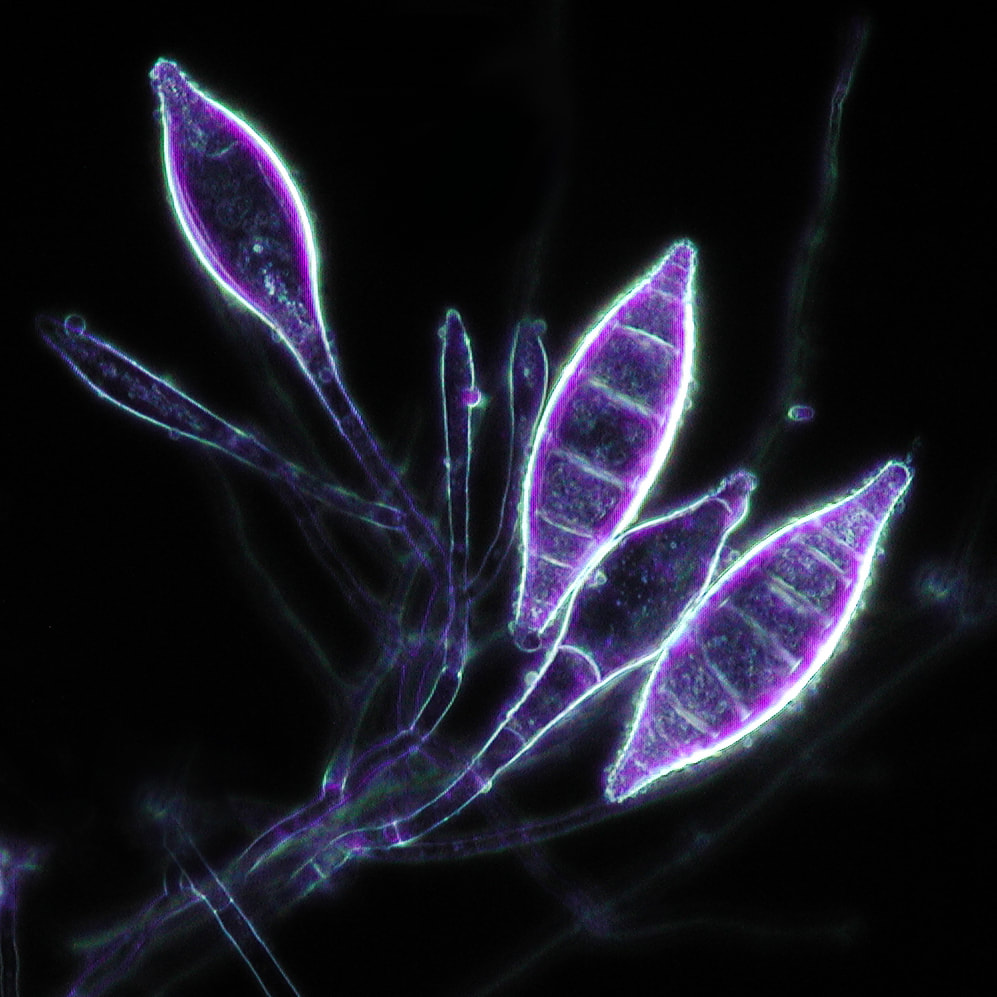
By Medmyco at English Wikipedia - Transferred from en.wikipedia to Commons., CC0, https://commons.wikimedia.org/w/index.php?curid=48280378
|
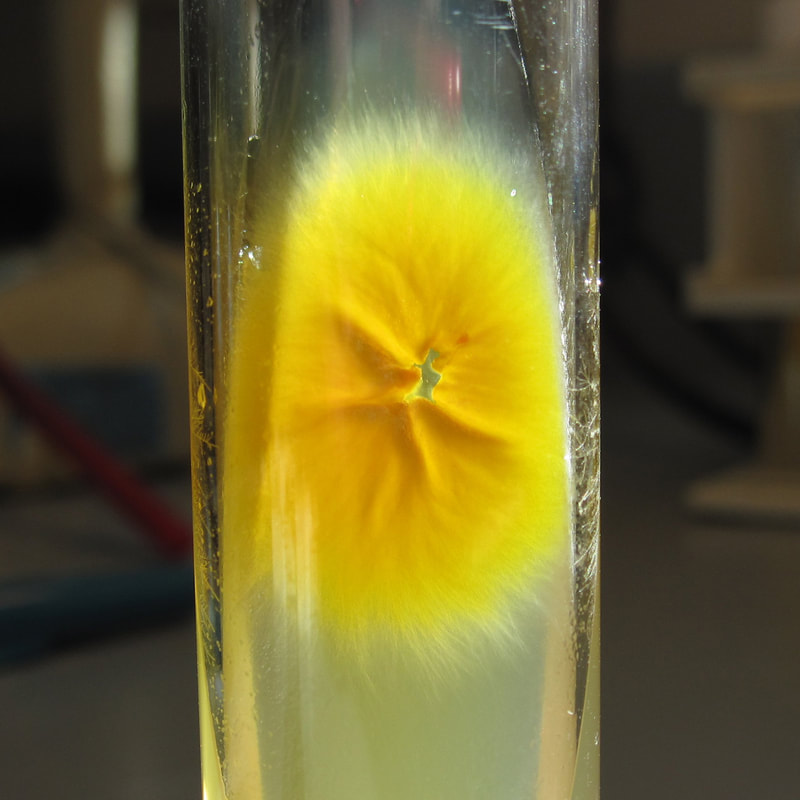
Medmyco at English Wikipedia [CC0], via Wikimedia Commons
|
Microsporum audouinii:
This species causes ringworm of the scalp in children, causing epidemics of tinea capitis, and infects skin as well. Rarely, it infects adults, too.
Macroscopic Exam:
Microscopic Exam:
This species causes ringworm of the scalp in children, causing epidemics of tinea capitis, and infects skin as well. Rarely, it infects adults, too.
Macroscopic Exam:
- It fluoresces under Wood's Lamp.
- It will not grow on polished rice grains. This distinguishes it from other Microsporum spp.
- It produces flat yellow, grayish or tannish white surfaace colonies on agar, which are downy-like or silky and radiate at the edges, with a salmon reverse with a red-brown center in about 6-10 days.
Microscopic Exam:
- Macroconidia that are bizarre-shaped, rare, and containing 2-9 cells are seen on LPCB stain.

M audouinii;By Medmyco at English Wikipedia - Transferred from en.wikipedia to Commons., CC0, https://commons.wikimedia.org/w/index.php?curid=30361673
|

Tinea capitis (scalp)
|
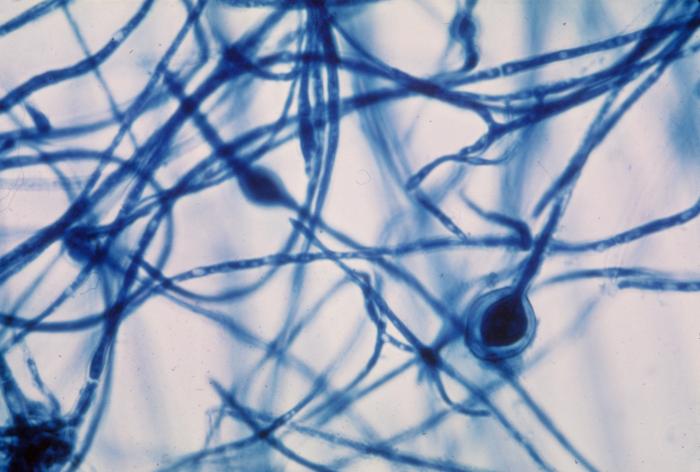
CDC/Dr. Lucille K. Georg - http://phil.cdc.gov/phil_images/20030129/25/PHIL_3054_lores.jpg
Epidermophyton floccosum:
This organism causes infection of the skin and nails, but not the hair, and is a common cause of tinea cruris, or "jock itch".
Macroscopic Exam:
Microscopic Exam:
This fungus causes epidermic dermatophytosis (athlete's foot) in summer camps and military settings, and it causes dermatophytosis of the nails and of the groin.
This organism causes infection of the skin and nails, but not the hair, and is a common cause of tinea cruris, or "jock itch".
Macroscopic Exam:
- It has colonies that are rapid growers, with a dull green or khaki-colored powdery surface that grow in about ten days.
- With age, the surfaces become folded with white floccose patches.
Microscopic Exam:
- Many raquet/club-shaped, rough-walled macroconidia occur, forming 2-4 cells borne singly or in clusters.
- There are no microconidia.
- Sometimes spiral hyphae can be seen, along with nodular bodies and chlamydoconidia.
This fungus causes epidermic dermatophytosis (athlete's foot) in summer camps and military settings, and it causes dermatophytosis of the nails and of the groin.

https://upload.wikimedia.org/wikipedia/commons/thumb/b/bc/14588_lores.jpg/640px-14588_lores.jpg
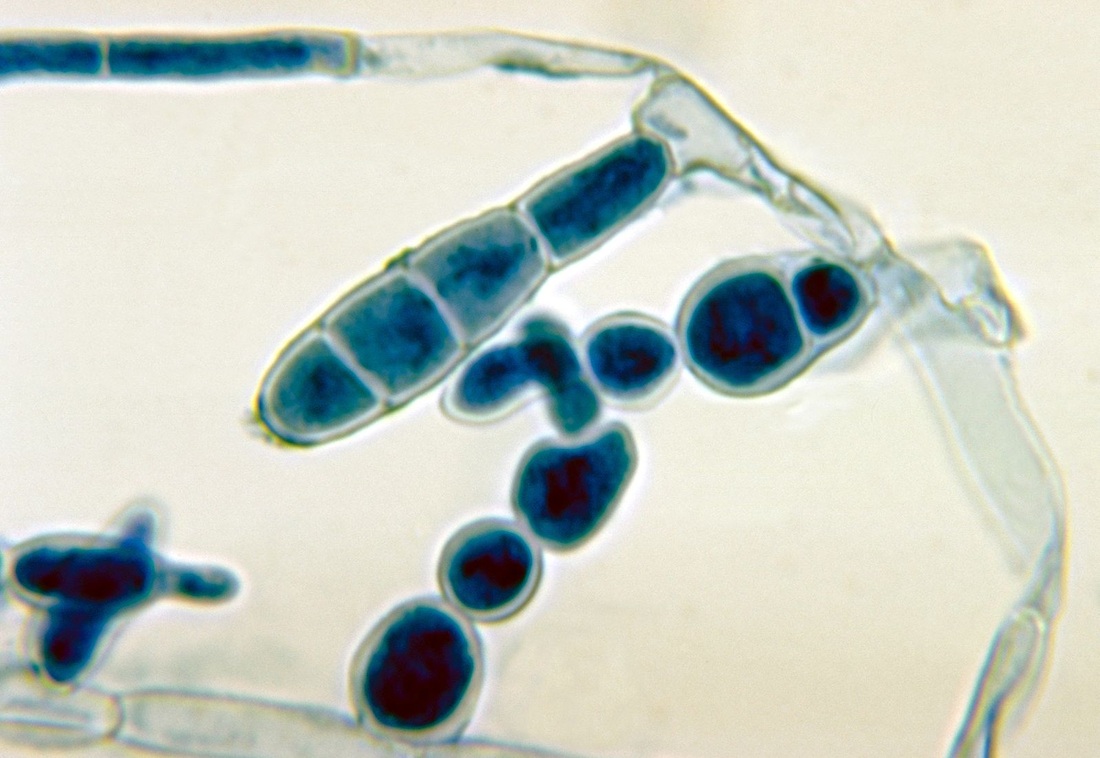
E. floccosum is characterized by septate hyphae without microconidia. In young cultures, macroconidia such as this one are smooth, thin and thick-walled, club-shaped structures with rounded ends, containing 2-6 cell compartments. They may be seen either in clusters or singularly.Public Domain, https://commons.wikimedia.org/w/index.php?curid=1857007

Epidermophyton
Trichophyton species:
- T. mentagrophytes
- After 7-10 days, fluffy colonies form with a white or cream, powdery, granular surface with a radiate margin or granular buff or rose-tan colonies with a brown, red or yellow reverse
- Lots of spherical microconidia born in clusters and along the sides of the hyphae
- Smooth-walled, cylindrical, pencil-shaped macroconidia containing 5-8 cells may be observed in granular strains, whereas rare macroconidia form in fluffy strains
- Spiral hyphae
- Urease positive in 2-4 days
- Ectothrix hair invasion in the hair perforation test with autoclaved hair
- Causes inflammatory dermatophytosis of the foot, body, nails, beard, scalp
- Most common cause of athlete's foot in general
- After 7-10 days, fluffy colonies form with a white or cream, powdery, granular surface with a radiate margin or granular buff or rose-tan colonies with a brown, red or yellow reverse
- T. rubrum
- Most prominent
- Variable morphology, but granular or fluffy white colonies with a pink periphery
- Ruby red, dark red or brown pigment diffuses into agar (see reverse)
- Deep red reverse forms in 2 weeks
- White, floccose colonies
- Numerous or few smooth-walled, pencil-shaped macroconidia bearing 3-8 cells
- Microconidia are numerous or scanty and oval in shape and borne along the sides of the hyphae
- Granular form with a coarse, folded surface is occasionally isolated, and this type also has numerous macroconidia
- Urease negative
- Does not perforate autoclaved hair
- Dermatophytosis of the body, foot, groin, nails
- May also cause abscesses or subcutaneous nodules
- Most prominent
- T. tonsurans
- Powdery, suede-like colonies that become folded with age OR granular white surface
- Surface color is white, gray, buff or yellow
- Reverse is colorless or yellow or mahogany
- Microconidia are numerous and vary in size, forming loose clusters, teardrop in shape, alternating along hyphae
- Chlamydospores
- Smooth-walled, club-shaped macroconidia (rare)
- Spiral hyphae (rare)
- Requires thiamine
- Urease positive after 4 days
- Does not perforate hair
- Causes >90% of cases of dermatophytosis of the scalp (tinea capitis) in the USA
- Causes epidemics in African American school-age children
- Causes black dot tinea capitis due to broken off hair shafts near the scalp
- It occasionally causes dermatophytosis of the body, foot, and nails
- Powdery, suede-like colonies that become folded with age OR granular white surface
- T. violaceum
- Glabrous colonies
- Slow-grower
- Hard texture
- Deep red to violet, waxy or suede, heaped colonies with a lavender reverse form in 2-3 weeks
- Microconidia and macroconidia are present or absent
- It requires thiamine to grow
- It causes dermatophytosis of the scalp and body and rarely of the foot, nails, or deep infections
- Glabrous colonies
- T. verrucosum
- Does not grow wel but if it does grow at all, it will produce a heaped, waxy, white or yellow colony with a colorless or yellow reverse in 2-3 weeks
- Only forms chlamydoconidia in chains or rare 3-5-celled rat-tail-shaped macroconidia
- Requires thiamine to grow and some strains also require inositol
- Causes dermatophytosis of the scalp, beard, body
- Infection occurs with contact from infected cattle
- Does not grow wel but if it does grow at all, it will produce a heaped, waxy, white or yellow colony with a colorless or yellow reverse in 2-3 weeks
- T. soudanense
- Slow-growing, glabrous colonies with a soft, brittle texture and prominent stellate fringe
- Orange to deep red with age
- Microconidia along hyphae (elongated)
- Branching on hyphae with short segments
- Slow-growing, glabrous colonies with a soft, brittle texture and prominent stellate fringe
- T. schoenleinii
- Favic chandeliers form, resembling deer antlers
- Slow-grower
- Glabrous
- White or gray with rough, waxy colonies form that are heaped, light yellow, buff with a convoluted surface and a colorless or yellow-orange reverse in 2-3 weeks
- No macroconidia form
- Microconidia are formed on rice grains
- Can cause a severe type of dermatophytosis of the scalp known as favus
- Favic chandeliers form, resembling deer antlers
- T. interdigitale
- White, floccose colonies that become cream colored and powdery in the center once the conidia develop
- Abundant microconidia (spherical), borne in clusters along the hyphae
- Cylindrical, smooth-walled macroconidia
- Spiral hyphae
- Urease positive
- White, floccose colonies that become cream colored and powdery in the center once the conidia develop
- T. equinum
- Requires nicotinic acid
- Requires nicotinic acid
- T. erinacei
- Rapid-growing colonies with a white, powdery surface and bright yellow pigment on the reverse
- Lots of elongated microconidia borne along the hyphae
- Inability to attack urea
- Rapid-growing colonies with a white, powdery surface and bright yellow pigment on the reverse
- T. concentricum
- Slow-grower
- Glabrous and soft texture
- Gray or buff colonies that are folded
- Hyphal swellings and chlamydospores
- Microconidia and macroconidia are absent or rare
- Slow-grower
Trichophyton mentagrophytes:
This fungus has the capability of invading all parts of the body, including the nails and the hair, and is THE MOST common cause of "athlete's foot" (tinea pedis).
Macroscopic Exam:
Microscopic Exam:
This fungus has the capability of invading all parts of the body, including the nails and the hair, and is THE MOST common cause of "athlete's foot" (tinea pedis).
Macroscopic Exam:
- It produces either fluffy white colonies or granular buff-colored to rose to tan-colored colonies after 7-10 days on SABHI agar at room temperature.
- The reverse is colorless to yellow, brown or red.
- Red strains are difficult to differentiate from T. rubrum.
- There is NO diffusion of red pigment into the agar as there is for T. rubrum.
- It produces a POSITIVE UREASE agar test in 2-4 days on Christenson's urea agar at room temperature.
Microscopic Exam:
- Granular forms will produce numerous, pencil-shaped, smooth, thin-walled macroconidia, containing 5-8 cells.
- Fluffy strains produce rare macroconidia.
- Granular forms will produce numerous or few round microconidia in grapelike clusters along the hyphae.
- Fluffy strains produce a few teardrop or club-shaped microconidia singly along the hyphae.
- You may also see racquet hyphae, spiral hyphae, nodular bodies, and chlamydoconidia.
- It perforates autoclaved hair in vitro.

T. mentagrophytes, Image by Jeanette Reynolds, MLS-AMT, M-ASCP (cm), 2015, own work
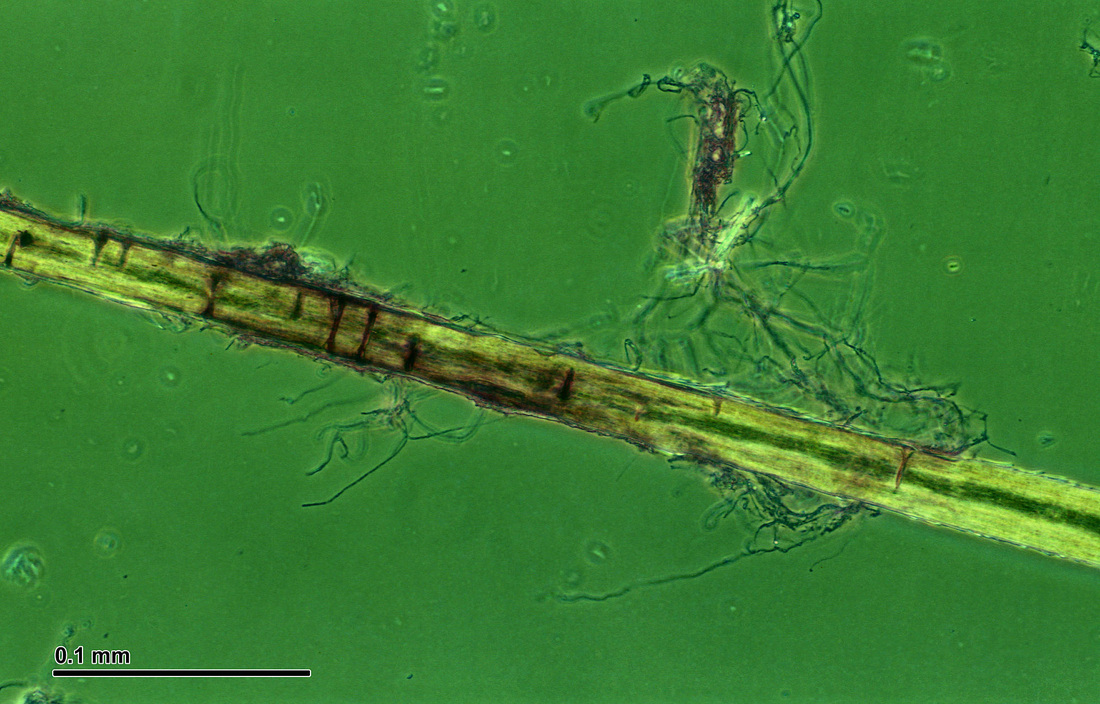
T. mentagrophytes causing an endothrix hair invasion
|
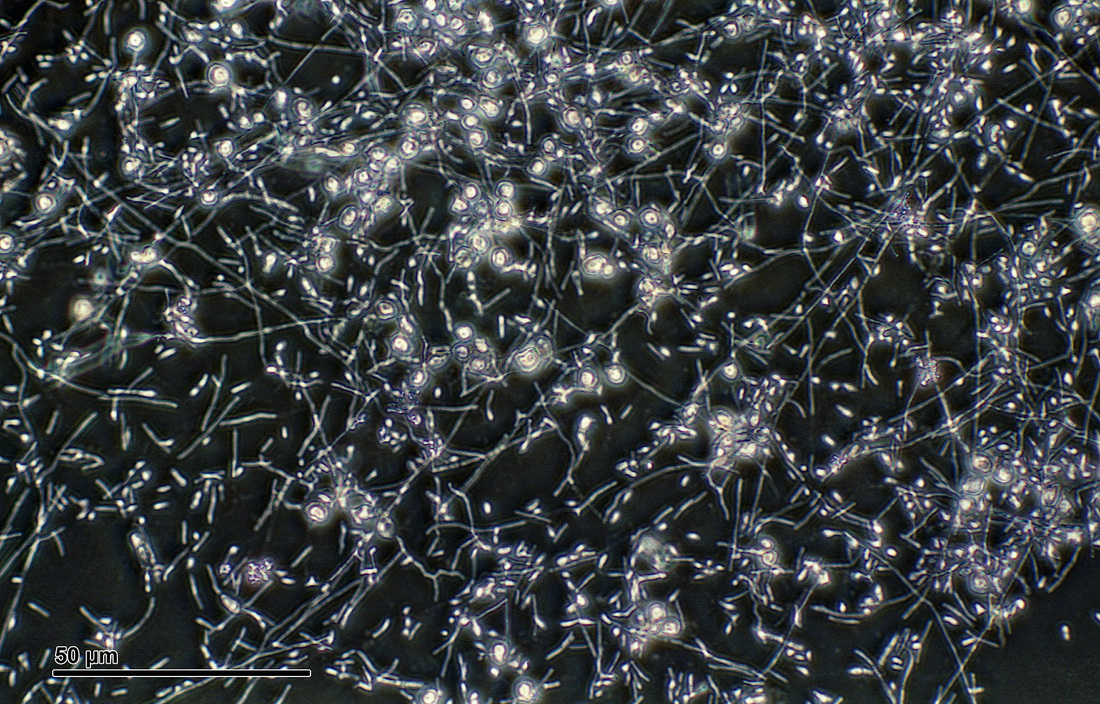
T. mentagrophytes seen fluorescing
|
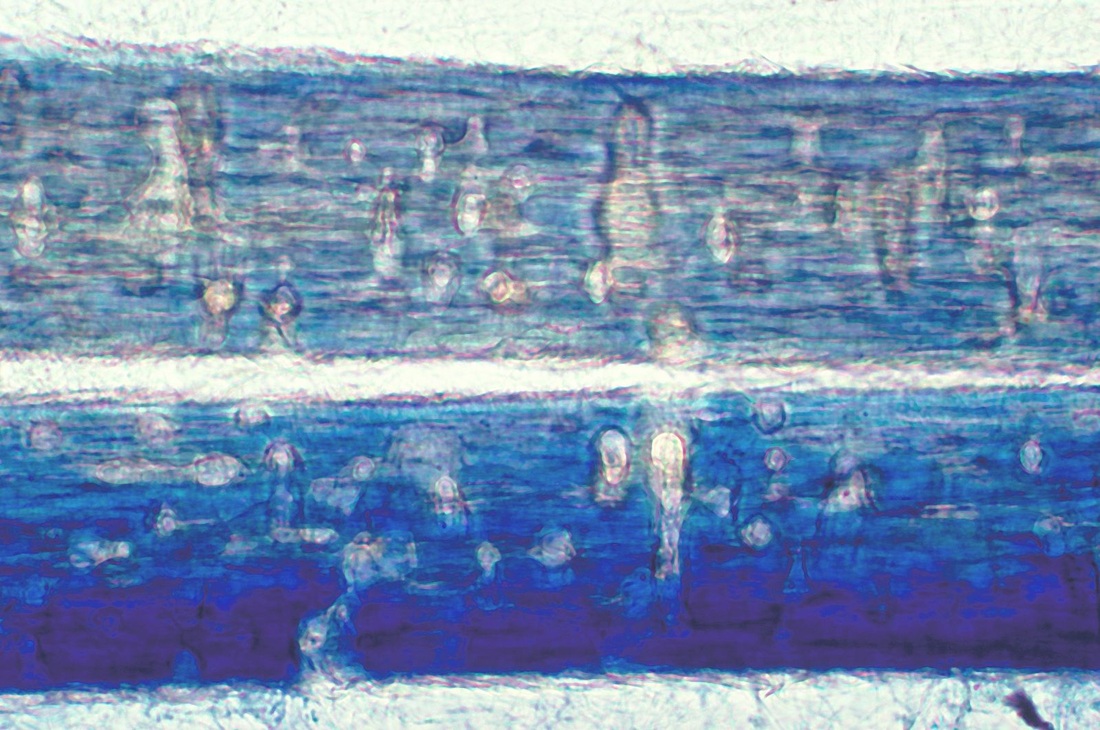
Lactophenol cotton blue staining of T. mentagrophytes invasion of hair (endothrix)
|

T. mentagrophytes is a moderate-grower, maturing in 7-10 days. Growth patterns vary. Texture may range from powdery to downy, and buff to white in color, maturing to a pink or yellow color. Concentric and radial folds may be present, as seen in this image. A dense fluff may develop, and little to no conidiation may be present. The reverse varies greatly in color.
|
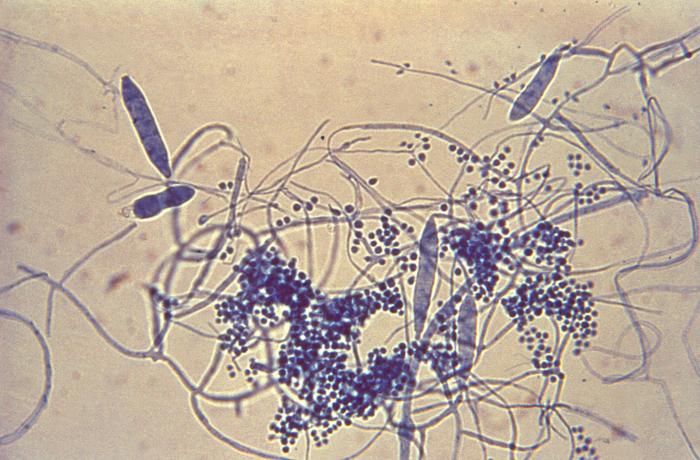
LPCB stain of T. mentagrophytes from a granular strain, showing numerous pencil-shaped macroconidia and numerous round microconidia in grapelike clusters.
|
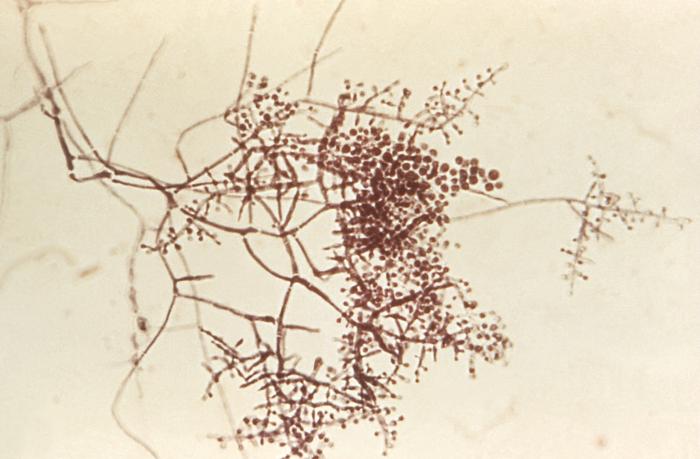
|
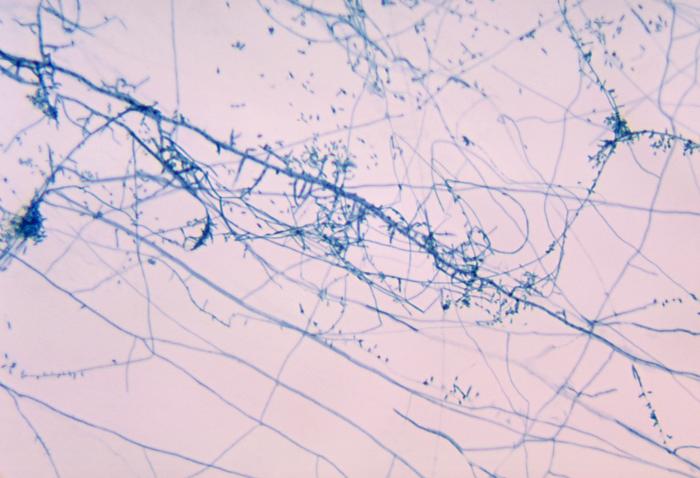
LPCB stain from a fluffy white strain of T. mentagrophytes produces rare macroconidia, and few-to-many teardrop or club-shaped microconidia along the hyphae.
|

This one is a fluffy white strain.
|

Onychomycosis may be caused by T. mentagrophytes (nail infection)
|

Athlete's foot is commonly caused by T. mentagrophytes
|

A severe case of Athlete's foot is seen here
|
T. mentagrophytes young growth
|

Wood's Lamp UV Lamp for fluorescence
Trichophyton rubrum:
This organism infects the skin and nails, the foot, groin, and rarely, the scalp (tinea capitis) or beard (tinea barbae). This one is the most common dermatophyte that infects humans overall. In patients who are immunosuppressed or immunocompromised, it is linked to abscesses and subcutaneous nodules.
Macroscopic Exam:
Microscopic Exam:
This organism infects the skin and nails, the foot, groin, and rarely, the scalp (tinea capitis) or beard (tinea barbae). This one is the most common dermatophyte that infects humans overall. In patients who are immunosuppressed or immunocompromised, it is linked to abscesses and subcutaneous nodules.
Macroscopic Exam:
- At room temperature, on SABHI agar, this organism produces either granular or fluffy white colonies with a pink periphery after 2 weeks.
- It produces a red reverse that is deep red, and it diffuses into the agar.
- The urease test is NEGATIVE, differentiating it from T. mentagrophytes.
- It does not perforate autoclaved hair.
Microscopic Exam:
- It produces numerous or a few smooth-walled, pencil-shaped macroconidia with 3-8 cells.
- It produces numerous club-shaped microconidia borne singly along the hyphae.
- It may also produce racquet hyphae, nodular bodies, and/or chlamydoconidia.
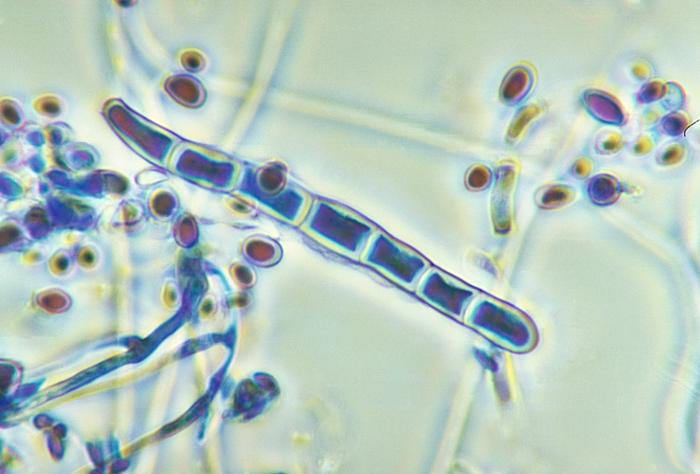
T. rubrum is characterized by septate hyphae with teardrop-shaped microconidia that are lateral. Macroconidia, as seen in the image above, are long, narrow, thin-walled structures with anywhere from 2-8 compartmental cells that form directly on the ends of hyphae as single or groups of macroconidia.
|
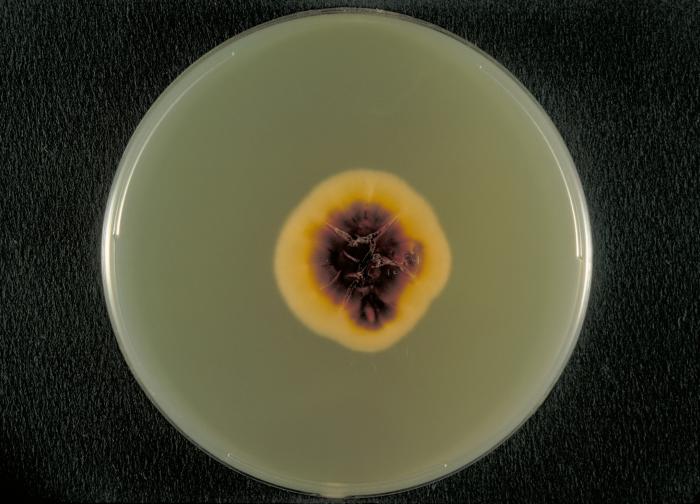
Characteristic deep "reddish-purple" reverse of T. rubrum. Pigment is best observed on cornmeal dextrose agar. This slow grower takes about 14 days to mature. The surface appears fluffy or granular. The surface color ranges from white to buff.
|

|

T. rubrum is a causative agent of tinea barbae, an infection of the beard follicles
|

|
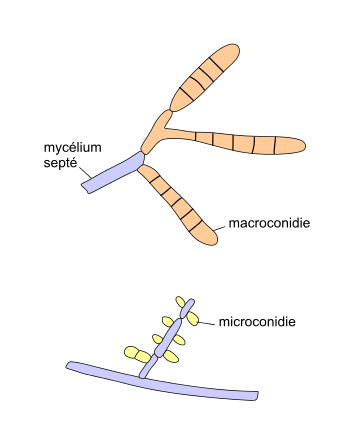
|

Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
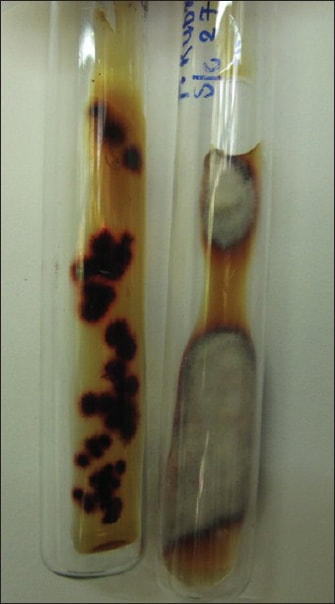
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
Trichophyton tonsurans:
This is the main cause of tinea capitis, or scalp ringworm, in the USA, though it also causes infections of the skin, foot and nails. In fact, over 90% of the cases of dermatophytosis of the scalp in the USA are caused by it.
It also causes epidemics of black dot tinea capitis in school-aged African American children, producing broken off hair shafts near the scalp.
Macroscopic Exam:
Microscopic Exam:
This is the main cause of tinea capitis, or scalp ringworm, in the USA, though it also causes infections of the skin, foot and nails. In fact, over 90% of the cases of dermatophytosis of the scalp in the USA are caused by it.
It also causes epidemics of black dot tinea capitis in school-aged African American children, producing broken off hair shafts near the scalp.
Macroscopic Exam:
- On SABHI at room temperature, there are three different colony types that may be observed after 1-2 weeks:
- Suede-like, gray-white colony with a mahogany reverse
- Granular white with a colorless reverse
- Granular-to-suede-like, bright yellow, rugose colony with a yellow reverse
- It is UREASE POSITIVE after 4 days.
- It does not perforate autoclaved hair.
- It grows extremely well in the presence of thiamine.
Microscopic Exam:
- It produces rare, smooth-walled, club-shaped macrocondia.
- It produces numerous microconidia, which show great variation in size and shape.
- Chlamydoconidia and racquet hyphae may be observed.
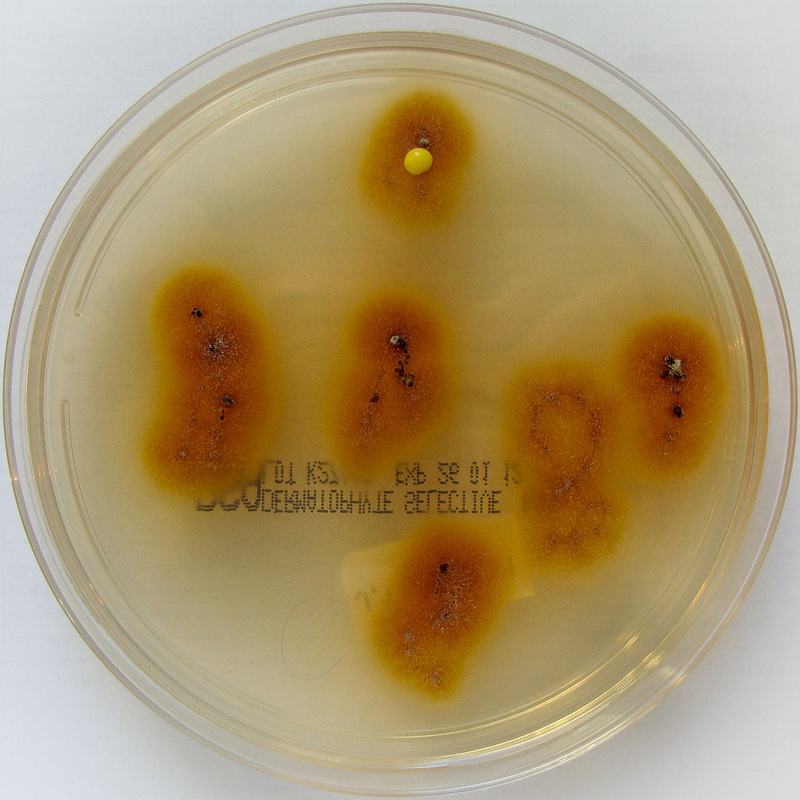
|
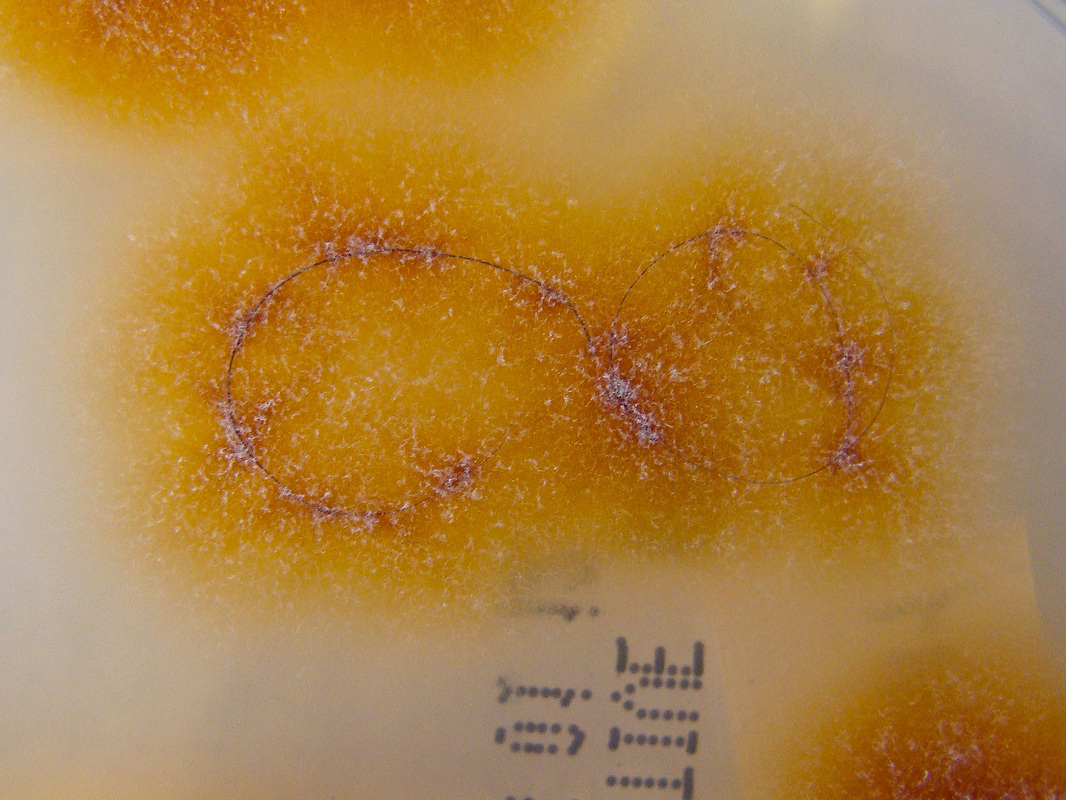
|


|

|
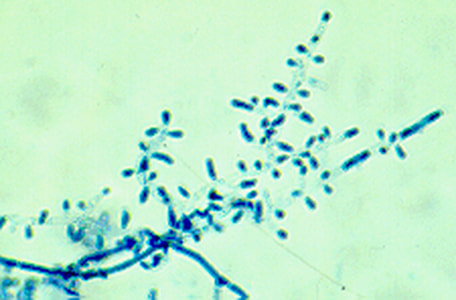
|
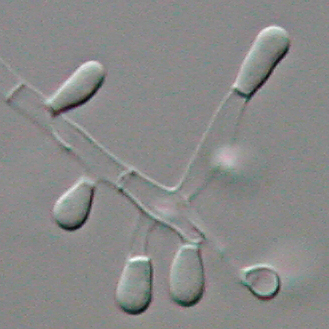
|
Trichophyton terrestre: *Now Arthroderma terrestre spp complex
It does not cause infection in humans.
Macroscopic Exam:
It produces pink-to-salmon, umbonate colonies on SABHI agar, resembling Fusarium spp.
Microscopic Exam:
It produces club-shaped microconidia on short stalks or larger, peg-shaped microconidia on septate hyphae.
It does not cause infection in humans.
Macroscopic Exam:
It produces pink-to-salmon, umbonate colonies on SABHI agar, resembling Fusarium spp.
Microscopic Exam:
It produces club-shaped microconidia on short stalks or larger, peg-shaped microconidia on septate hyphae.

Trichophyton mariatii:
This organism primarily causes tinea barbae, infection of the beard, but also causes scalp or skin infections (very rare infection).
Macroscopic Exam:
This organism primarily causes tinea barbae, infection of the beard, but also causes scalp or skin infections (very rare infection).
Macroscopic Exam:
- It produces either fluffy white, rugose colonies or waxy, heaped, rugose colonies that are light yellow or buff in color.
- The reverse is colorless or yellow-orange.

|

|
Trichophyton schoenleinii:
This fungus causes "favus", which is a chronic conidition of the scalp resulting in scarring and permanent hair loss. It also occasionally infects the skin and nails.
Macroscopic Exam:
Microscopic Exam:
This fungus causes "favus", which is a chronic conidition of the scalp resulting in scarring and permanent hair loss. It also occasionally infects the skin and nails.
Macroscopic Exam:
- On SABHI at room temperature, this organisms produces waxy, heaped, light yellow or buff-colored colonies in 2 weeks.
- It produces a colorless or yellow-orange reverse.
Microscopic Exam:
- Microscopic typical favic chandeliers will be observed, resembling deer or moose antlers.
- No macroconidia are exhibited.
- Chlamydoconidia and hyphal swellings may also be observed that appear irregular and knob-like.
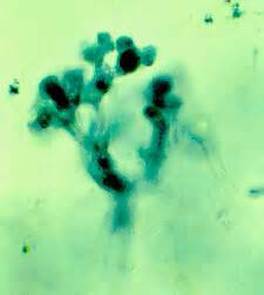
Typical favic chandeliers seen in T. schoenleinii
|

The image above shows the reverse of T. schoenleinii, which is tan but can also be yellowish orange or even colorless. The surface is waxy, white or downy, folded or heaped, and looks like yeast.
|
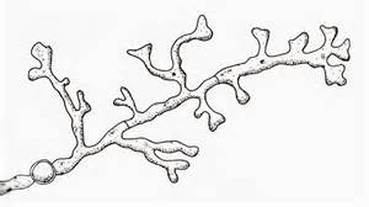
Favic chandeliers
Trichophyton ajelloi:
This organism rarely causes disease in humans.
This organism rarely causes disease in humans.
Trichophyton violaceum:
This fungus infects the skin, hair, scalp, foot, and nails. It rarely produces deep infections.
Macroscopic Exam:
Microscopic Exam:
This fungus infects the skin, hair, scalp, foot, and nails. It rarely produces deep infections.
Macroscopic Exam:
- On SABHI agar at room temperature, the most distinguishing feature about this fungus is its purple waxy or suede, heaped colony in 2-3 weeks.
- It also produces a lavender reverse.
- It grows best with thiamine and trypticase.
Microscopic Exam:
- Macroconidia are not produced or are rarely produced.
- It produces chlamydoconidia in chains and hyphal swellings.
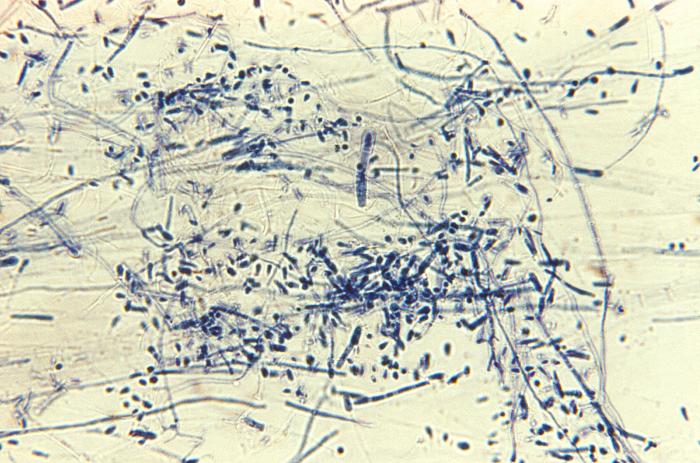
|
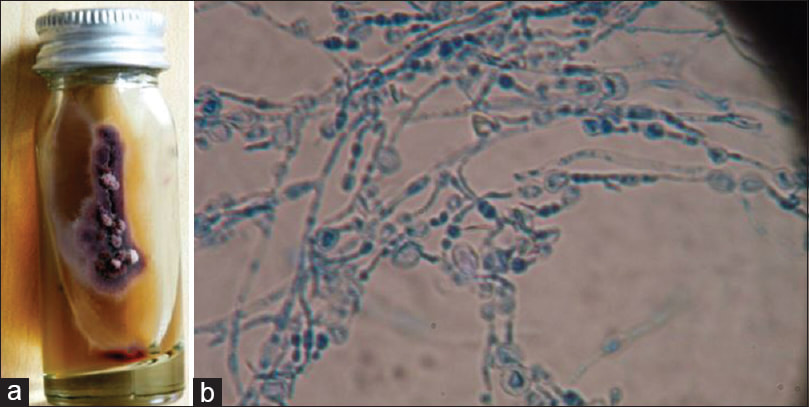
http://www.jlponline.org/articles/2015/7/2/images/JLabPhysicians_2015_7_2_84_163135_f4.jpg; Trichophyton violaceum
|
Appropriate treatment for dermatophytosis includes a topical agent, such as one of the azoles. Dermatophytes of the scalp or extensive cases of dermatophytosis need something stronger and should be treated systemically with griseofulvin. Dermatophytosis of the nails requires prolonged therapy for 3-12 months with either griseofulvin or itraconazole.
Neoscytalidium dimidiatum is a rare cause of ringworm, tinea, dermatophytosis, or onychomycosis. Because it is a soil inhabitant, it infects humans who come into contact with contaminated soil or plant materials. Rarely, it causes systemic disease and fatality in the immunocompromised individual. Colonies are rapid-growing, brown-to-black due to the production of the pigment melanin, and they are woolly or furry in texture.
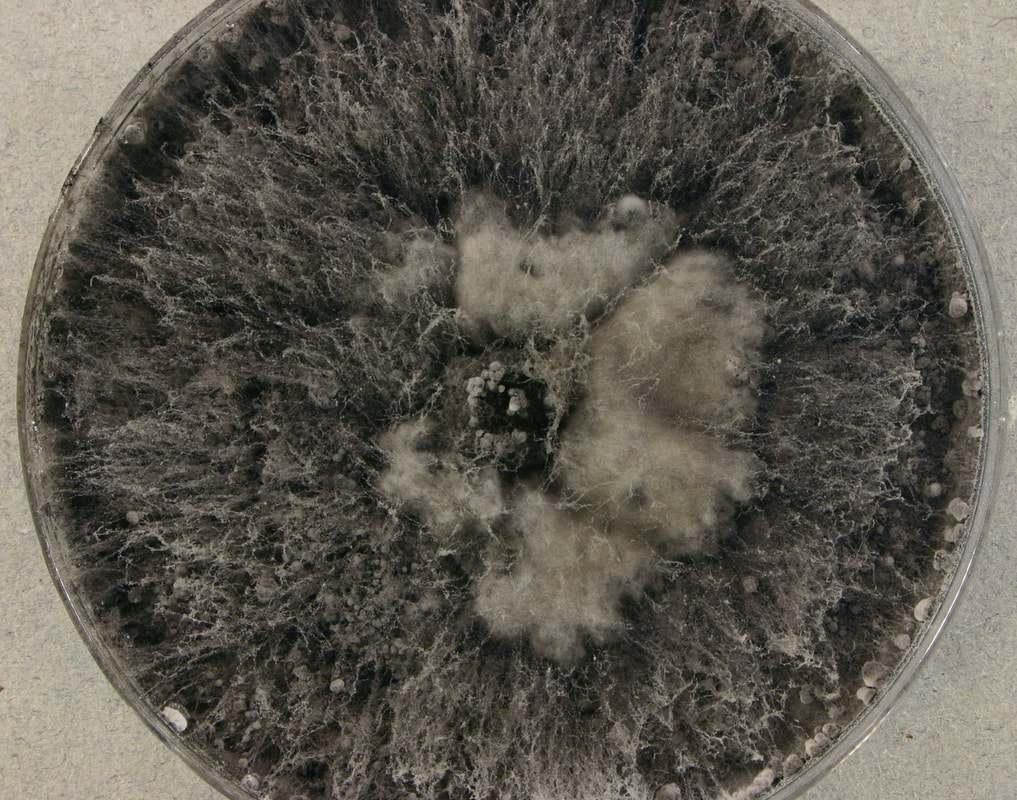
By Medmyco - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=53542147
|
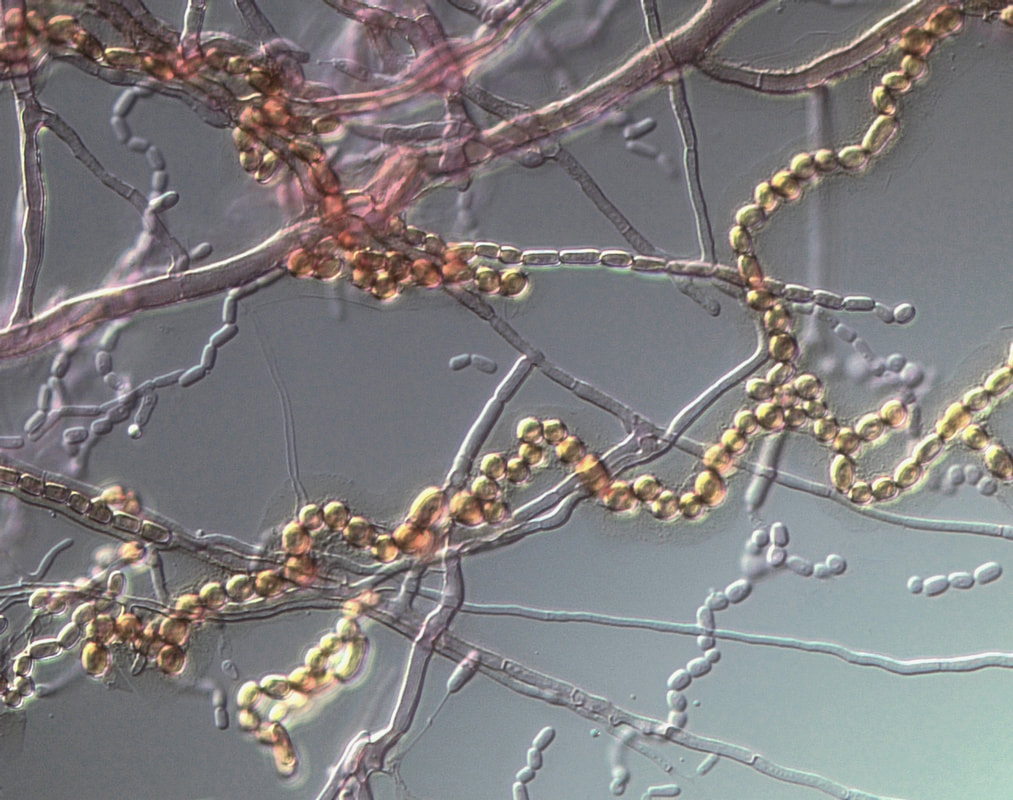
By Medmyco - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=53542146
|
Dermatophytosis Progression and Healing (Tinea Ringworm):
Typically, this type of dermatophytosis is limited to the superficial, keratinzied layer of the skin, hair, or nails. If a person is immunosuppressed or immunocompromised, however, the healing process may take longer, and in fact, become chronic, and the lesions may extend deeper into the deeper layers of skin or spread into the tissues.
If you have pets and notice that they exhibit signs of ringworm, they can serve as vectors for infection, so you should examine anyone who has come into contact with the infected pets. Pets should be treated, as well as the individuals interacting with them. If one family member is infected, the whole family should be treated. Ringworm is highly contagious and it can spread from towels, linens (fomites) through indirect contact, as well as through direct contact (touch, skin-to-skin).
- During the first week of infection, the initial follicular lesion is covered by a circular, and sometimes target-shaped, area of erythema. Sometimes it is itchy. With skin scrapings at this point, a positive culture can be obtained from the central region up to 40 mm into the periphery at around 7 days.
- During the second week of infectio, some smaller satellite lesions may form around the original lesion. It will reach its peak, and positive cultures can be obtained from skin scrapings up to 45 mm into the periphery.
- By the third week of infection, the intial lesion will be at its maximum size. It will start to heal in the middle. Skin scrapings at this point should be obtained from just the outer red ring, but not from the center, because the center will heal first.
- By the fourth and fifth weeks, healing from the center outward continues, and skin scraping cultures from the healed areas will be negative.
- By week six, the lesion will be completely healed and any skin scraping cultures will be negative.
Typically, this type of dermatophytosis is limited to the superficial, keratinzied layer of the skin, hair, or nails. If a person is immunosuppressed or immunocompromised, however, the healing process may take longer, and in fact, become chronic, and the lesions may extend deeper into the deeper layers of skin or spread into the tissues.
If you have pets and notice that they exhibit signs of ringworm, they can serve as vectors for infection, so you should examine anyone who has come into contact with the infected pets. Pets should be treated, as well as the individuals interacting with them. If one family member is infected, the whole family should be treated. Ringworm is highly contagious and it can spread from towels, linens (fomites) through indirect contact, as well as through direct contact (touch, skin-to-skin).
the hyaline molds:
The hyaline molds produce hyaline or light-colored hyphae, however, the colonies themselves may be dark with dark conidia. The hyphae and conidia will typically stain blue in the LPCB wet mounts.
This section discusses the common light-colored molds that can cause subcutaneous disease. Subcutaneous tissues are those that lie beneath the epidermal and dermal layers of skin, beginning with the fatty layer, which can seed through the bloodstream deeper into the tissues.
This section discusses the common light-colored molds that can cause subcutaneous disease. Subcutaneous tissues are those that lie beneath the epidermal and dermal layers of skin, beginning with the fatty layer, which can seed through the bloodstream deeper into the tissues.
Scedosporium apiospermum spp complex:
This mold is light, however, it is considered to be a thermally dimorphic mold. This is the asexual stage of the mold, whereas Pseudallescheria apiospermum is the teleomorph, or sexual stage, of the mold.
It is isolated from the soil or stagnant water and is considered an agent of phaeohyphomycosis, even though the hyphae are hyaline and transparent in color. This can cause infections on the upper and lower extremeties or other exposed parts of the body. It can cause infections of the subcutaneous tissues, muscles, tendons, and bones. Disseminated infections can lead to the lungs, sinuses, eyes, central nervous system, and others.
In cases where a person has a near-drowning experience, this is the most common cause of fatal lung or central nervous system infections resulting from that in a complication. Immunocompromised patients are at highest risk of infection with the mold. It can be quite invasive in such individuals, and it can cause a lung infection that resembles aspergillosis. Patients with underlying cystic fibrosis can become colonized with this mold and can suffer from recurrent lung infections triggered by it.
They are instrinsically resistant to voriconazole, but most are susceptible to amphotericin B.
This mold is light, however, it is considered to be a thermally dimorphic mold. This is the asexual stage of the mold, whereas Pseudallescheria apiospermum is the teleomorph, or sexual stage, of the mold.
It is isolated from the soil or stagnant water and is considered an agent of phaeohyphomycosis, even though the hyphae are hyaline and transparent in color. This can cause infections on the upper and lower extremeties or other exposed parts of the body. It can cause infections of the subcutaneous tissues, muscles, tendons, and bones. Disseminated infections can lead to the lungs, sinuses, eyes, central nervous system, and others.
In cases where a person has a near-drowning experience, this is the most common cause of fatal lung or central nervous system infections resulting from that in a complication. Immunocompromised patients are at highest risk of infection with the mold. It can be quite invasive in such individuals, and it can cause a lung infection that resembles aspergillosis. Patients with underlying cystic fibrosis can become colonized with this mold and can suffer from recurrent lung infections triggered by it.
They are instrinsically resistant to voriconazole, but most are susceptible to amphotericin B.
Macroscopic Exam:
Microscopic Exam:
- On SABHI agar at room temperature, this fungus produces a fluffy white colony fairly quickly, since it is a rapid-grower, turning gray with age.
- The reverse is gray.
- Though it may resemble several other molds, it is NOT a dimorphic mold and CANNOT be converted to a yeast form.
Microscopic Exam:
- When the mold is in its asexual stage, it will produce a large single or small clustered, oval-shaped (balloon-shaped) annelloconidia terminally on long or short annellophores with a "crooked neck", or along the sides of the hyphae.
- When the mold is in its sexual stage, it will produce large brown cleistothecia, ranging from 50-200 micrometers in diameter. When they rupture, they release asci containing 8 light brown, oval-shaped ascospores. The sexual stage of the mold is known as Pseudallescheria boydii.

Mold colonies of Scedosporium spp
|

Microscopic exam of Scedosporium spp in its asexual stage.
|
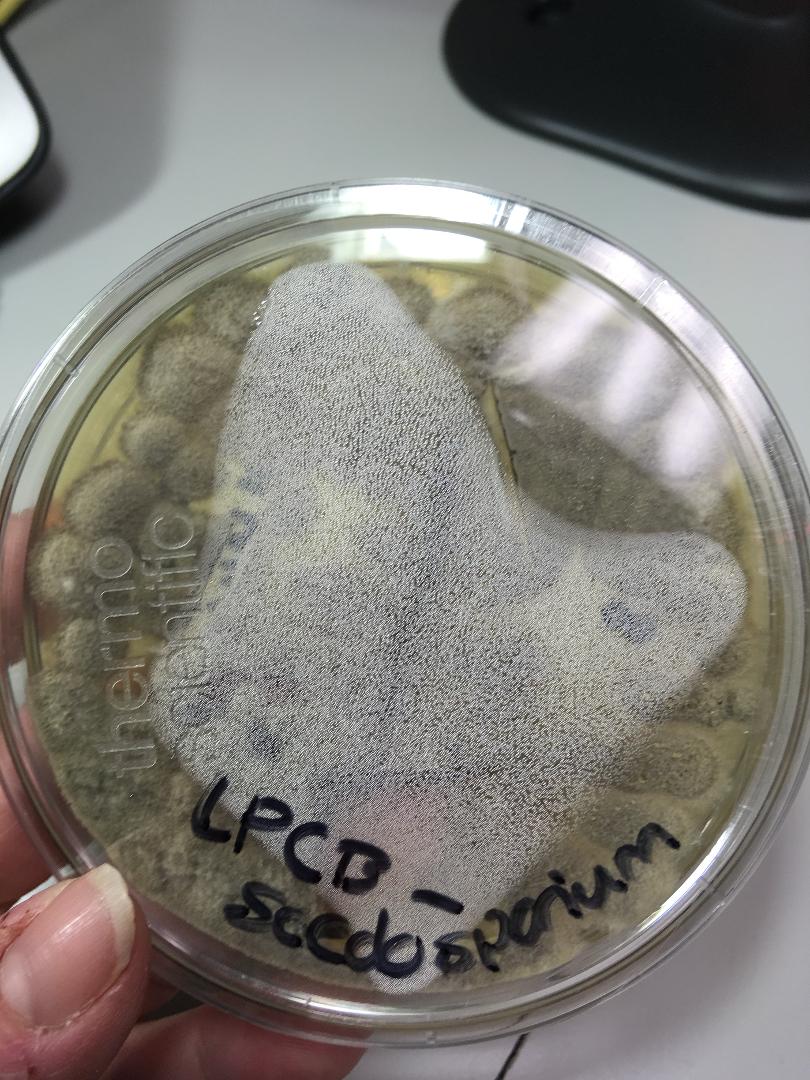
Scedosporium spp on Potato Dextrose Agar; This spp forms beige-tan-white colonies that are velvety and round, and microscopic spores are oval/lemon-shaped with a flat edge on one side and a bent or crooked "neck" where they connect; Image by Jeanette Reynolds, M-ASCP, MT-AMT, MS-Biology, Microbiologist
|
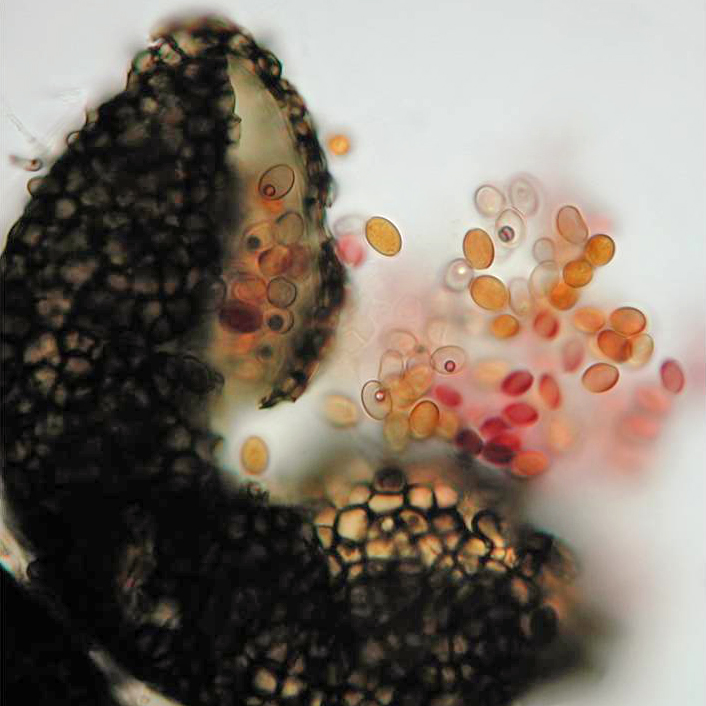
This is a brown cleistothecia rupturing, releasing asci and ascopsores. This is the sexual stage of Scedosporium, also named Pseudallescheria boydii. https://upload.wikimedia.org/wikipedia/commons/e/ea/Pseudallescheria_boydii.jpg
|
This species is associated with traumatic implanation of the fungus via contaminated thorns or wood splinters. In the USA, it is the most common agent of mycetoma. It is also linked to pulmonary disease, sinusitis, and even fungus ball in the lungs. It can cause keratomycosis of the eyes, prostatitis in men, chronic otomycosis (ear infection), meningomycosis (meningitis), and systemic disease due to its ability to seed to other areas of the body and spread.
Scedosporium prolificans: *NOTE: This has been renamed to Lomentospora prolificans
This fungal strain has been linked to invasive infections, particularly fungal endocarditis, osteomyelitis of the bones, and arthritis. It has also been associated with systemic infections in neutropenic and immunocompromised patients. There have been even documented nosocomial (hospital-acquired) infections leading to fatality in leukemia patients. Often times, infection begins with traumatic inoculation of the fungus, which can become disseminated throughout the body in a variety of sites. In addition to the infections listed above, it has also been linked to lung infections and brain infections. Disseminated infections are often fatal.
It is resistant to many of the current antifungal agents. Infections are often treated with ketoconazole or amphotericin B along with flucytosine.
Macroscopic Exam:
Microscopic Exam:
This fungal strain has been linked to invasive infections, particularly fungal endocarditis, osteomyelitis of the bones, and arthritis. It has also been associated with systemic infections in neutropenic and immunocompromised patients. There have been even documented nosocomial (hospital-acquired) infections leading to fatality in leukemia patients. Often times, infection begins with traumatic inoculation of the fungus, which can become disseminated throughout the body in a variety of sites. In addition to the infections listed above, it has also been linked to lung infections and brain infections. Disseminated infections are often fatal.
It is resistant to many of the current antifungal agents. Infections are often treated with ketoconazole or amphotericin B along with flucytosine.
Macroscopic Exam:
- It produces a fluffy white colony quickly, later turning gray.
- It has a gray reverse.
Microscopic Exam:
- It produces hyaline, septate hyphae, which bear balloon-shaped, teardrop-shaped annelloconidia at the tips of annellophores with inflated bases and tapering tips.
- It does not demonstrate a sexual stage like the other strain of Scedosporium apiospermum.

https://upload.wikimedia.org/wikipedia/commons/thumb/d/df/Scedosporium_prolificans.jpg/640px-Scedosporium_prolificans.jpg
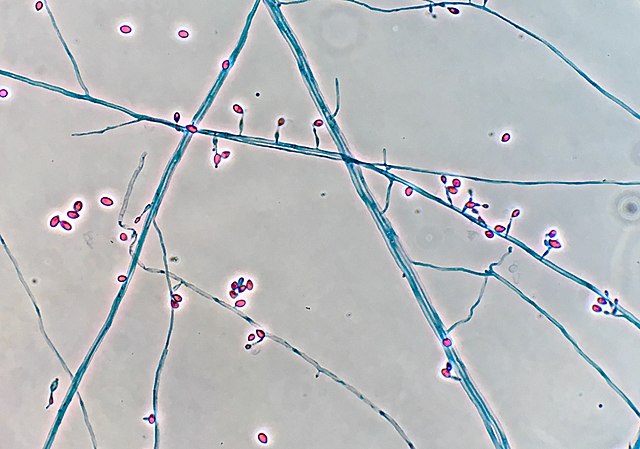
https://upload.wikimedia.org/wikipedia/commons/thumb/8/8e/Lomentospora_Family_Portrait.jpg/640px-Lomentospora_Family_Portrait.jpg
Phialemonium spp:
|
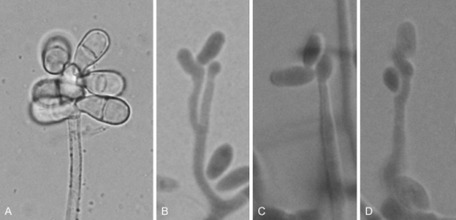
|
This species normally causes no harm, but can cause disseminated infections in patients who are immunocompromised. It has been associated with peritonitis, endocarditis, bone infections (osteomyelitis), wounds, and burns.
Sporothrix schenckii:
This fungus is not only a hyaline mold, but also one of the dimorphic molds. It causes sporotrichosis and can also cause keratomycosis of the eyes. Typically, infection results from a puncture wound with a thorn, such as a rose thorn, contaminated with the mold. Hay or wood punctures and splinters can also cause this. For this reason, it is often referred to as "rose gardener's disease".
Infection results in subcutaneous, hard, black, ulcerating lesions on the extremities, particularly the arm. Since they can travel along the lymphatic system, they may leave a track or track of these lesions as they progress. Rarely, it can become disseminated and spread, causing systemic infection.
In the USA, there have been several documented outbreaks of sporotrichosis associated with sphagnum moss in WI, which is often used in crafting or in gardening. Though granules are sometimes found, none were found in these cases.
Cutaneous infections can be treated with oral potassium iodide. Disseminated infection must be treated with amphotericin B and flucytosine.
Macroscopic Exam:
Microscopic Exam:
Infection results in subcutaneous, hard, black, ulcerating lesions on the extremities, particularly the arm. Since they can travel along the lymphatic system, they may leave a track or track of these lesions as they progress. Rarely, it can become disseminated and spread, causing systemic infection.
In the USA, there have been several documented outbreaks of sporotrichosis associated with sphagnum moss in WI, which is often used in crafting or in gardening. Though granules are sometimes found, none were found in these cases.
Cutaneous infections can be treated with oral potassium iodide. Disseminated infection must be treated with amphotericin B and flucytosine.
Macroscopic Exam:
- Because this is a dimorphic mold, conversion of the yeast form to the mold form is required for identification.
- On SABHI at room temperature, it grows a cream-colored, wrinkled, leathery, "wet" colony, which may blacken with age.
- In mold phase, the colony may resemble the glabrous form of Acremonium spp.
- In yeast phase at 37 degrees Celsius, colonies will be soft and white or cream-colored.
- Conversion: In order to convert the mold form to the yeast form, it should be subcultured from SABHI agar to brain heart infusion (BHI) agar with or without 10% blood, and incubated at 37 degrees Celsius in 5% CO2 for 3-5 days, keeping the medium moist.
Microscopic Exam:
- Yeast form: A wet mount will reveal elliptical-shaped budding yeasts in the yeast phase, and these are called "cigar bodies".
- Mold form: From mold cultures at room temperature, hyphae and conidia are observed, best stained in LPCB stain.
- Small, oval conidia will be seen singly along the hyphae or in flowerlike clusters, resembling "daisies", at the ends of short, unbranched conidiophores.
- Tiny hairlike structures connect the conidia to the conidiophore.

Sporothrix schenckii mold form single and daisy-like conidia
|

Sporothrix schenckii is associated with traumatic implantation via rose thorns or wood splinters and is known to cause "rose gardener's disease"
|
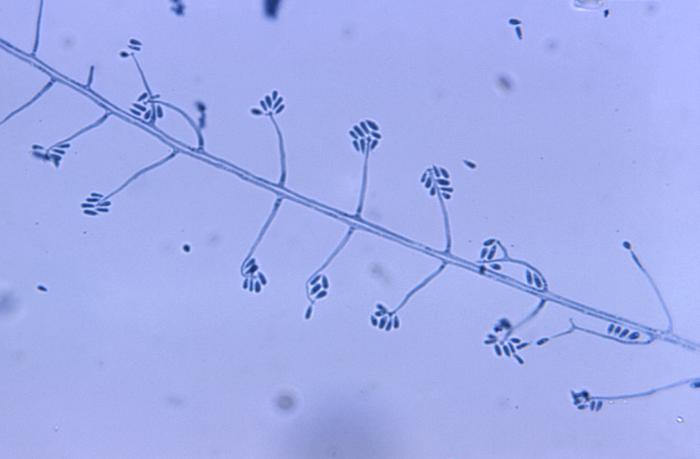
Mold phase "daisy head" conidia attached to conidiphores
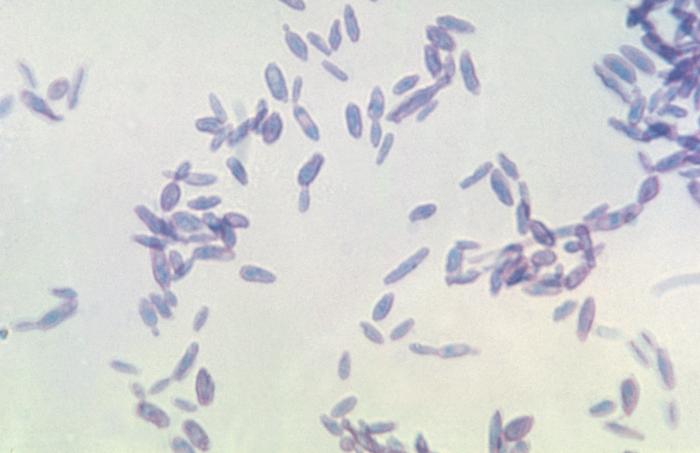
Yeast phase "cigar bodies"
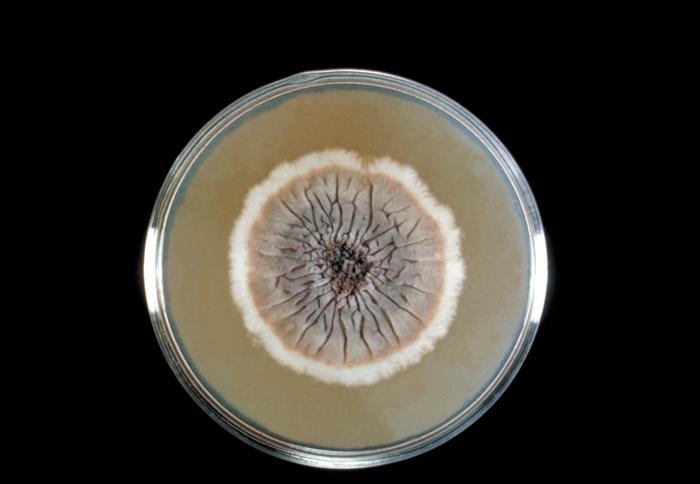
Sporothrix schenckii mold form
|

Sporothrix schenckii mold form (left) and yeast form (right)
|

Sporothrix schenckii yeast form.
Myceliophthora species:
Myceliphthora thermophila is typically not a pathogen, but it can cause rare, deep and systemic infection in those who are immunocompromised. It has been linked to infections in patients with myeloblastic leukemia. Other rare infections have occurred via direct inoculation into the body by garden or surgical tools that have been contaminated with the mold.
In environmental microbiology, this mold is being researched for its possibility for biofuels, since it breaks down cellulose, which makes up the cell walls of plants.
Macroscopic Exam:
In environmental microbiology, this mold is being researched for its possibility for biofuels, since it breaks down cellulose, which makes up the cell walls of plants.
Macroscopic Exam:
- On agar, it grows as a flat, powdery colony with cottony tufts, and is white with a cinnamon brown center.
- The reverse is cream.
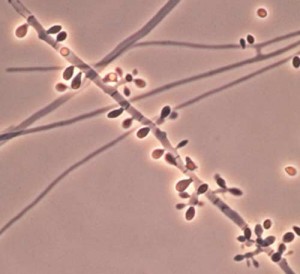
M. thermophila with large, racket-shaped aleuriospores.
Rhinocladiella species:
R. atrovirens:
- This is an environmental mold that is a rare cause of phaeohyphomycosis
- It grows as a flat or heaped, olive-green to dark grey floccose colony with a grey to black reverse
- This is an environmental mold that is a rare cause of cerebral phaeohyphomycosis, resulting in discolored CSF, headaches, psychosis, brain and spinal abscesses, particularly in immunocompromised patients, such as those with an underlying cancer like leukemia, and it can be fatal
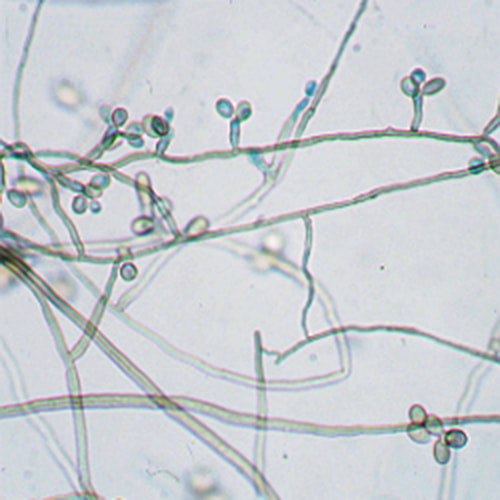
By Medmyco - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=61618702
ochroconis gallopava: *Now renamed to verruconis gallopava
This mold is an environmental mold but infections in the immunocompromised are on the rise with this organism. It is a rare cause of pulmonary, cerebral, and other forms of phaeohyphomycosis that can become disseminated in immunocompromised patients, particularly those who have had organ transplants or who have underlying hematological malignancies like leukemia or lymphoma. It has a predilection for the central nervous system (Larone, 2023). It can cause brain infection similar to encephalitis in humans.
Macroscopic Exam:
Microscopic Exam:
Macroscopic Exam:
- On agar, the mold grows as a flat, granular to velvety, dark red-brown or cinnamon colored colony with a reddish brown reverse (diffusible pigment).
Microscopic Exam:
- Microscopially, it produces hyaline or pale brown hyphae that are thick-walled and septate. Conidiophores are upright and sometimes bent or knobby at the point where the conidia form.
- Conidia are held by threadlike denticles and are brown, two-celled, and oval or teardrop-shaped with a marked constriction at the central septum (Larone, 2023).
Verruconis gallopava mold (a dark gray-black mold); Image by Jeanette Reynolds, M-ASCP, MLS-AMT, MS-Biology,
Microbiologist; This particular mold also formed dark cinnamon colonies on SAB slant agar and formed a dark red pigment that diffused into the agar
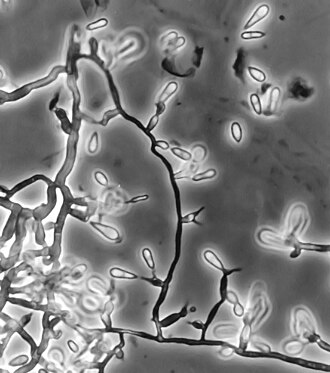
https://upload.wikimedia.org/wikipedia/commons/thumb/6/67/Ochroconis_gallopava.jpg/330px-Ochroconis_gallopava.jpg
yeasts:
Yeasts and yeastlike cells are unicellular organisms that reproduce by budding. The buds are referred to as "blastoconidia". Blastoconidia in some yeasts, such as Candida albicans, elongate but stay connected to the parent cell, forming "pseudohyphae". Other yeasts form "true hyphae" that are truly septate (contain cross-walls). Some don't form hyphae at all and are only observed as buds or spores.
Yeast colonies grow as smooth, waxy, glabrous, moist or dry, lacy/wrinkled colonies that tend to be cream, white or buff in color. Some may be pink, orange or tan in color as well. Some appear "fuzzy" due to the formation of "feet" or extensions that reach out to the agar to reach nutrients found in the agar. Yeasts grow very well on Cornmeal-Tween 80 agar, Sabouraud dextrose agar, BHI with blood, some grow on Mycosel with cycloheximide, ChromAGAR, and they grow well at 25-35 degrees Celsius, or body temperature.
In the clinical laboratory, yeasts are the most common fungi isolated because they are ubiquitous and found everywhere in the environment. Yeasts that truly cause infection are considered opportunistists, causing illness in persons who are immunocompromised, immunosuppressed, or who have otherwise underlying illnesses that lead to a breakdown in the body's normal immune response. Prolonged antibiotic therapy, heavy antibiotic dosage therapy, corticosteroid treatment, cytotoxic drug administration, IV catheters, and those with diabetes mellitus are at higher risk for opportunistic infections.
Invasive candidiasis infections are associated with 30% mortality! The most common yeasts seen in the clinical setting include: Candida albicans, C. glabrata, C. parapsilosis, C. tropicalis, and C. krusei (CDC, 2024). Species distribution varies by patient population and geographic region. One of the biggest concerns is growing antifungal-resistance, spread, and potential outbreaks. In 2019, a new pathogenic yeast was discovered: C. auris. It has shown 90% resistance to fluconazole, 30% resistance to amphotericin B, and 5% resistance to the echinocandins (CDC, 2024). For this reason, some hospitals screen for surveillance of this particular organism.
Yeast colonies grow as smooth, waxy, glabrous, moist or dry, lacy/wrinkled colonies that tend to be cream, white or buff in color. Some may be pink, orange or tan in color as well. Some appear "fuzzy" due to the formation of "feet" or extensions that reach out to the agar to reach nutrients found in the agar. Yeasts grow very well on Cornmeal-Tween 80 agar, Sabouraud dextrose agar, BHI with blood, some grow on Mycosel with cycloheximide, ChromAGAR, and they grow well at 25-35 degrees Celsius, or body temperature.
In the clinical laboratory, yeasts are the most common fungi isolated because they are ubiquitous and found everywhere in the environment. Yeasts that truly cause infection are considered opportunistists, causing illness in persons who are immunocompromised, immunosuppressed, or who have otherwise underlying illnesses that lead to a breakdown in the body's normal immune response. Prolonged antibiotic therapy, heavy antibiotic dosage therapy, corticosteroid treatment, cytotoxic drug administration, IV catheters, and those with diabetes mellitus are at higher risk for opportunistic infections.
Invasive candidiasis infections are associated with 30% mortality! The most common yeasts seen in the clinical setting include: Candida albicans, C. glabrata, C. parapsilosis, C. tropicalis, and C. krusei (CDC, 2024). Species distribution varies by patient population and geographic region. One of the biggest concerns is growing antifungal-resistance, spread, and potential outbreaks. In 2019, a new pathogenic yeast was discovered: C. auris. It has shown 90% resistance to fluconazole, 30% resistance to amphotericin B, and 5% resistance to the echinocandins (CDC, 2024). For this reason, some hospitals screen for surveillance of this particular organism.
Candida spp:
Candida albicans:
This is the most common cause of candidiasis. Candidiasis may cause infection in any part of the body, including sterile sites such as the blood or CSF, which may be acute, subacute or chronic. Infection may be local or systemic. Candida albicans is also part of the normal commensal flora on the skin, and in the mouth, stool, and vaginal mucosa. Overgrowth may result in opportunistic infection. Common infections include:
Candida krusei: In addition to the infections above, this organism can cause deep-seated or bloodstream infections (candidemia) in susceptible individuals who are immunocompromised or have an underlying illness. This species is resistant to fluconazole.
Candida parapsilosis: This species is linked to infections in susceptible persons who are immunocompromised or have underlying illness and frequently causes candida-associated endocarditis. Neonates, critical care patients, those with indwelling catheters or tubing for parenteral nutrition are at risk for infection.
Candida pseudotropicalis: Also called C. kefyr, this species is usually considered a nonpathogen. Rarely, it has been linked to infection in the immunocompromised.
Candida pelliculosa: This yeast only occasionally causes infection in susceptible patients. It is usually found in the soil as a saprobe. It produces cream-colored, smooth, moist colonies in 5 days.
Candida rugosa complex: This species is a complex that was originally isolated from cattle, where it is one of the primary causes of mastitis, as well as from turkeys, which can kill them if it gets into their digestive tracts. Now, it is considered to be one of the emerging pathogenic fungi in humans. Not only has it been reported in humans, but it has also been reported as linked to outbreaks, particularly of cather-associated infections (Larone, 2023). It has also been linked to urinary tract infections in hospitals, trauma and burn centers (Larone, 2023).
Candida tropicalis: This species is linked to invasive infection, particularly in immunocompromised patients such as those with underlying hematological malignancies or stem cell transplant patients. It can also cause bloodstream infections.
Candida lusitaniae: This species is a causative agent of opportunistic infection in immunocompromised patients, especially those with underlying malignancies or serious conditions, and has shown some antifungal resistance. It is of low virulence. Colonies are white to cream, glistening and smooth.
Candida glabrata: This species is an opportunistic pathogen of the urogenital tract and of the bloodstream, particularly in patients who are HIV positive or who are elderly. Because it forms biofilms on urinary catheters and IV catheters and dentures, patients with indwelling catheters or elderly with dentures are at risk for fungal infection by this organism. It has been associated with nosocomial infections (hospital-acquired), arthritis, endocarditis, disseminated infections, pulmonary infections, vaginitis, urinary tract infections, oral infections, and esophagitis. Since antifungal resistance is on the rise, this organism is being studied for its growing resistance, particularly to the chinocandins and fluconazole and other azoles.
This yeast is germ tube negative, and it is a budding yeast with small budding cells that do not form pseudohyphae in the wet mount or on cornmeal agar.
Candida guilliermondii complex: This yeast complex is usually a nonpathogen, linked only occasionally to infection in the immunocompromised, which can be superficial or deep-seated. According to Larone, it has been linked to endocarditis, osteomyelitis, cutaneous infections and urinary tract infections, and occasional systemic disease (Larone, 2023). It is linked to sporadic cases of nosocomial infections, since it may be carried on the hands of healthcare workers. Growth is rapid, maturing in 3 days, with flat, glossy, smooth, cream-colored colonies that pinken with age. Microscopically, it appears as small cells and a few short pseudohyphae with small clusters of blastoconidia at the septa. The germ tube test is negative.
Candida haemulonii complex: This species complex is becoming a more and more recognized cause of fungemia and it is also linked to deeply invasive candidiasis. It is showing high levels of resistance to fluconazole and amphotericin B. It grows fast, and in 5 days, produces mature colonies that WILL grow on Mycosel agar. Colonies are white or cream in color, smooth, and glabrous. On CHROMagar, colonies are pink at 24 hours and violet at 72 hours. On Cornmeal Agar, this yeast produces budding yeast cells that are oval, and it does not produce true hyphae, and only rarely produces pseudohyphae.
Candida lipolytica: This yeast is an opportunistic pathogen that may rarely infect the immunocompromised. It grows rapidly, maturing within 6 days, and produces colonies that are cream-colored and raised, dull and smooth-to-wrinkled. Microscopically, it is observed as pseudohyphae and true hyphae (septate) that bear elongated blastoconidia in short chains. They look like tree branches. Arthroconidia may be present as well. The germ tube test is negative. It is urease positive.
Candida dubliniensis: This yeast is an opportunistic pathogen that typically infects those who are immunocompromised, such as those with HIV/AIDS, underlying malignancies, undergoing chemotherapy, insulin-dependent diabetics, or individuals who have had an organ transplant. Occasionally, it has been isolated from the immunocompetent as well, however. It has been linked to oral thrush, respiratory, urine, and even GI infections. Some strains are resistant to fluconazole, but many are susceptible to that and closely related antifungals.
Candida zylanoides: This yeast is rarely reported as a cuase of fungemia, but rare causes have been linked to arthrits, skin and nail infections. It grows in 5 days and produces colonies that are cream or yellow in collor, dull, and smooth. On Cornmeal Agar, it is beautiful and dainty with pseudohyphae consisting of curved cells or blastoconidia that are elongated both singly and in small clusters and in short chains. It is "featherlike".
Candida auris: This yeast is of extreme concern because of the new pathogen and its jump in cases in the USA and growing resistance to common antifungals. This organism spreads easily, especially in healthcare settings. It can cause severe illness, particularly in those who are immunocompromised. It can cause bloodstream infections, wound infections, and stubborn ear infections. It has also been associated with outbreaks. It was first isolated from the external ear canal of an individual in Japan in 2009, and has since spread globally as an aemerging multidrug-resistant pathogen (Larone, 2023). This yeast not only causes candidemia, but it can deeply invade the tissues, causing candidiasis. Not only that, it can form biofilms, leading to its persistance and difficulty to completely get rid of. It can also colonize the human body and skin, causing an invasive opportunistic infection if the conditions are just right. It has shown resistance to fluconazole and some resistance to amphotericin B, and even to echinocandins. Infection control and prevention methods, including surveillance and screening, close monitoring, reporting, and tracking of colonized cases and active infections is key to prevent healthcare-associated infections.
Unfortunately, since it can also colonize the skin of some people, resulting in no symptoms, but they can be carriers and pass it on to others who may get sick, or it can put them at higher risk for an opportunistic infection during surgery or if they get sick with something else. The term "colonization" means that a person can still transmit the yeast directly to others through direct contact, or transmit it to surfaces through indirect contact. Most of the time, however, it is not a threat to otherwise healthy individuals.
The colonies grow and mature within 5 days and can pretty much grow at any temperature ranging from 25 to 42 degrees Celsius, which differentiates them from the other yeasts. They will NOT grow on Mycosel agar, because cycloheximide inibits growth. The colonies will appear as cream in color and smooth on SAB dextrose agar. On CHROMagar, colonies will be pink or purple in color, darkening to red with extended incubation time. This is considered to be a preliminary screening.
In nutrient broth, the yeast produces small, oval, budding yeasts, some of which are elongated and ellipsoid in shape. They range from 2-3 to 2.5.5 micrometers in size, and are found singlyin pairs, or in small clusters. They typically do not form pseudohyphae or hyphae. The results should always be confirmed with MALDI-TOF MS or by DNA sequencing (PCR).
There are two ways to test for this organism:
If a colonization screening or culture comes back positive for this organism, if the individual is in the hospital inpatient setting, contact precautions should be put into place. Healthcare providers and family members who are visiting the individual should wash their hands or use alcohol-based hand sanitizer prior to entering the patient's room, AND before they leave the room, to prevent it from spreading to other patients. Medical devices need to be thoroughly cleaned between patients as well. Gowns and gloves need to be worn when providing care, and when cleaning the room. Special cleaners should be used to clean the room after the patient is discharged from the hospital.
According to the CDC, "a total of 3270 clinical cases and 7413 screening cases of C auris were reported in the United States through 31 December 2021. The percentage increase in clinical cases grew each year, from a 44% increase in 2019 to a 95% increase in 2021. Colonization screening volume and screening cases increased in 2021 by more than 80% and more than 200%, respectively. From 2019 to 2021, 17 states identified their first C auris case. The number of C auris cases that were resistant to echinocandins in 2021 was about 3 times that in each of the previous 2 years. " (CDC, 2024) For this reason, this is a reportable organism to your county and state health departments.
Who is at risk for infection? Patients who are on ventilators, breathing tubes, feeding tubes, IV catheters, or urinary catheters are at higher risk for infection. Only those with an infection should be treated with antifungals. Antifungal susceptibility testing should be performed on the isolate, to see which antifungals it is susceptible to for treatment of the patient. So far, about 90% of isolates have shown resistance to fluconazole, 30% have shown resistance to amphotericin B, and 5% are resistant to echinocandins (class of antifungals) (CDC, 2024).
Candida albicans:
This is the most common cause of candidiasis. Candidiasis may cause infection in any part of the body, including sterile sites such as the blood or CSF, which may be acute, subacute or chronic. Infection may be local or systemic. Candida albicans is also part of the normal commensal flora on the skin, and in the mouth, stool, and vaginal mucosa. Overgrowth may result in opportunistic infection. Common infections include:
- Vaginosis
- UTI
- Wound
- Nail
- Thrush
- Esophagitis
Candida krusei: In addition to the infections above, this organism can cause deep-seated or bloodstream infections (candidemia) in susceptible individuals who are immunocompromised or have an underlying illness. This species is resistant to fluconazole.
Candida parapsilosis: This species is linked to infections in susceptible persons who are immunocompromised or have underlying illness and frequently causes candida-associated endocarditis. Neonates, critical care patients, those with indwelling catheters or tubing for parenteral nutrition are at risk for infection.
Candida pseudotropicalis: Also called C. kefyr, this species is usually considered a nonpathogen. Rarely, it has been linked to infection in the immunocompromised.
Candida pelliculosa: This yeast only occasionally causes infection in susceptible patients. It is usually found in the soil as a saprobe. It produces cream-colored, smooth, moist colonies in 5 days.
Candida rugosa complex: This species is a complex that was originally isolated from cattle, where it is one of the primary causes of mastitis, as well as from turkeys, which can kill them if it gets into their digestive tracts. Now, it is considered to be one of the emerging pathogenic fungi in humans. Not only has it been reported in humans, but it has also been reported as linked to outbreaks, particularly of cather-associated infections (Larone, 2023). It has also been linked to urinary tract infections in hospitals, trauma and burn centers (Larone, 2023).
Candida tropicalis: This species is linked to invasive infection, particularly in immunocompromised patients such as those with underlying hematological malignancies or stem cell transplant patients. It can also cause bloodstream infections.
Candida lusitaniae: This species is a causative agent of opportunistic infection in immunocompromised patients, especially those with underlying malignancies or serious conditions, and has shown some antifungal resistance. It is of low virulence. Colonies are white to cream, glistening and smooth.
Candida glabrata: This species is an opportunistic pathogen of the urogenital tract and of the bloodstream, particularly in patients who are HIV positive or who are elderly. Because it forms biofilms on urinary catheters and IV catheters and dentures, patients with indwelling catheters or elderly with dentures are at risk for fungal infection by this organism. It has been associated with nosocomial infections (hospital-acquired), arthritis, endocarditis, disseminated infections, pulmonary infections, vaginitis, urinary tract infections, oral infections, and esophagitis. Since antifungal resistance is on the rise, this organism is being studied for its growing resistance, particularly to the chinocandins and fluconazole and other azoles.
This yeast is germ tube negative, and it is a budding yeast with small budding cells that do not form pseudohyphae in the wet mount or on cornmeal agar.
Candida guilliermondii complex: This yeast complex is usually a nonpathogen, linked only occasionally to infection in the immunocompromised, which can be superficial or deep-seated. According to Larone, it has been linked to endocarditis, osteomyelitis, cutaneous infections and urinary tract infections, and occasional systemic disease (Larone, 2023). It is linked to sporadic cases of nosocomial infections, since it may be carried on the hands of healthcare workers. Growth is rapid, maturing in 3 days, with flat, glossy, smooth, cream-colored colonies that pinken with age. Microscopically, it appears as small cells and a few short pseudohyphae with small clusters of blastoconidia at the septa. The germ tube test is negative.
Candida haemulonii complex: This species complex is becoming a more and more recognized cause of fungemia and it is also linked to deeply invasive candidiasis. It is showing high levels of resistance to fluconazole and amphotericin B. It grows fast, and in 5 days, produces mature colonies that WILL grow on Mycosel agar. Colonies are white or cream in color, smooth, and glabrous. On CHROMagar, colonies are pink at 24 hours and violet at 72 hours. On Cornmeal Agar, this yeast produces budding yeast cells that are oval, and it does not produce true hyphae, and only rarely produces pseudohyphae.
Candida lipolytica: This yeast is an opportunistic pathogen that may rarely infect the immunocompromised. It grows rapidly, maturing within 6 days, and produces colonies that are cream-colored and raised, dull and smooth-to-wrinkled. Microscopically, it is observed as pseudohyphae and true hyphae (septate) that bear elongated blastoconidia in short chains. They look like tree branches. Arthroconidia may be present as well. The germ tube test is negative. It is urease positive.
Candida dubliniensis: This yeast is an opportunistic pathogen that typically infects those who are immunocompromised, such as those with HIV/AIDS, underlying malignancies, undergoing chemotherapy, insulin-dependent diabetics, or individuals who have had an organ transplant. Occasionally, it has been isolated from the immunocompetent as well, however. It has been linked to oral thrush, respiratory, urine, and even GI infections. Some strains are resistant to fluconazole, but many are susceptible to that and closely related antifungals.
Candida zylanoides: This yeast is rarely reported as a cuase of fungemia, but rare causes have been linked to arthrits, skin and nail infections. It grows in 5 days and produces colonies that are cream or yellow in collor, dull, and smooth. On Cornmeal Agar, it is beautiful and dainty with pseudohyphae consisting of curved cells or blastoconidia that are elongated both singly and in small clusters and in short chains. It is "featherlike".
Candida auris: This yeast is of extreme concern because of the new pathogen and its jump in cases in the USA and growing resistance to common antifungals. This organism spreads easily, especially in healthcare settings. It can cause severe illness, particularly in those who are immunocompromised. It can cause bloodstream infections, wound infections, and stubborn ear infections. It has also been associated with outbreaks. It was first isolated from the external ear canal of an individual in Japan in 2009, and has since spread globally as an aemerging multidrug-resistant pathogen (Larone, 2023). This yeast not only causes candidemia, but it can deeply invade the tissues, causing candidiasis. Not only that, it can form biofilms, leading to its persistance and difficulty to completely get rid of. It can also colonize the human body and skin, causing an invasive opportunistic infection if the conditions are just right. It has shown resistance to fluconazole and some resistance to amphotericin B, and even to echinocandins. Infection control and prevention methods, including surveillance and screening, close monitoring, reporting, and tracking of colonized cases and active infections is key to prevent healthcare-associated infections.
Unfortunately, since it can also colonize the skin of some people, resulting in no symptoms, but they can be carriers and pass it on to others who may get sick, or it can put them at higher risk for an opportunistic infection during surgery or if they get sick with something else. The term "colonization" means that a person can still transmit the yeast directly to others through direct contact, or transmit it to surfaces through indirect contact. Most of the time, however, it is not a threat to otherwise healthy individuals.
The colonies grow and mature within 5 days and can pretty much grow at any temperature ranging from 25 to 42 degrees Celsius, which differentiates them from the other yeasts. They will NOT grow on Mycosel agar, because cycloheximide inibits growth. The colonies will appear as cream in color and smooth on SAB dextrose agar. On CHROMagar, colonies will be pink or purple in color, darkening to red with extended incubation time. This is considered to be a preliminary screening.
In nutrient broth, the yeast produces small, oval, budding yeasts, some of which are elongated and ellipsoid in shape. They range from 2-3 to 2.5.5 micrometers in size, and are found singlyin pairs, or in small clusters. They typically do not form pseudohyphae or hyphae. The results should always be confirmed with MALDI-TOF MS or by DNA sequencing (PCR).
There are two ways to test for this organism:
- "Colonization screening– a healthcare provider swabs the patient’s skin by rubbing a swab near the armpits and groin and sends the swab to a laboratory for testing.
- Clinical specimen testing– If a patient is showing symptoms of an infection of unknown cause, a healthcare provider may collect a clinical sample, like blood or urine. They usually test for many types of infections including those caused by bacteria and the results may show that the patient has C. auris." (CDC, 2024)
If a colonization screening or culture comes back positive for this organism, if the individual is in the hospital inpatient setting, contact precautions should be put into place. Healthcare providers and family members who are visiting the individual should wash their hands or use alcohol-based hand sanitizer prior to entering the patient's room, AND before they leave the room, to prevent it from spreading to other patients. Medical devices need to be thoroughly cleaned between patients as well. Gowns and gloves need to be worn when providing care, and when cleaning the room. Special cleaners should be used to clean the room after the patient is discharged from the hospital.
According to the CDC, "a total of 3270 clinical cases and 7413 screening cases of C auris were reported in the United States through 31 December 2021. The percentage increase in clinical cases grew each year, from a 44% increase in 2019 to a 95% increase in 2021. Colonization screening volume and screening cases increased in 2021 by more than 80% and more than 200%, respectively. From 2019 to 2021, 17 states identified their first C auris case. The number of C auris cases that were resistant to echinocandins in 2021 was about 3 times that in each of the previous 2 years. " (CDC, 2024) For this reason, this is a reportable organism to your county and state health departments.
Who is at risk for infection? Patients who are on ventilators, breathing tubes, feeding tubes, IV catheters, or urinary catheters are at higher risk for infection. Only those with an infection should be treated with antifungals. Antifungal susceptibility testing should be performed on the isolate, to see which antifungals it is susceptible to for treatment of the patient. So far, about 90% of isolates have shown resistance to fluconazole, 30% have shown resistance to amphotericin B, and 5% are resistant to echinocandins (class of antifungals) (CDC, 2024).
|
|
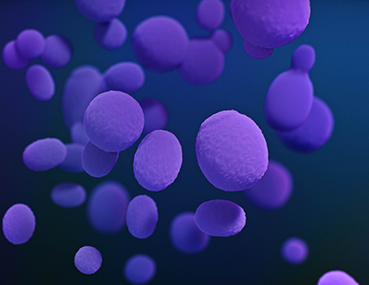
|

https://www.cdc.gov/fungal/candida-auris/images/test-tube-swab-250px.jpg
|

https://www.cdc.gov/fungal/candida-auris/images/colonization-hospital-bed-300px.jpg
|

https://www.cdc.gov/fungal/candida-auris/images/lab-test-small.jpg?_=09928
|

https://www.cdc.gov/fungal/candida-auris/images/hand_washing_b250px.jpg
|
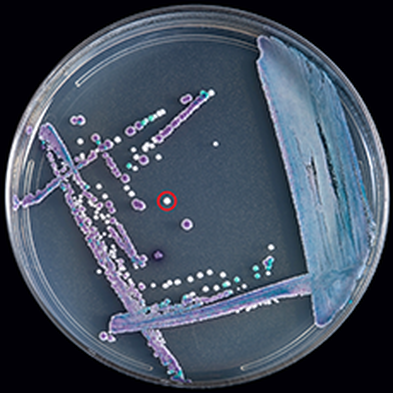
On this ChromAGAR plate, there are several different yeast colony types, and this is common. The one that is circled (white) is the C. auris colony. https://www.cdc.gov/fungal/candida-auris/images/Artificially-mixed-plate-230px.png?_=43634
|

On this type of ChromAGAR plate, there are several color variations of C. auris, but they are all the same organism. https://www.cdc.gov/fungal/candida-auris/images/grown-in-broth-4-days-230px.png?_=43633
|
Candida Albicans:
C. albicans grows well at 30 degrees Celsius on glucose peptone agar, producing white-to-cream, glistening, smooth, sometimes dull, rough colonies with or without a filamentous margin. On cornmeal agar, the yeast produces true hyphae, pseudohyphae, and chlamydospores. It also produces blastospores formed in clusters at intervals along the length of the hyphae and chlamydophores at the ends, giving it a "lollipop" appearance on Cornmeal agar. See the 2 images below for examples of Cornmeal agar observation under the microscope. Other characteristics include:
- Inability to ferment sucrose
- Positive germ tube test within 2-3 hours
- Fewer chlamydospores than C. dubliniensis
- Grows at 45 degrees Celsius
- Produces B-glucosidase
identification of yeasts:
According to the CDC, verification of the initial screening tests performed on isolates on plates like cornmeal agar or ChromAGAR should be performed for confirmation prior to releasing final results. What is highly recommended is matrix-assisted laser desorption ionization time of flight (MALDI-TOF) since it is one of the simplest and most accurate methodologies for identifying yeasts. Many laboratories are using this method because it is so quick and easy and saves hours-to-days of time. It is best to perform this method from the SAB dextrose subculture plate, but you can also perform this method from the original SAB plate. It is best to subculture different colony appearances, because plates can have 2-3 different types of yeast growing on them. If you have a plate growing 1, 2 or even 3 different looking colonies, test them all. MALDI-TOF will ID all of them.
When you perform a wet mount or look at a cornmeal agar under the microscope, C. auris, like C. glabrata, is a budding yeast only. It does not form pseudohyphae. In the germ tube test, it does not form germ tubes, so this test will be negative. Some strains form aggregates of cells, but others do not. C. auris grows best at 40-42 degrees Celsius. On ChromAGAR, C. auris will range from white to pink to purple to red.
It is best to fill in two circles at a time for the best chance of identification the first time. Use the pen or small loop to smear the colony in the target well of the stainless steel plate. Cover with 0.5 microliters of CHCA matrix first, allowing it to completely air dry. Cover with 1.0 microliters of 70% formic acid and allow to completely air dry prior to running this on the MALDI-TOF.
Other methods of effective ID include: real-time PCR, Biofire microfilm array PCR, Vitek, Microscan, Phoenix ID yeast cards (not as accurate as MALDI-TOF or PCR). API and RapID biochemical rapid tests can also be used, but be aware that these methods can misidentify C. auris since others are similar. https://www.cdc.gov/fungal/candida-auris/identification.html
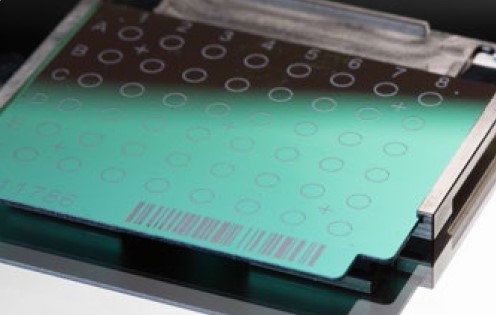
https://www.cdc.gov/fungal/lab-professionals/images/maldi-target-plate.jpg?_=94654
yeast cultures, wet mounts, cornmeal and chromagar screenings:
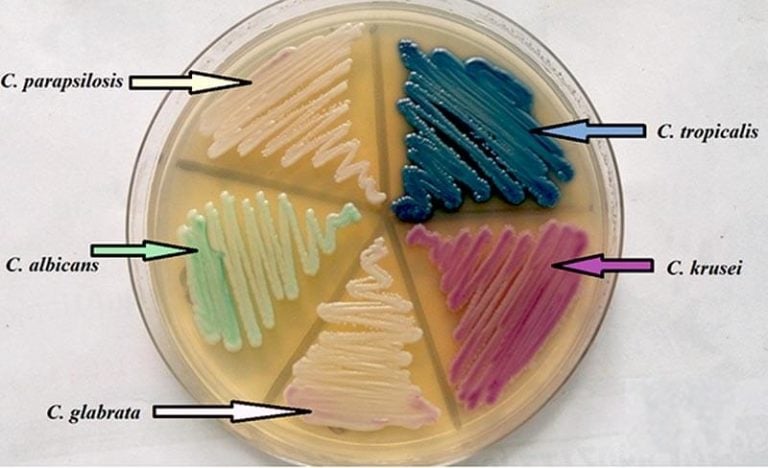
https://external-content.duckduckgo.com/iu/?u=https%3A%2F%2Fmicrobenotes.com%2Fwp-content%2Fuploads%2F2020%2F05%2FLaboratory-Diagnosis-of-Candida-glabrata-768x468.jpg&f=1&nofb=1&ipt=c98d33e6894e7ca89befcfc0315ff9ca83a5f1dcda294428d68ad76d1c4a0923&ipo=images
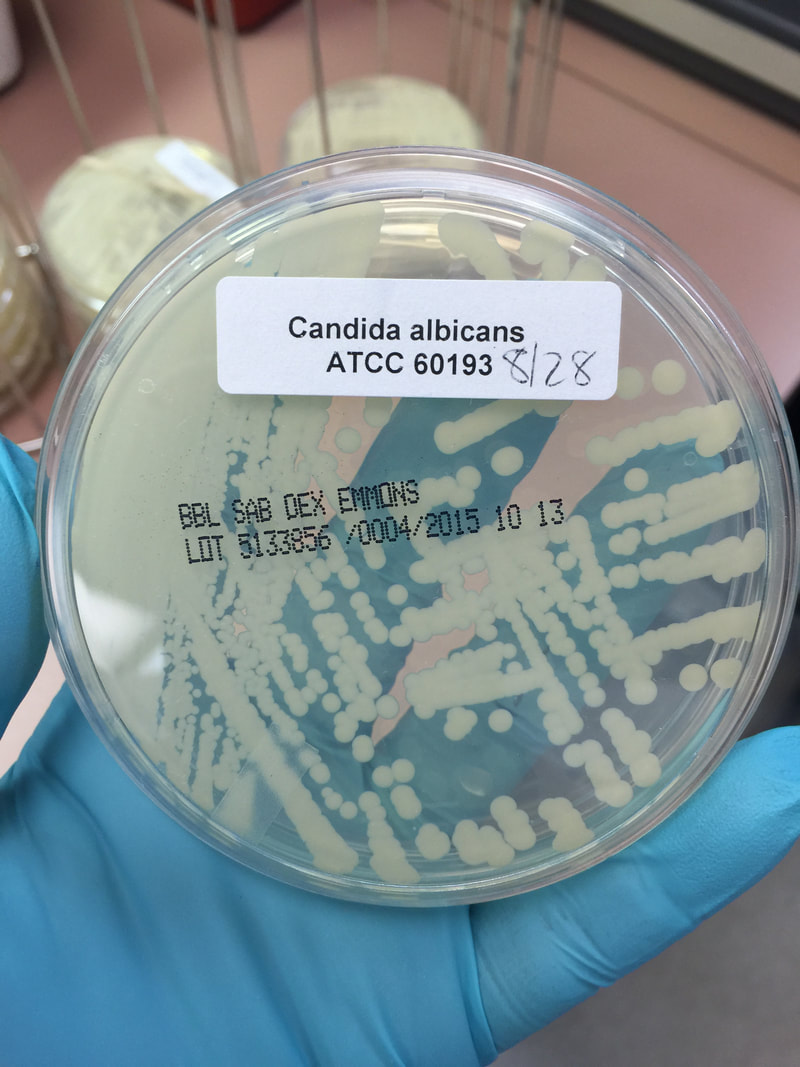
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
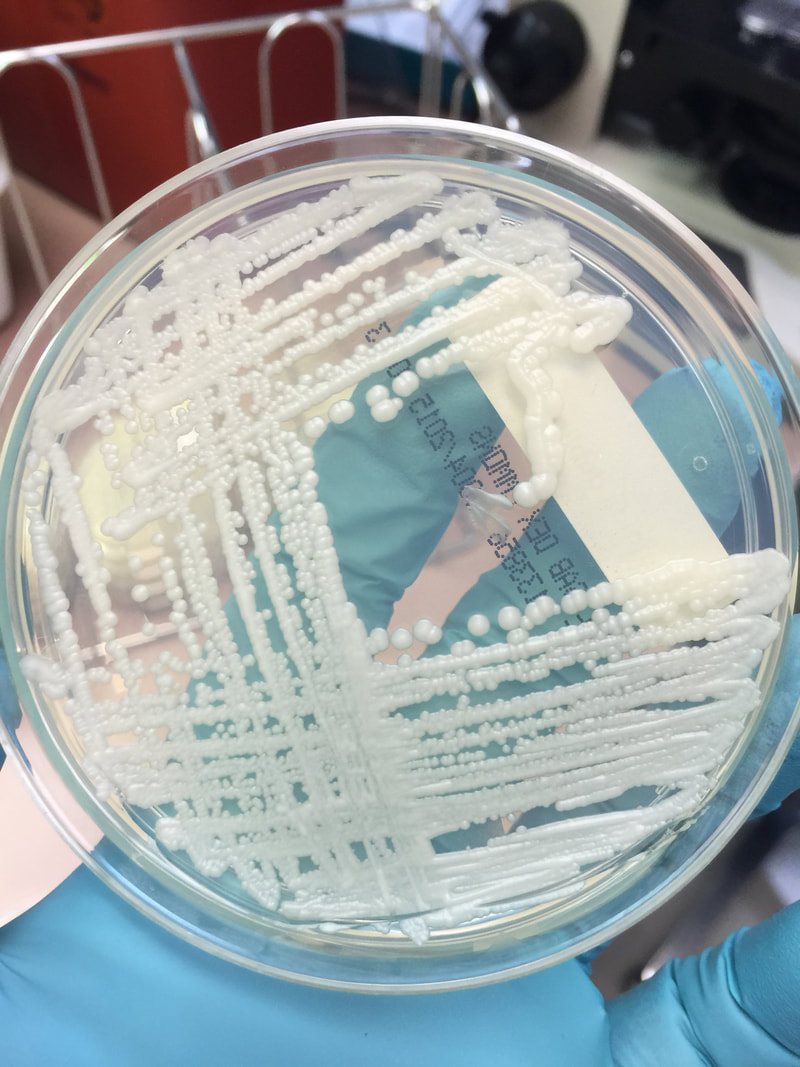
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
This strain is cream or off-white, glabrous, and pearly.
|
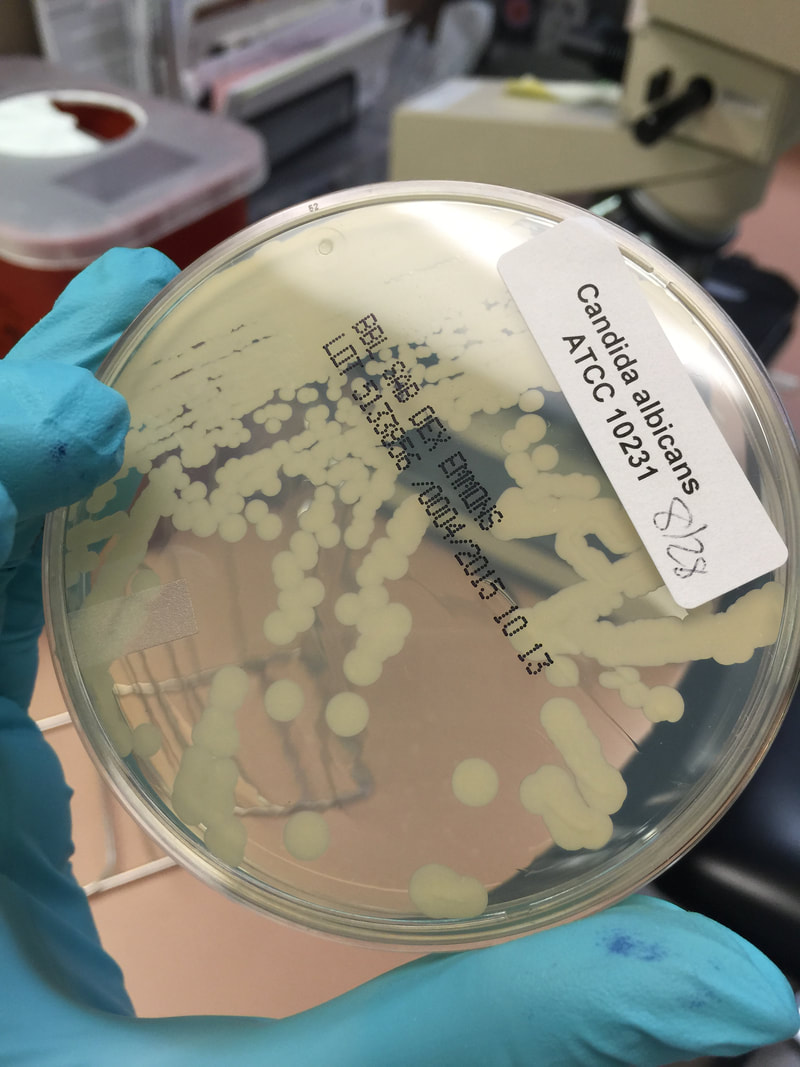
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
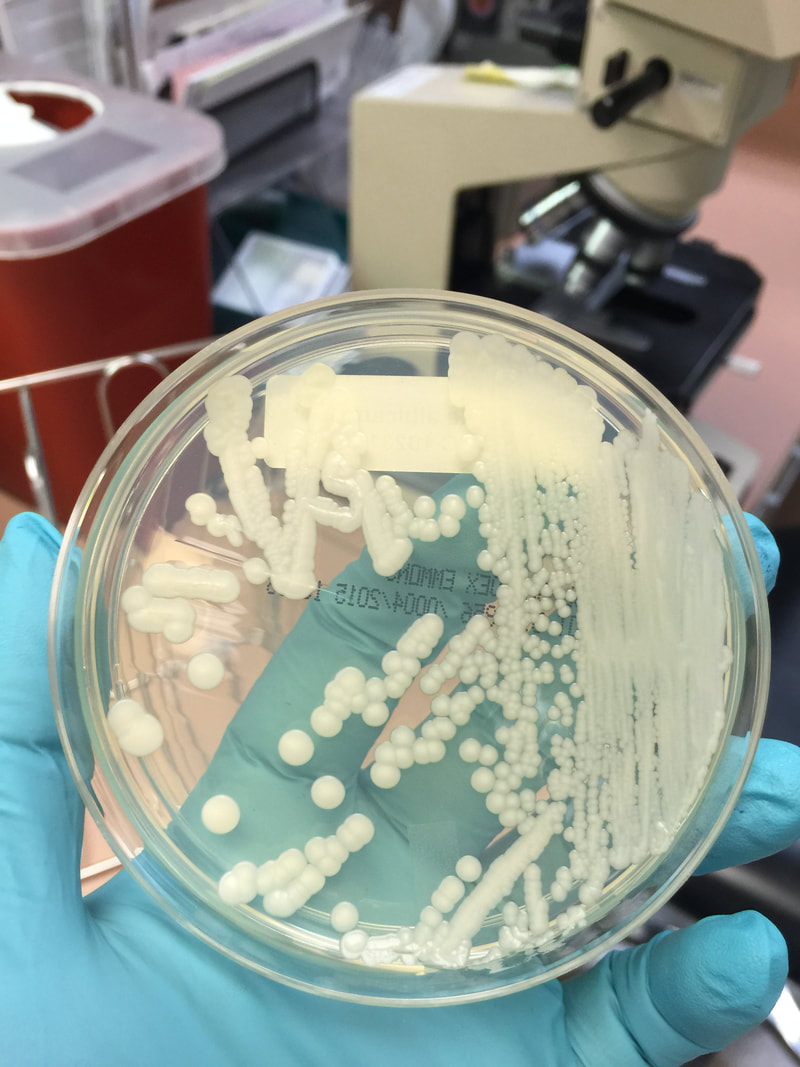
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
This strain is umbonate, larger, cream-colored and shiny.
|
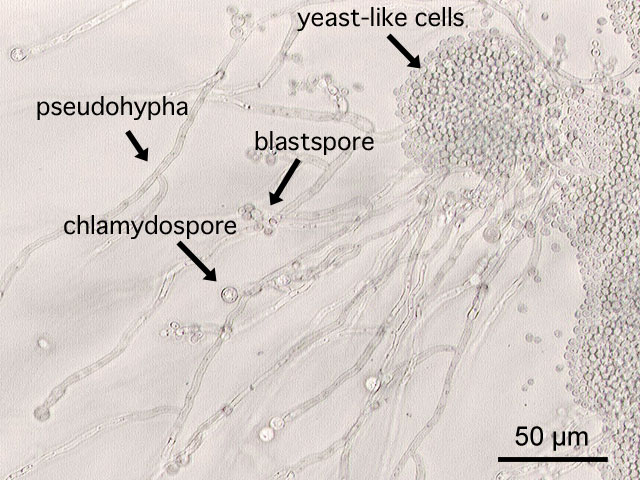
C. albicans on Cornmeal Agar: At 25 degrees Celsius at 72 hours, microscopically, C. albicans may be observed with pseudohyphae, clusters of blastoconidia (spherical/round), large, round, thick-walled chlamydospores
|

Terminal chlamydospores seen here, and in C. albicans only, they resemble "lollipops" because they are large, circular, and at the ends. Terminal chlamydospores are inhibited at 30-37 degrees Celsius; Cornmeal Agar
|
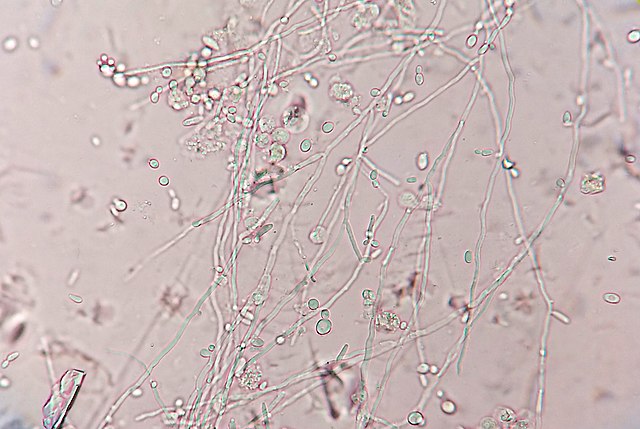
https://upload.wikimedia.org/wikipedia/commons/thumb/6/66/Candida_with_pseudohyphae.jpg/640px-Candida_with_pseudohyphae.jpg
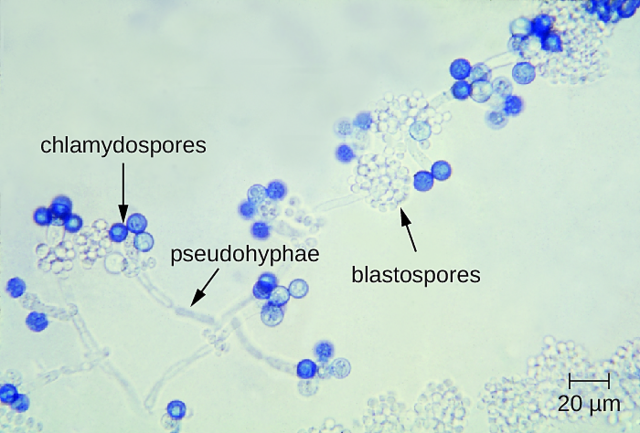
https://upload.wikimedia.org/wikipedia/commons/thumb/d/df/Candida_pseudohyphae%2C_chlamydospores%2C_blastospores.png/640px-Candida_pseudohyphae%2C_chlamydospores%2C_blastospores.png
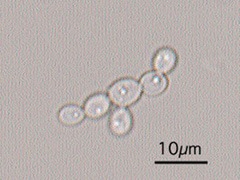
Budding yeast cells: Blastoconidia
|
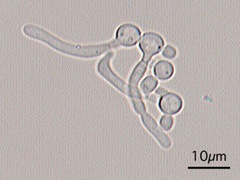
Germ Tube Test: C. albicans gives a positive germ tube test
|
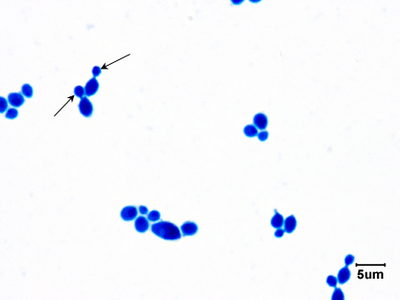
Budding (methylene blue)
|
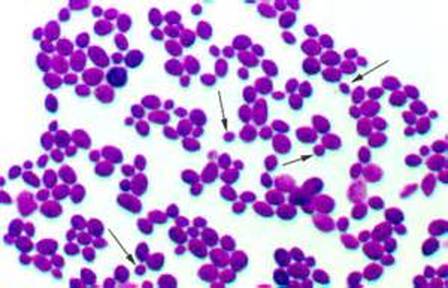
Budding (Gram stain)
|
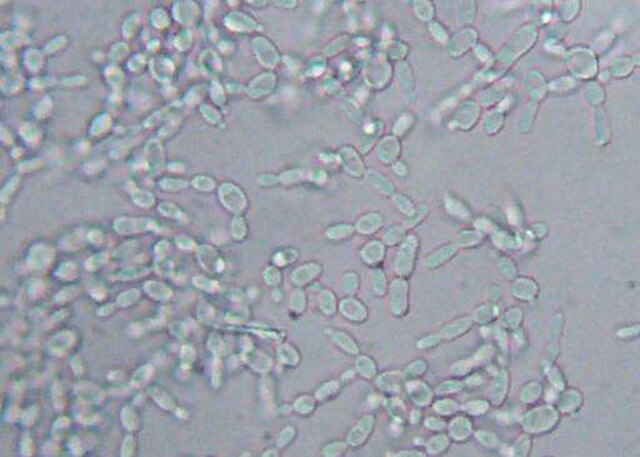
https://upload.wikimedia.org/wikipedia/commons/thumb/1/11/Candida_wet_mount.jpg/640px-Candida_wet_mount.jpg

The waxy, mucoid, glabrous, creamy colonies produced by C. albicans on SAB agar; Photo by Jeanette Reynolds, MS-Biology, MT-AMT, M-ASCP
|

C. albicans is a very rapid grower, maturing in just 3 days and forming creamy, cream-colored, pasty, smooth, waxy colonies on SAB or Cornmeal-Tween 80 agars. As these colonies age, you can also see the spiderweb-like "feet" spreading from the colonies into the agar.
|
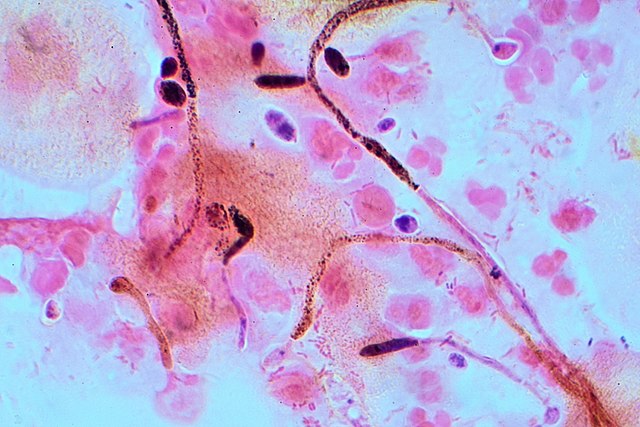
This is a Gram-stained vaginal swab positive for C. albicans. https://upload.wikimedia.org/wikipedia/commons/thumb/e/e6/Candida_Gram_stain.jpg/640px-Candida_Gram_stain.jpg
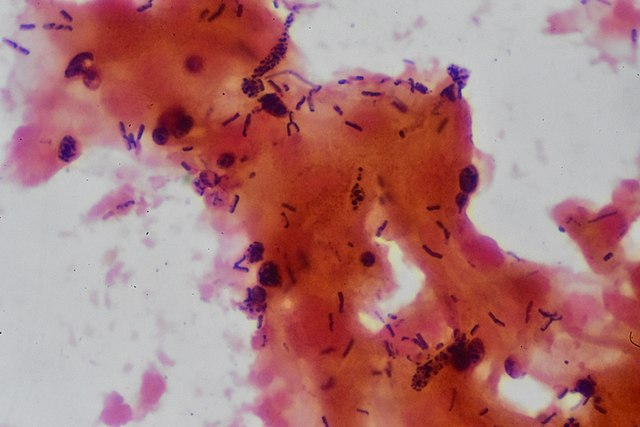
https://upload.wikimedia.org/wikipedia/commons/thumb/9/93/Candida_spores_and_pseudohyphae.jpg/640px-Candida_spores_and_pseudohyphae.jpg
Candida krusei:
C. krusei produces white or gray colonies on glucose peptone agar, which are flat, dull and smooth. On Cornmeal agar, the yeast produces abundant pseudohyphae and few ellipsoidal or cylindrical blastospores, giving it a "matchstick" appearance.

Candida kruseii matures quickly in 3 days and grows as flat, dull, dry colonies, cream-colored with a fringe. It grows on Cornmeal-Tween 80 agar at 25 degrees Celsius. Microscopically, long pseudohyphae form, which bear elongated blastoconidia. They look like "matchsticks" or "trees". The germ tube test is negative.
|
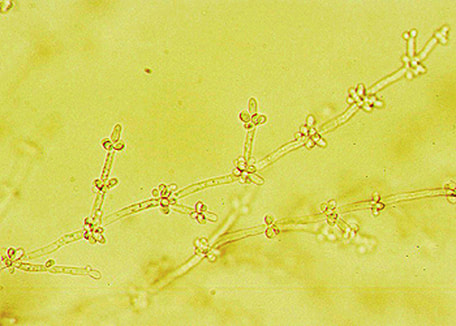
C. kruseii on Cornmeal Agar
|

Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
C. krusei colonies tend to be small, dry, umbonate, and sometimes lacy.
|
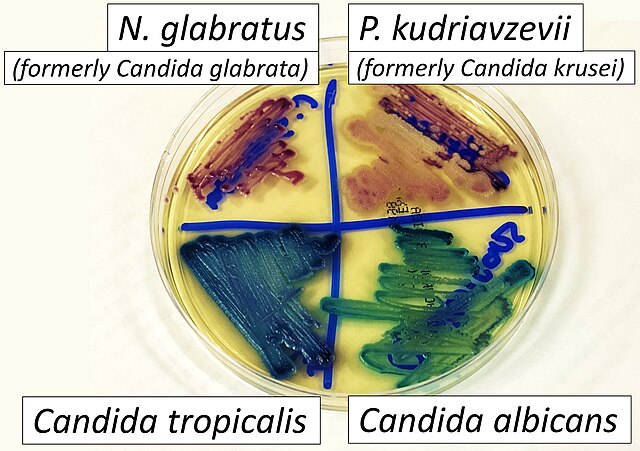
https://upload.wikimedia.org/wikipedia/commons/thumb/0/05/CHROMAgar_with_N_glabratus%2C_P_kudriavzevii%2C_Candida_albicans_and_Candida_tropicalis%2C_annotated.jpg/640px-CHROMAgar_with_N_glabratus%2C_P_kudriavzevii%2C_Candida_albicans_and_Candida_tropicalis%2C_annotated.jpg
Candida parapsilosis:
Candida parapsilosis is a yeast that is a major cause of fungal sepsis in humans. It has also been linked to wound and soft tissue infections, particularly in immunocompromised patients, and onychomycosis (nail infections). It is also commonly found in the environment, such as on the human skin, especially that of healthcare workers, in the soil, on insects, and even on domestic pets. Those who are most at risk for infection include the following:
Two newer species that fall into this category that resemble C. parapsilosis and are similar to it include C. orthopsilosis and C. marapsilosis. These are identified by the Vitek Mass Spectrophotometry Analyzer.
- Immunocompromised
- Post-surgical, especially gastrointestinal surgery
- Indwelling catheters
- Critical care patients
- Parenteral nutrition (IV feeding tube)
- Neonates
Two newer species that fall into this category that resemble C. parapsilosis and are similar to it include C. orthopsilosis and C. marapsilosis. These are identified by the Vitek Mass Spectrophotometry Analyzer.

This yeast is also a rapid-grower, maturing in 3 days. Colonies are also creamy, and somewhat "lacy" in appearance. This also grows well on Cornmeal-Tween 80 agar at 25 degrees Celsius. Microscopically, the yeast forms pseudohyphae that are short, crooked or curved, which bear blastoconidia either singly or in small clusters. Occasionally, large hyphal elements called "giant cells" may be observed as well. This species is inhibited by cycloheximide and the germ test is negative.
|
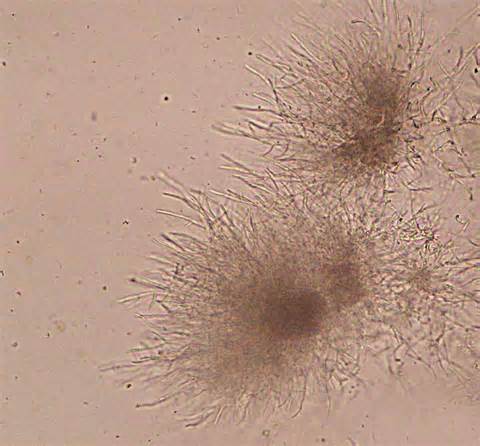
C. parapsilosis on Cornmeal Agar: "Shaggy Star" appearance
|
Candida pseudotropicalis:
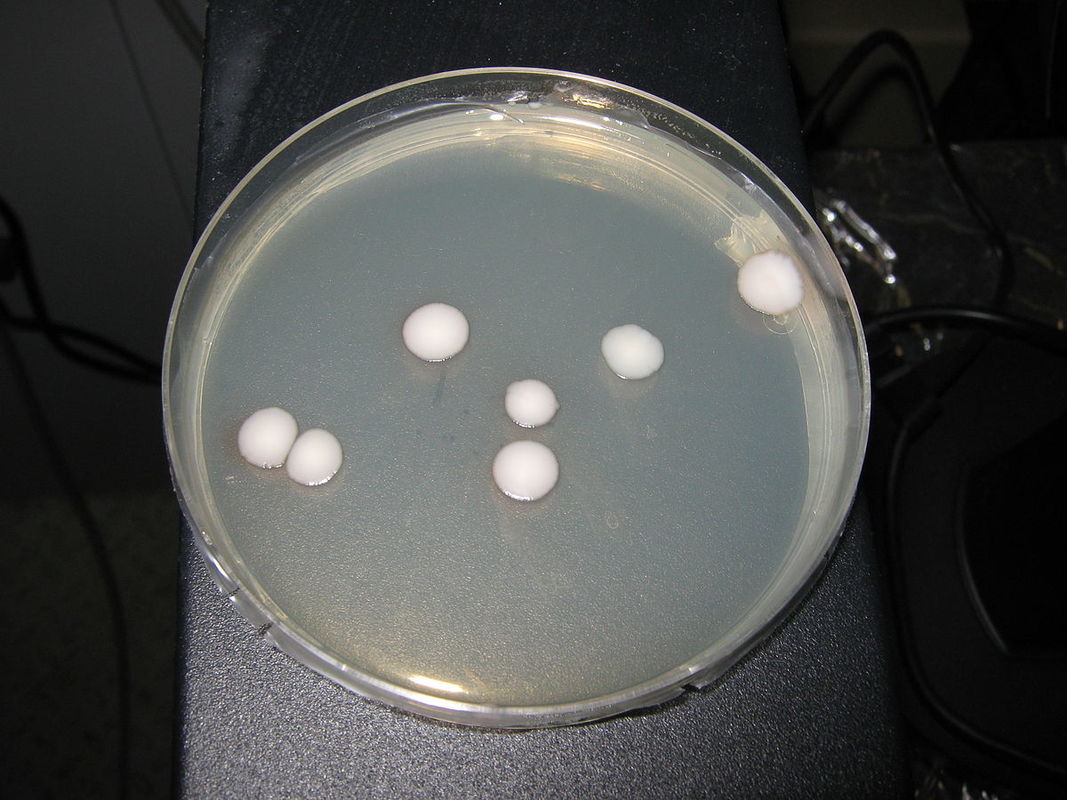
https://upload.wikimedia.org/wikipedia/commons/thumb/a/a1/Kluyveromyces_marxianus_colonies.jpg/1200px-Kluyveromyces_marxianus_colonies.jpg; Candida pseudotropicalis
|
C. pseudotropicalis grows quickly within 3 days and produces colonies that are creamy and smooth, growing well on Cornmeal-Tween 80 agar. Microscopically, on Cornmeal Agar, it is viewed as a "logs in the stream" appearance, with short pseudohyphae bearing elongated blastoconidia that line up and parallel each other. The germ tube test is negative.
|

Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
Candida tropicalis:
Colony growth on glucose peptone agar resembles that of C. albicans, as colonies are white or cream in color, glistening, smooth or dull, and may have rough edges. On Cornmeal agar, there are true hyphae and pseudohyphae, blastospore production in clusters at intervals along the hyphae, and sometimes there are also single, internodal blastospores as well. They resemble "tree branches". Unlike C. albicans, there is no production of chlamydospores and the yeast is unable to ferment sucrose.
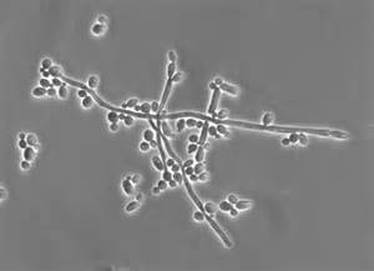
C. tropicalis elegantly forms long pseudohyphae and some true hyphae which bear single or small groups of blastoconidia, which are round-to-oval-to-teardrop in shape with a few teardrop-shaped chlamydospores
|
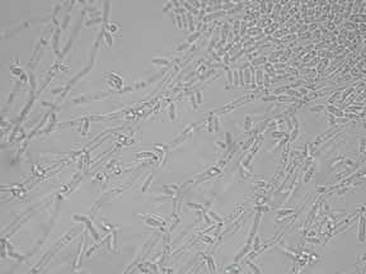
C. tropicalis on Cornmeal Agar: Growth is inhibited by cycloheximide and the germ tube test is negative
|
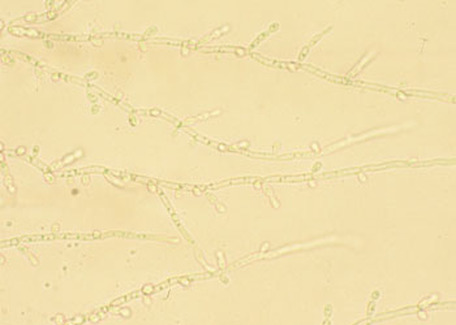
C. tropicalis on Cornmeal Agar
|

Candida tropicalis is a rapid grower, maturing in just 3 days. Colonies are creamy, cream-colored with a mycelial fringe and grow well on Cornmeal-Tween 80 or SAB agars at 25 degrees Celsius
|
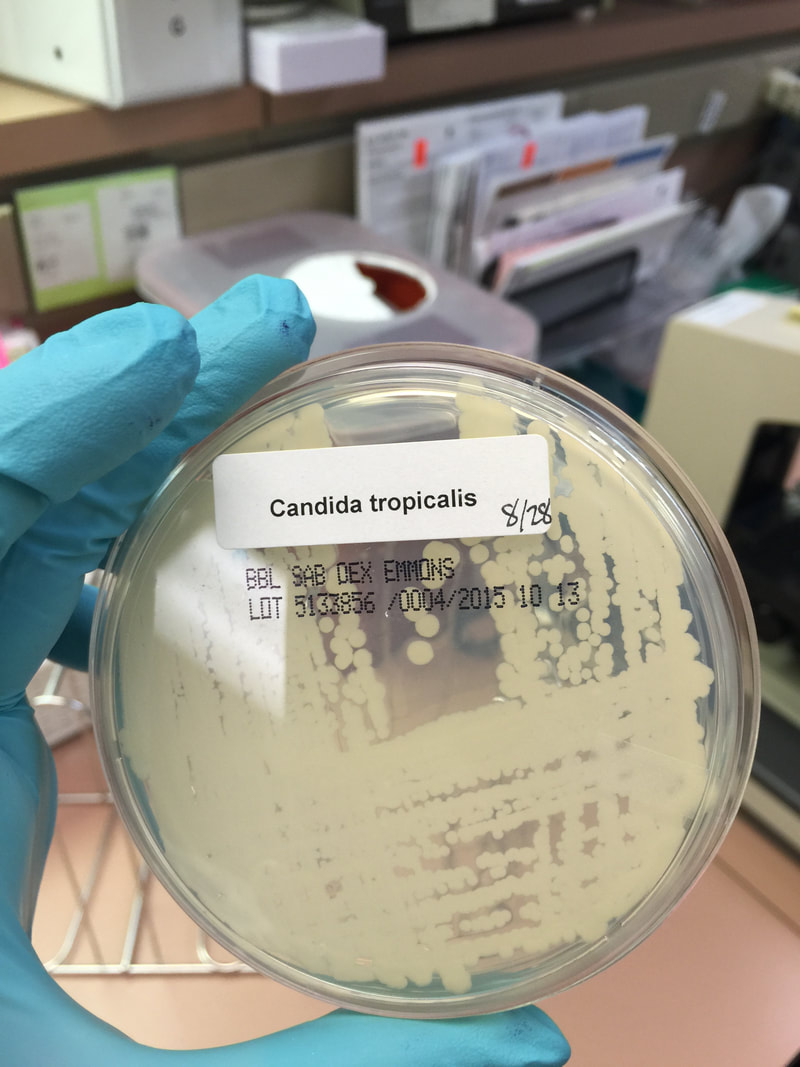
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
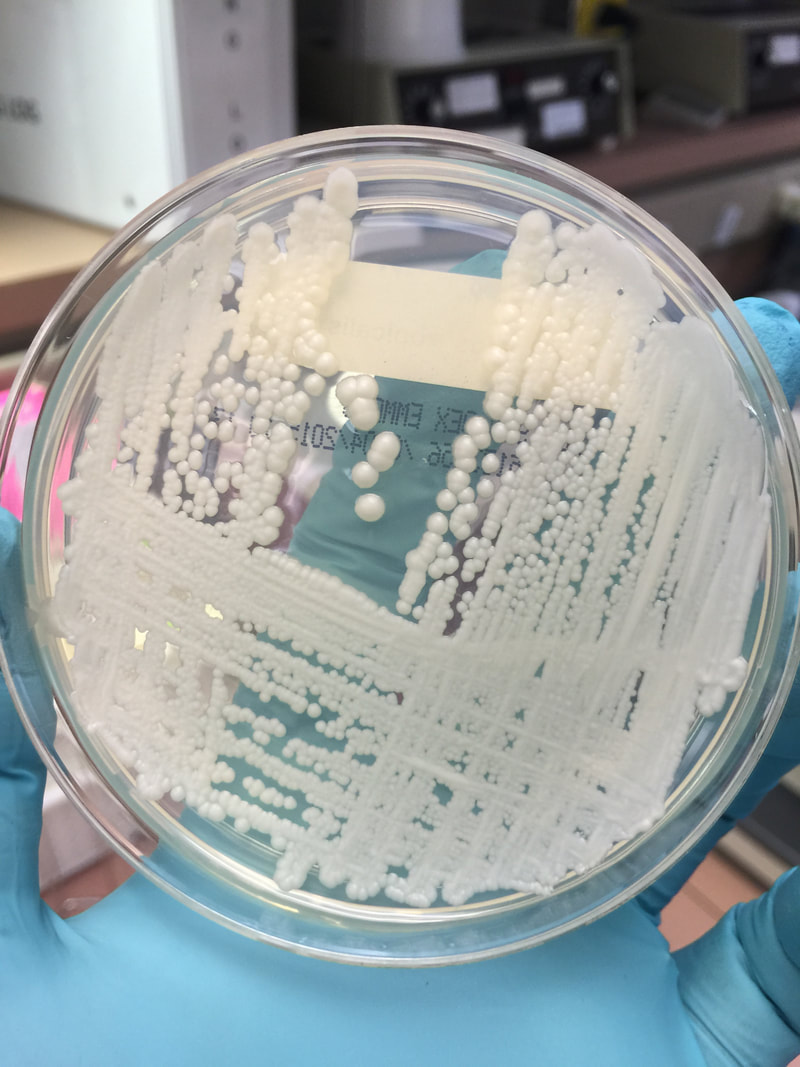
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
Colonies are pearly, round and glabrous
|
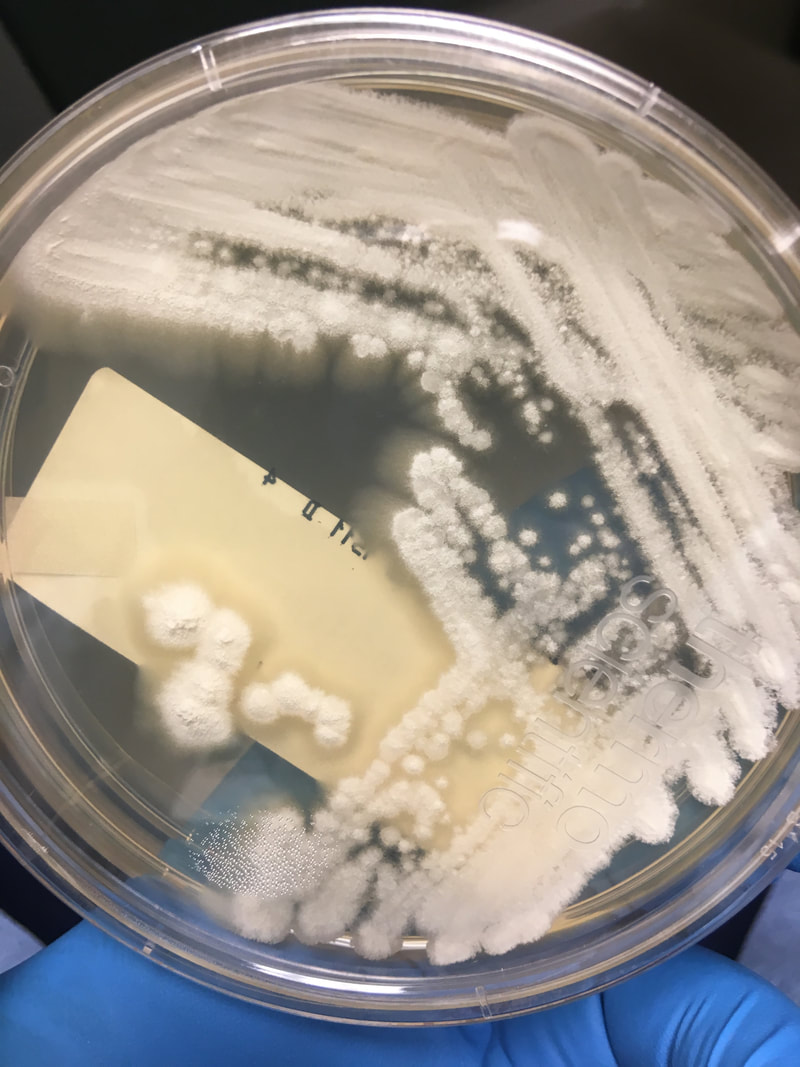
An older, fuzzy version of C. tropicalis, grown and taken by Jeanette Reynolds, MLS-AMT, M-ASCP. Yeasts like this one can sometimes grow extensions to reach out into the agar to access the nutrients, and we often refer to them as "feet". Fuzzy yeasts can resemble molds. This one was identified by the MALDI-TOF Mass Spec.
|

This is the original plate prior to the subculture of C. tropicalis, grown and taken by Jeanette Reynolds, M-ASCP, MLS-AMT.
|
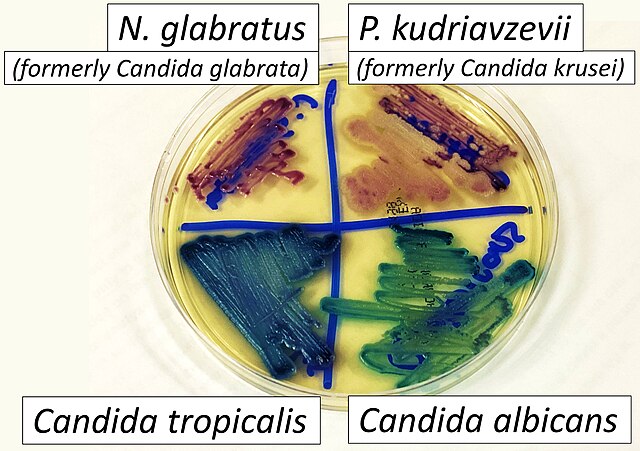
https://upload.wikimedia.org/wikipedia/commons/thumb/0/05/CHROMAgar_with_N_glabratus%2C_P_kudriavzevii%2C_Candida_albicans_and_Candida_tropicalis%2C_annotated.jpg/640px-CHROMAgar_with_N_glabratus%2C_P_kudriavzevii%2C_Candida_albicans_and_Candida_tropicalis%2C_annotated.jpg
Candida lusitaniae:
C. lusitaniae produces colonies that are white to cream, glistening and smooth on glucose peptone agar, and produces long pseudohyphae with few branches and abundant, small clusters of oval blastospores on Cornmeal agar. It has the ability to assimilate rhamnose.
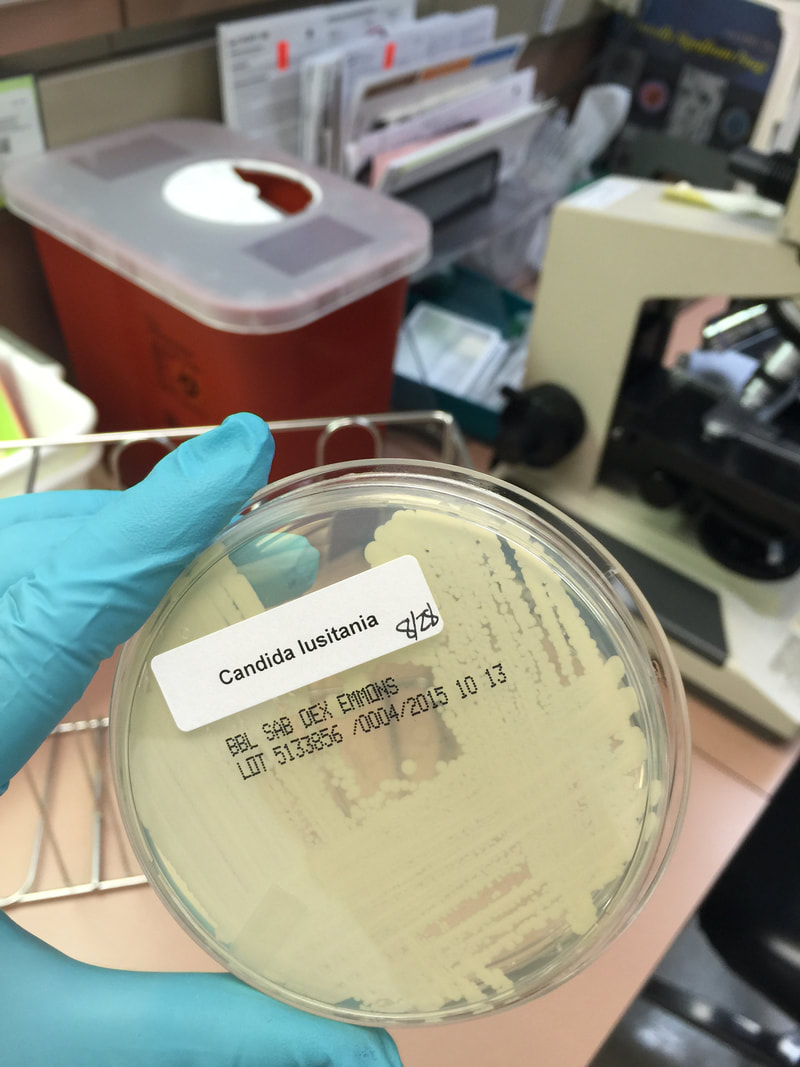
Image by Jeanette Sprute, MT-AMT, M-ASCP (cm), 2015, own work
|
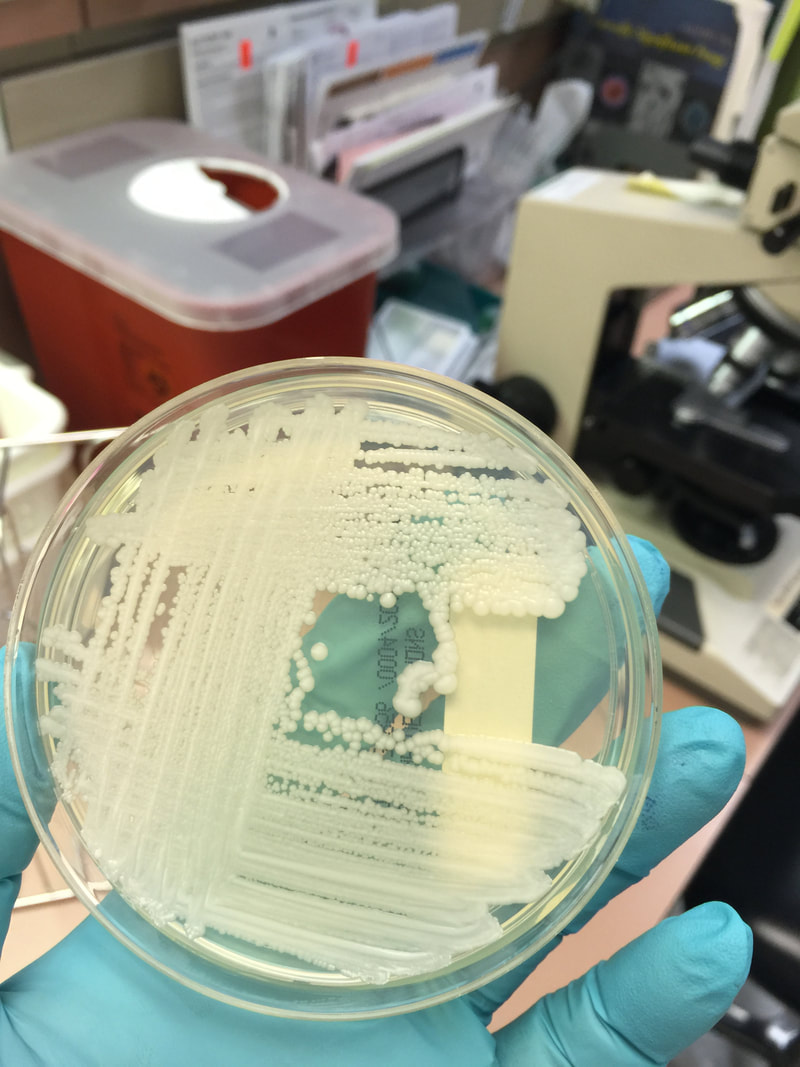
Image by Jeanette Sprute, MT-AMT, M-ASCP (cm), 2015, own work
|
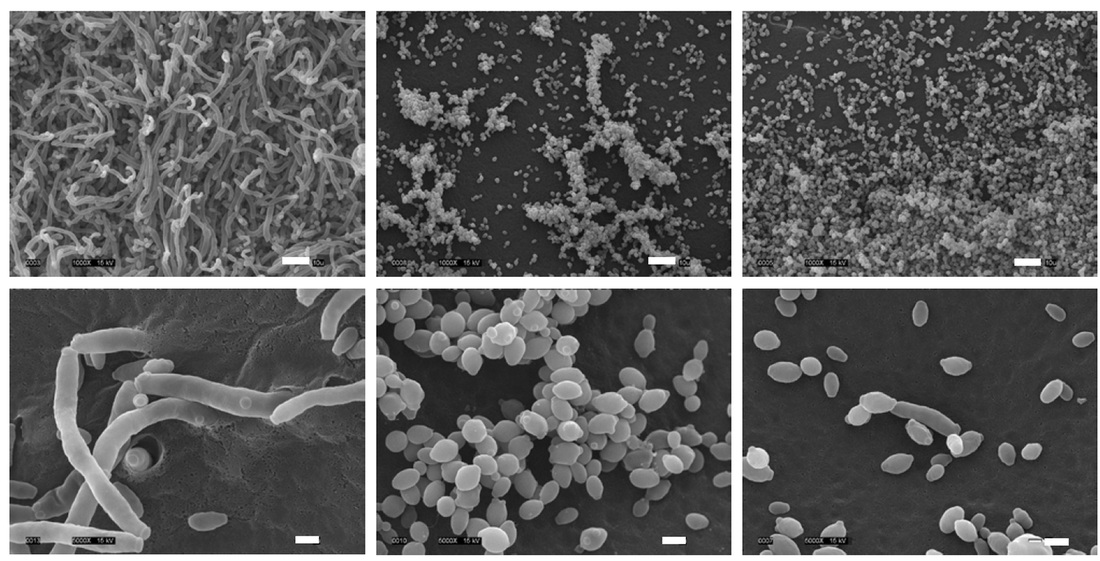
Candida lusitaniae is a rapid-grower that matures in 3 days and grows as creamy, cream-colored, smooth, glistening colonies on Cornmeal-Tween 80 agar at 25 degrees Celsius. Microscopically, the pseudohyphae are long and narrow, curved, branched, and bear oval-shaped blastoconidia. The germ tube test is negative.
Candida glabrata:
C. glabrata produces 2.5 to 3 x 4 micrometer round, oval and elongated budding yeast cells seen in wet mount or by LPCB stain on cellophane tape prep. It is of low virulence, however, it is a significant cause of secondary infection in the immunocompromised patient. Cells produced no or just a few small pseudohyphae. It ferments glucose and trehalose only. Macroscopically, on SAB agar, colonies are smooth, cream-colored, and glistening but some strains become brownish-gray as they age. C. glabrata and C. auris appear as identical and their resistance to antifungals is on the rise, which is of concern.
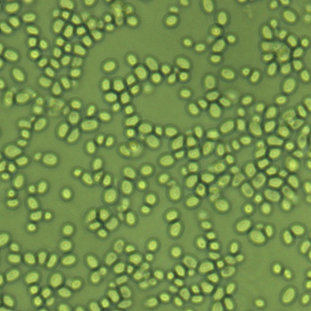
C. glabrata grow as oval, single terminal budding cells that are noncapsulated without any pseudohyphae, often arranged in tight clusters.https://upload.wikimedia.org/wikipedia/commons/thumb/7/7b/Glabrata.jpg/640px-Glabrata.jpg
|
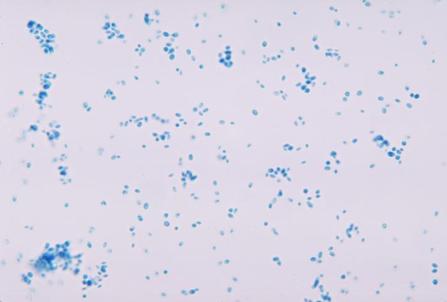
Yeast cells produced by C. glabrata
|

This is a rapid-grower, maturing in 3 days. It produces large colonies, cream-colored, pasty, convex, glossy and smooth. Sometimes they are tan-beige and umbonate in the middle.
|
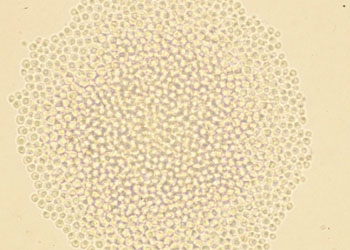
C. glabrata on Cornmeal Agar: Yeast cells and budding yeast cells only, no pseudohyphae or hyphae seen
|
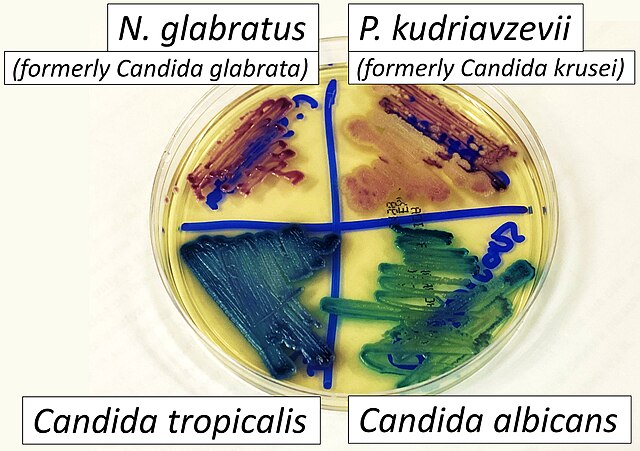
https://upload.wikimedia.org/wikipedia/commons/thumb/0/05/CHROMAgar_with_N_glabratus%2C_P_kudriavzevii%2C_Candida_albicans_and_Candida_tropicalis%2C_annotated.jpg/640px-CHROMAgar_with_N_glabratus%2C_P_kudriavzevii%2C_Candida_albicans_and_Candida_tropicalis%2C_annotated.jpg
Candida auris:

Candida auris presents very similar to Candida glabrata, and is also inherently quite resistant to antifungals, particularly the azoles. Colonies are cream-colored and matte to slightly shiny on SAB dextrose agar. https://upload.wikimedia.org/wikipedia/commons/thumb/d/d0/Candida-auris_2016-250px.jpg/800px-Candida-auris_2016-250px.jpg
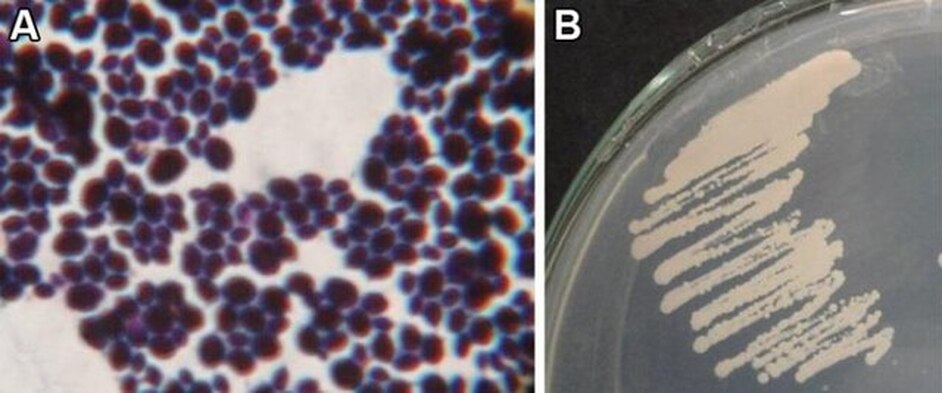
https://upload.wikimedia.org/wikipedia/commons/thumb/b/bd/Candida_auris_%28Kumar_2015%29.jpg/640px-Candida_auris_%28Kumar_2015%29.jpg
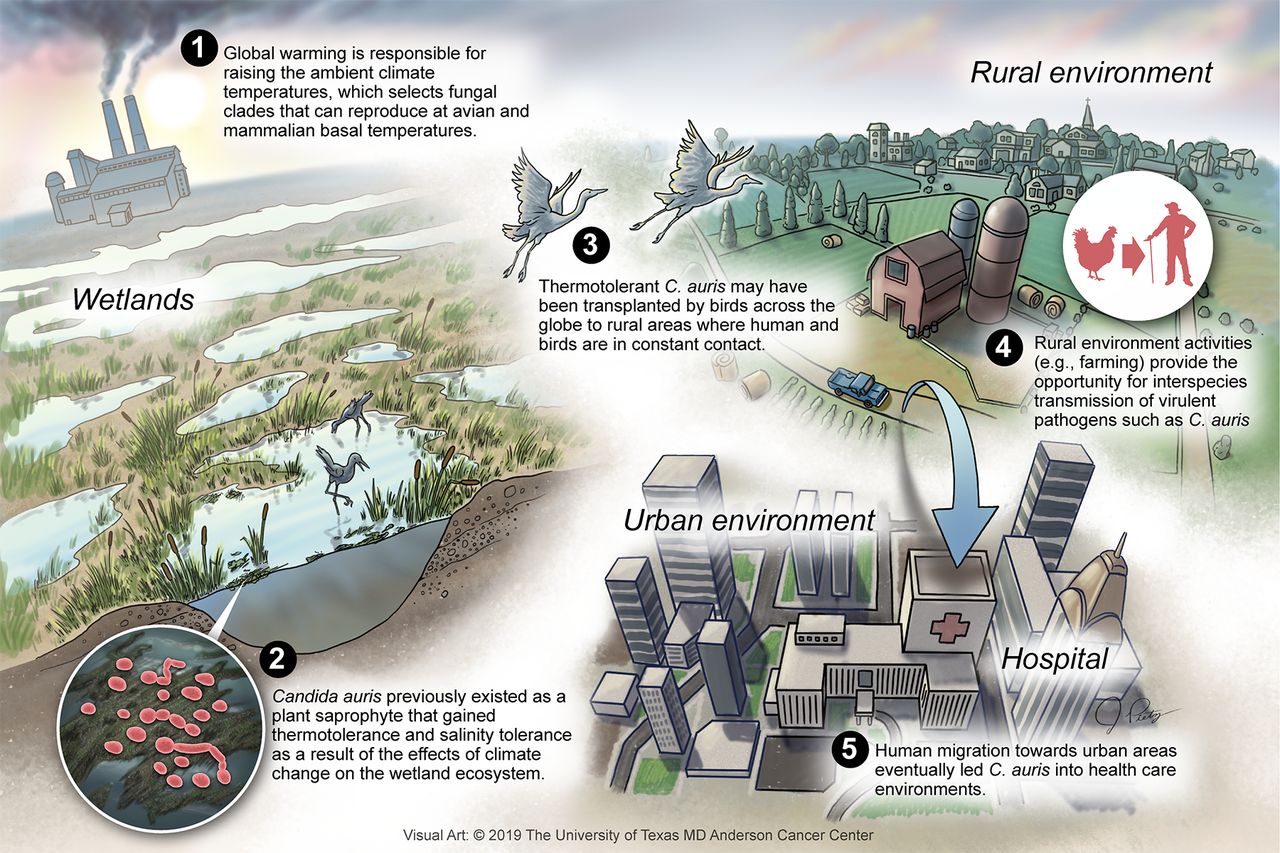
https://upload.wikimedia.org/wikipedia/commons/0/0a/Proposed_scheme_for_the_emergence_of_Candida_auris.jpg
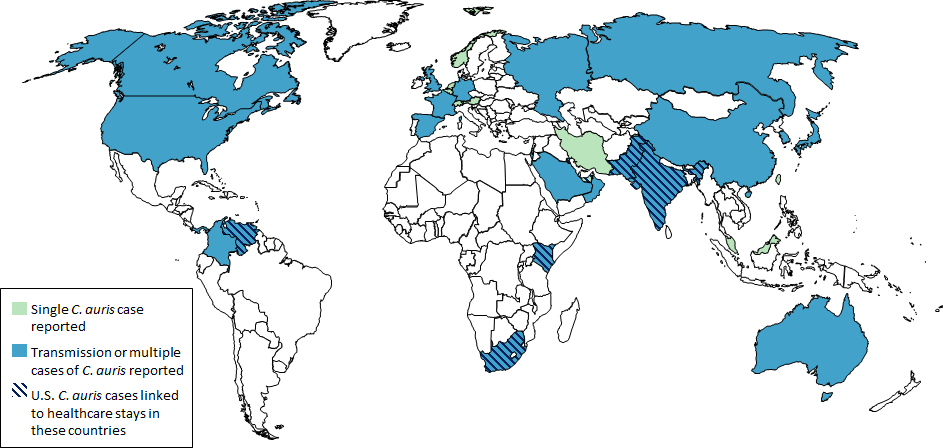
https://upload.wikimedia.org/wikipedia/commons/b/b5/Candida_auria_infections_world_distribution_2019.png
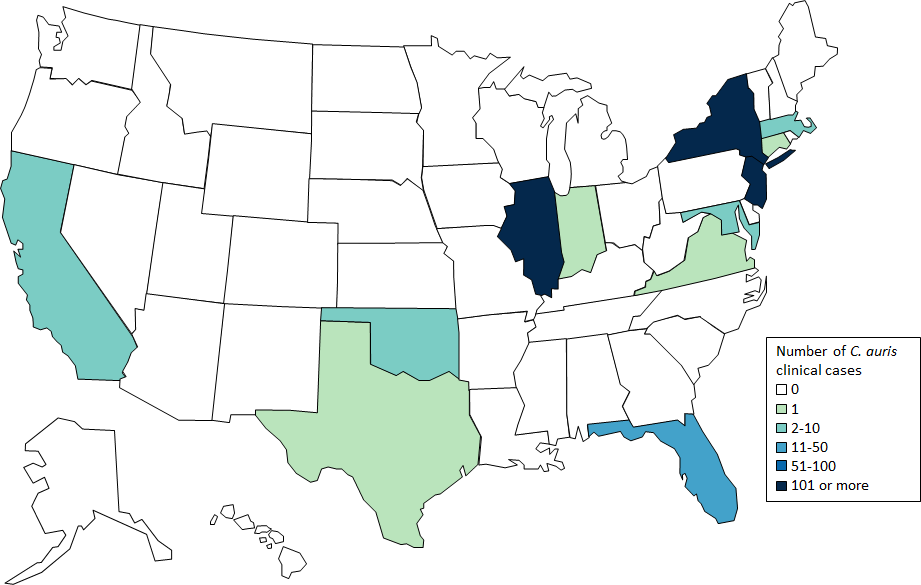
https://upload.wikimedia.org/wikipedia/commons/7/7b/Map_of_Candida_auris_infections_in_US_as_of_2019.png
Candida guillermondii:
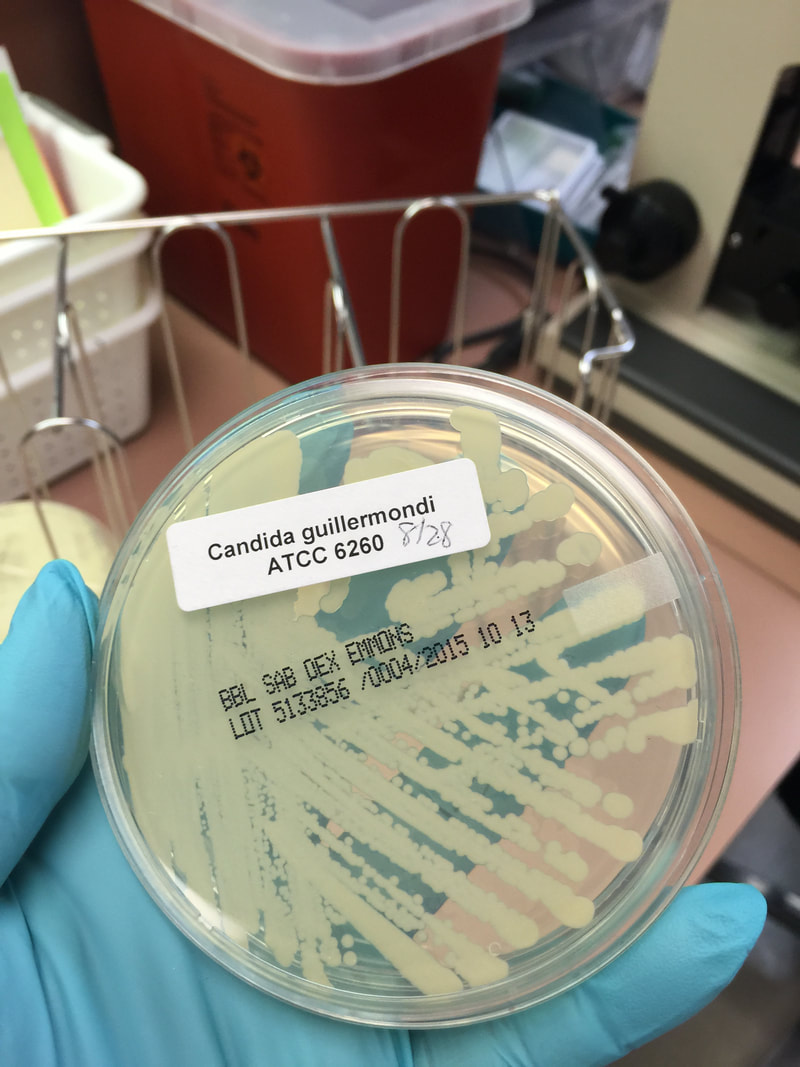
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
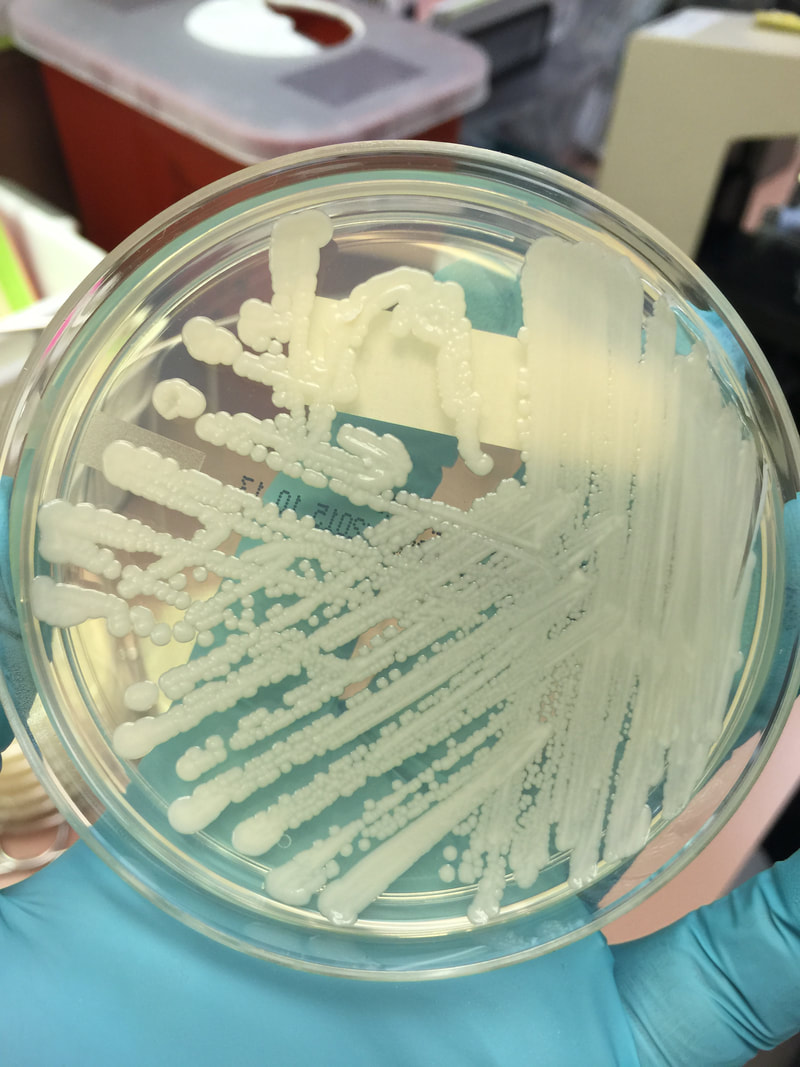
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
Candida kefyr:
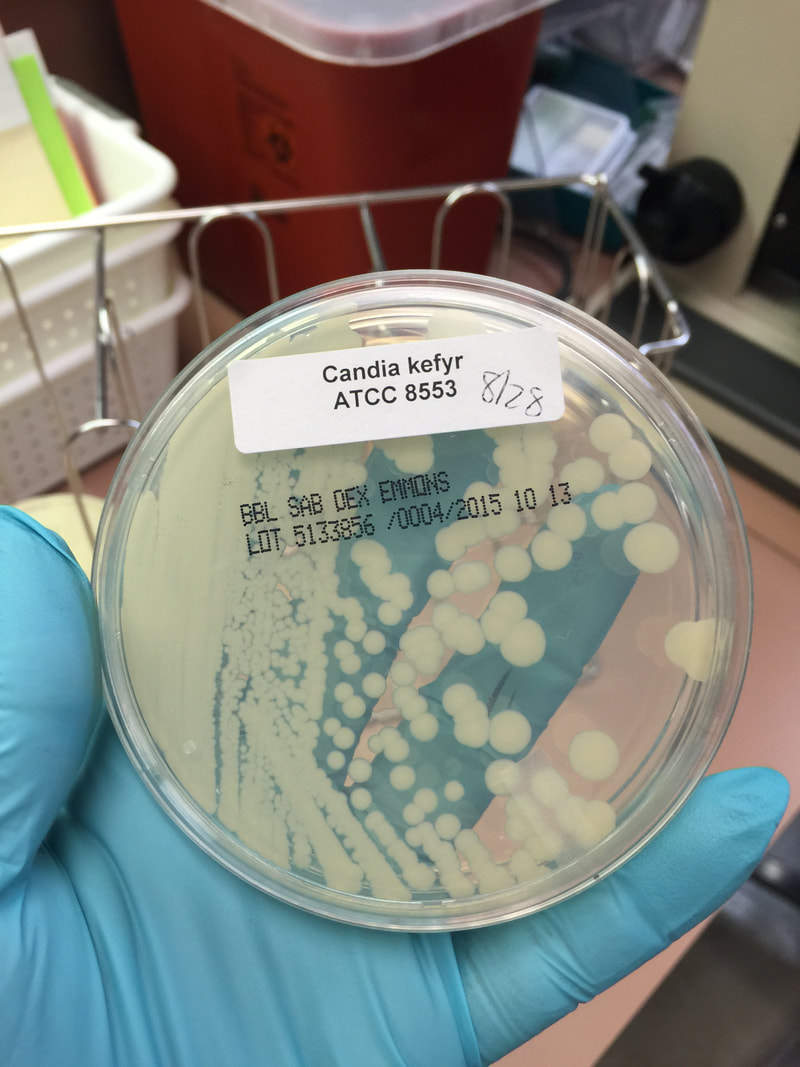
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
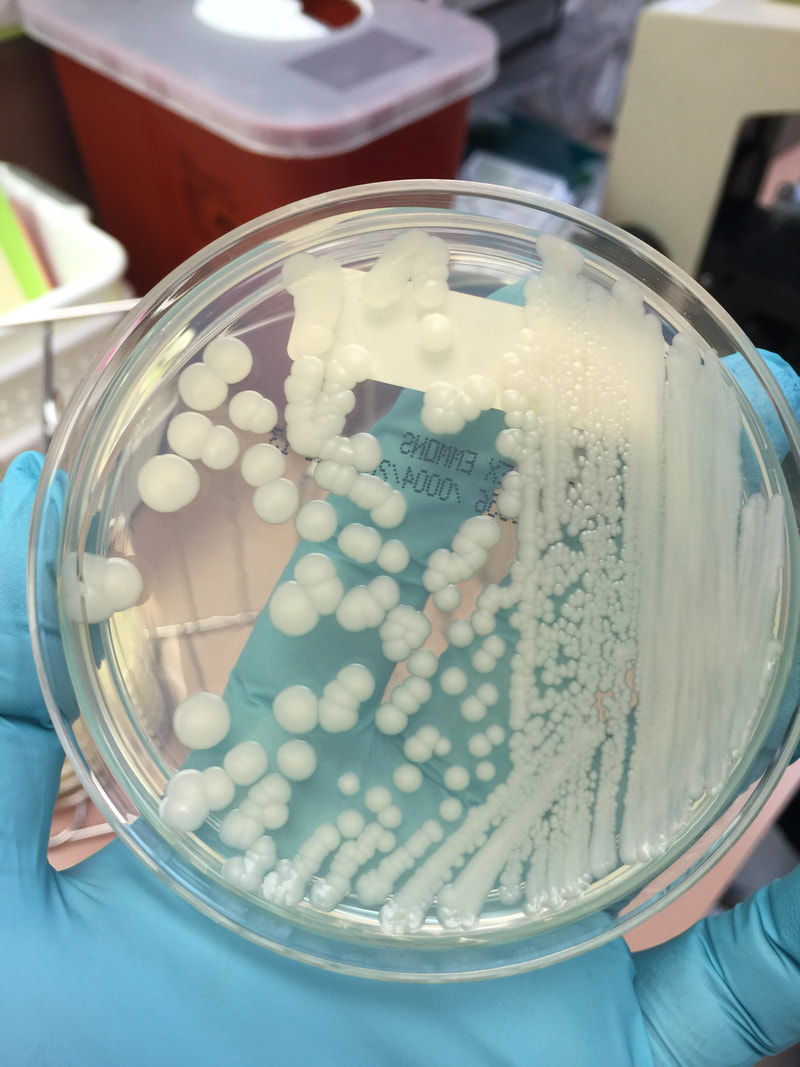
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
Candida dubliniensis:
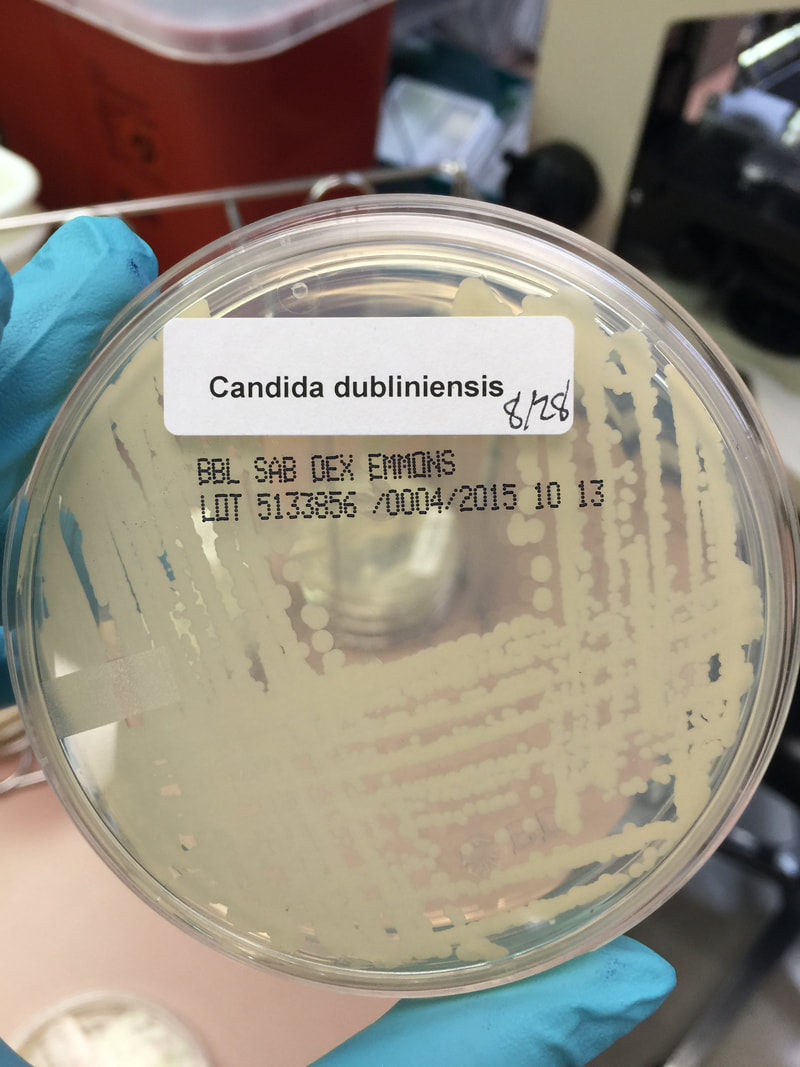
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
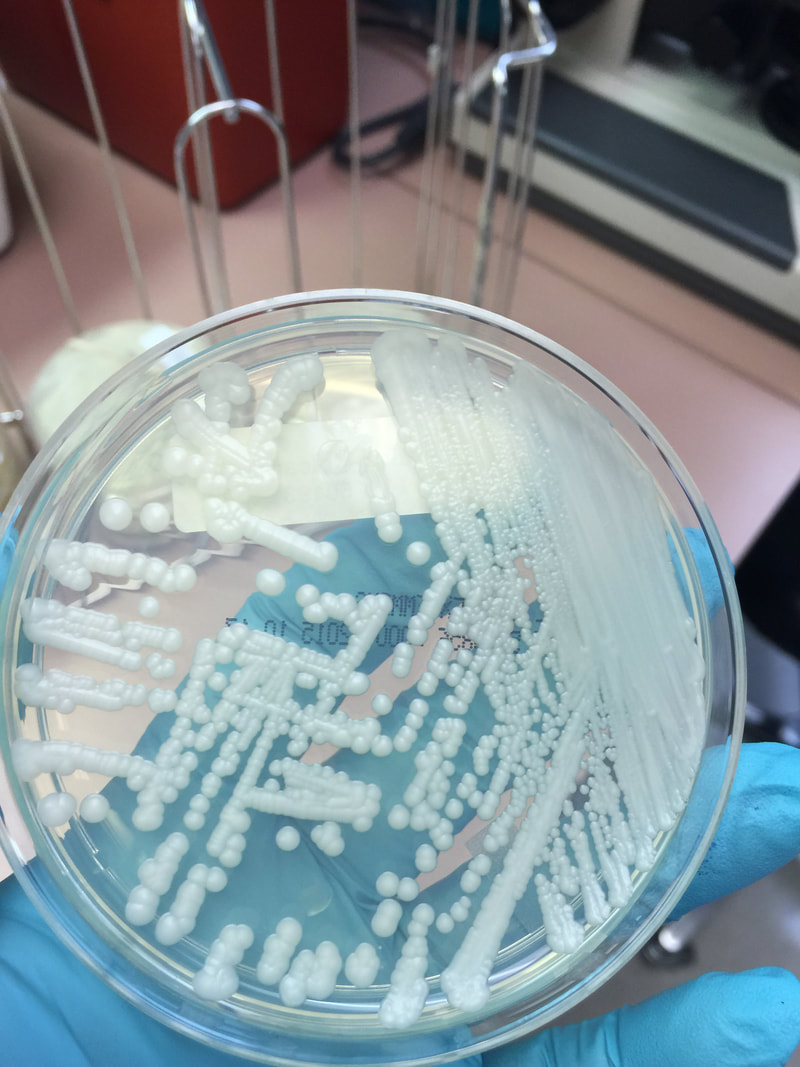
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work; Produces white, raised, round, somewhat "pearly" colonies on SAB
|
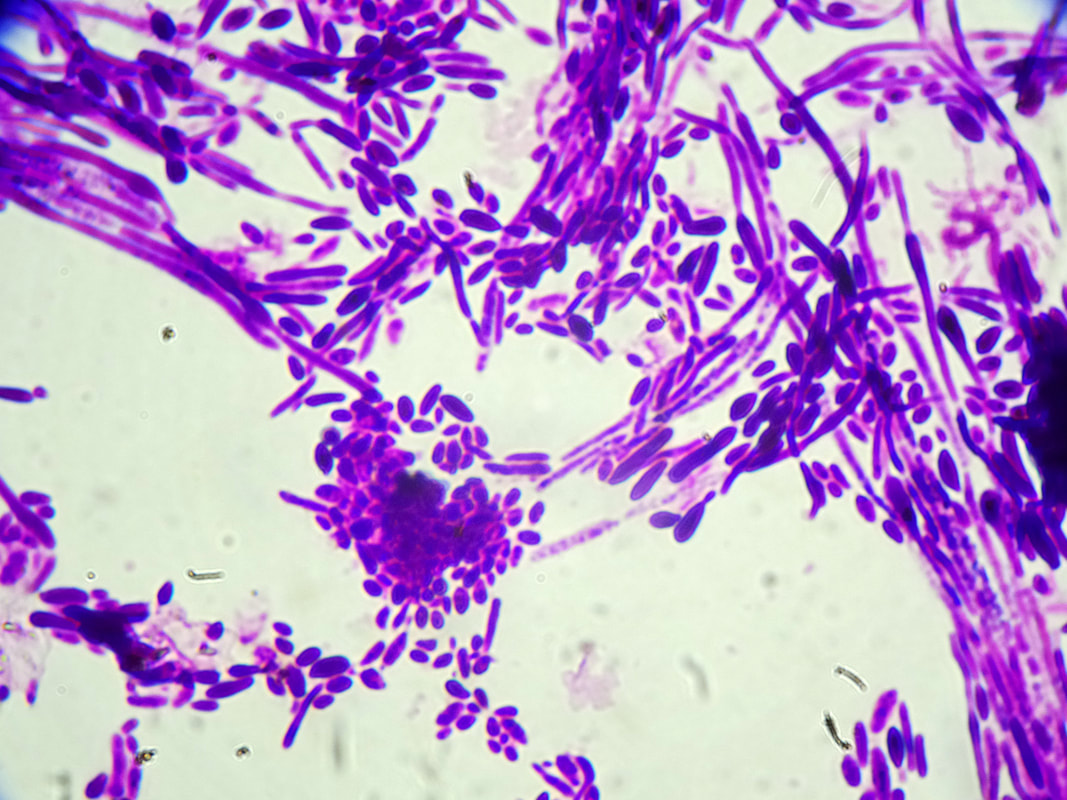
By Stefan Walkowski - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=44448835
Cryptococcus species:
Cryptococcus spp are yeasts that are unicellular, thick-walled, encapsulated round-to-slighly oval yeasts. C. neoformans is of concern because it is linked to meningitis in both immunocompetent and immunocompromised individuals. Infection can begin in the lungs, get into the bloodstream and spread to the meninges. It is mainly associated with fungal meningitis in HIV/AIDS patients. The mortality rate is high, at 10-30% (approximately).
Cryptococcus neoformans is a complex that causes cryptococcosis. The infection can be subacute or chronic and is most often linked with the tissue of the central nervous system. Lesions have been found in the skin, in the bones, on the lungs or other organs, but meningitis is considered to be the most serious of the infections. Other Cryptococcus spp other than gattii are mostly nonpathogenic, but can cause rare disease in those who are severely immunocompromised. The most common source and carrier of the yeast is pigeons and pigeon droppings, specifically.
This organism has become resistant to the echinocandins, but is still susceptible to amopherecin B, triazoles, and flucytosine.
On SAB agar, it produces flat-to-slightly heaped colonies that are shiny and moist. There are mucoid strains, too. The color starts out as cream, but darkens to tan. On Niger (bird) seed agar, it produces brown colonies.
The microscopic morphology on CMA is cells that are round, dark, and budding without any hyphae. In India Ink, you can see the capsules around the yeast cells as distinct, clear halos against the black background. Not all strains produce apparent capsules, so this is something to be aware of. In urease agar, C. neoformans produces a positive test (fuschia) and the caffeic acid test will be positive.
Cryptococcus gattii species complex is also similar to C. neoformans, but the cells are more oval in shape. Infections can occur in immunocompromised individuals where lesions can be found in the lungs and rain, and are more common in tropical, subtropical, and temperate regions. It thrives in decayed hollows and on the surfaces of many different types of trees globally. It has been isolated from wood and wood products, from soil, water, air, mammals, and other places, and it is naturally resistant to the echinocandins.
On agar, it looks just like C. neoformans. The best means of identification is the MALDI-TOF MS or DNA by PCR.
Cryptococcus spp are yeasts that are unicellular, thick-walled, encapsulated round-to-slighly oval yeasts. C. neoformans is of concern because it is linked to meningitis in both immunocompetent and immunocompromised individuals. Infection can begin in the lungs, get into the bloodstream and spread to the meninges. It is mainly associated with fungal meningitis in HIV/AIDS patients. The mortality rate is high, at 10-30% (approximately).
Cryptococcus neoformans is a complex that causes cryptococcosis. The infection can be subacute or chronic and is most often linked with the tissue of the central nervous system. Lesions have been found in the skin, in the bones, on the lungs or other organs, but meningitis is considered to be the most serious of the infections. Other Cryptococcus spp other than gattii are mostly nonpathogenic, but can cause rare disease in those who are severely immunocompromised. The most common source and carrier of the yeast is pigeons and pigeon droppings, specifically.
This organism has become resistant to the echinocandins, but is still susceptible to amopherecin B, triazoles, and flucytosine.
On SAB agar, it produces flat-to-slightly heaped colonies that are shiny and moist. There are mucoid strains, too. The color starts out as cream, but darkens to tan. On Niger (bird) seed agar, it produces brown colonies.
The microscopic morphology on CMA is cells that are round, dark, and budding without any hyphae. In India Ink, you can see the capsules around the yeast cells as distinct, clear halos against the black background. Not all strains produce apparent capsules, so this is something to be aware of. In urease agar, C. neoformans produces a positive test (fuschia) and the caffeic acid test will be positive.
Cryptococcus gattii species complex is also similar to C. neoformans, but the cells are more oval in shape. Infections can occur in immunocompromised individuals where lesions can be found in the lungs and rain, and are more common in tropical, subtropical, and temperate regions. It thrives in decayed hollows and on the surfaces of many different types of trees globally. It has been isolated from wood and wood products, from soil, water, air, mammals, and other places, and it is naturally resistant to the echinocandins.
On agar, it looks just like C. neoformans. The best means of identification is the MALDI-TOF MS or DNA by PCR.
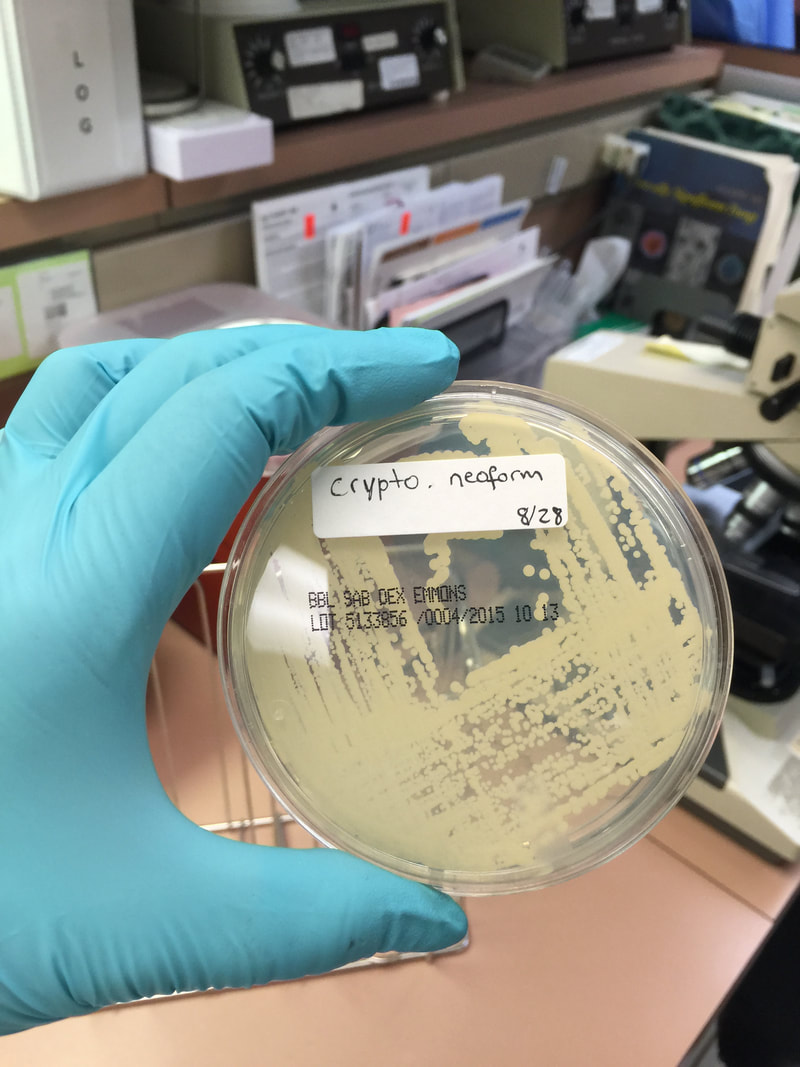
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
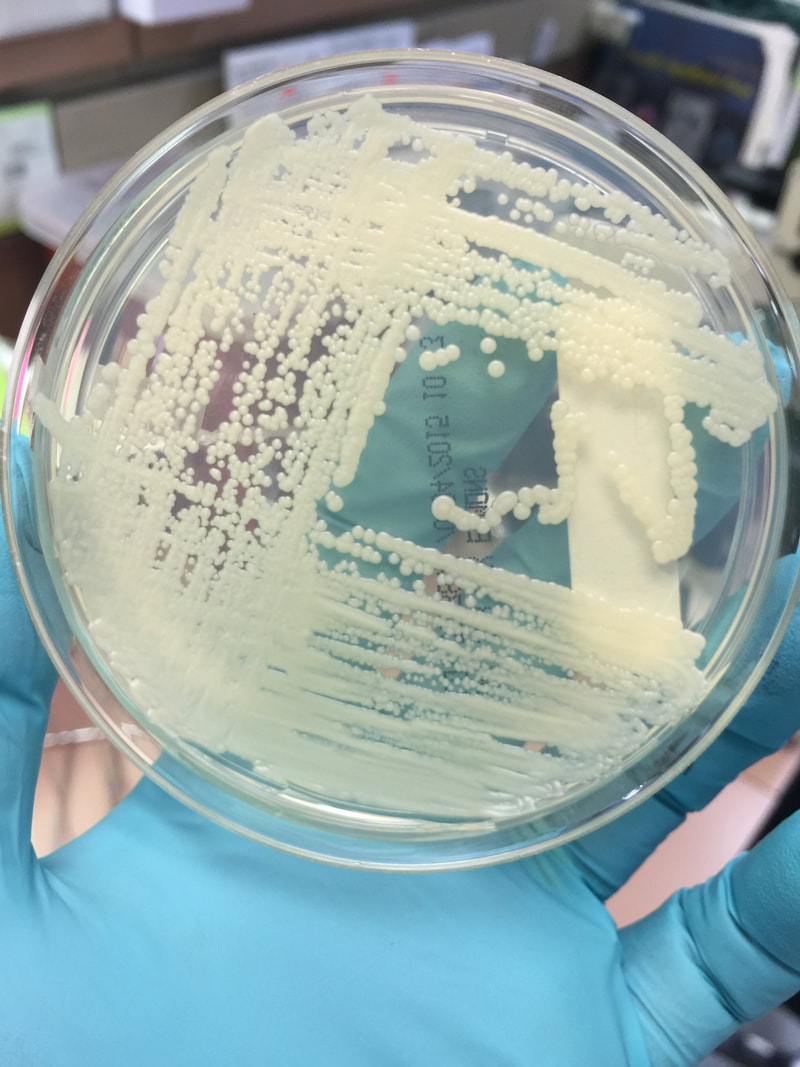
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
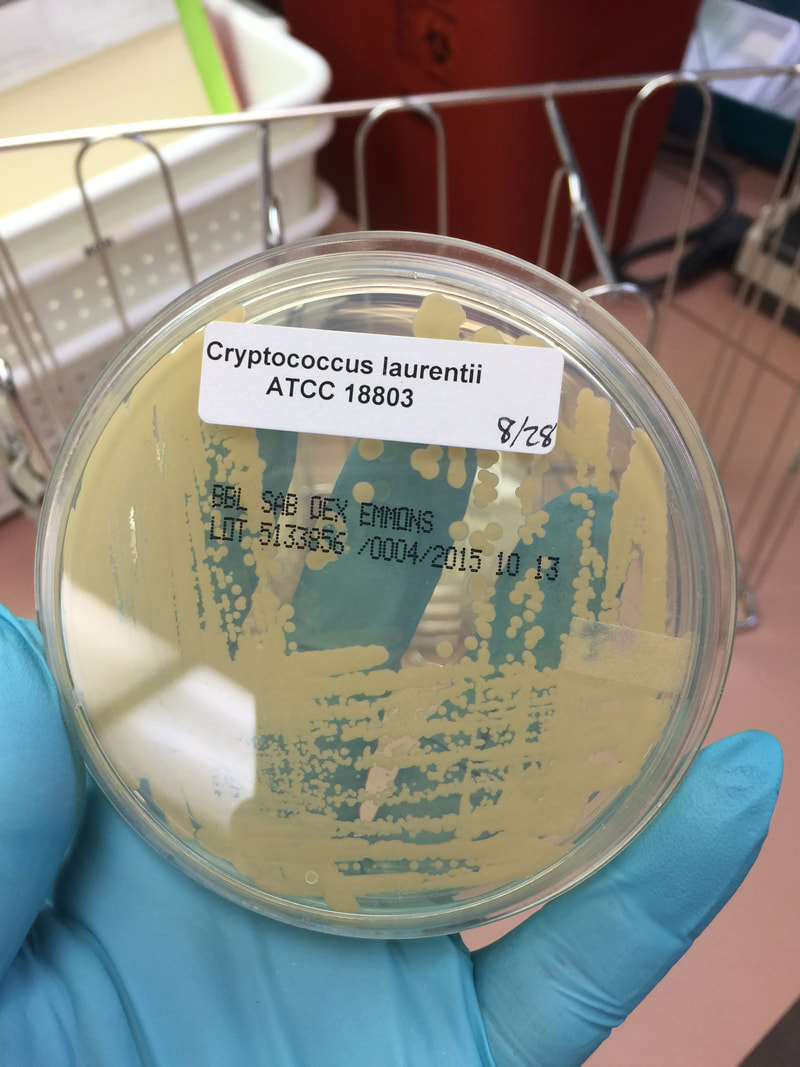
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
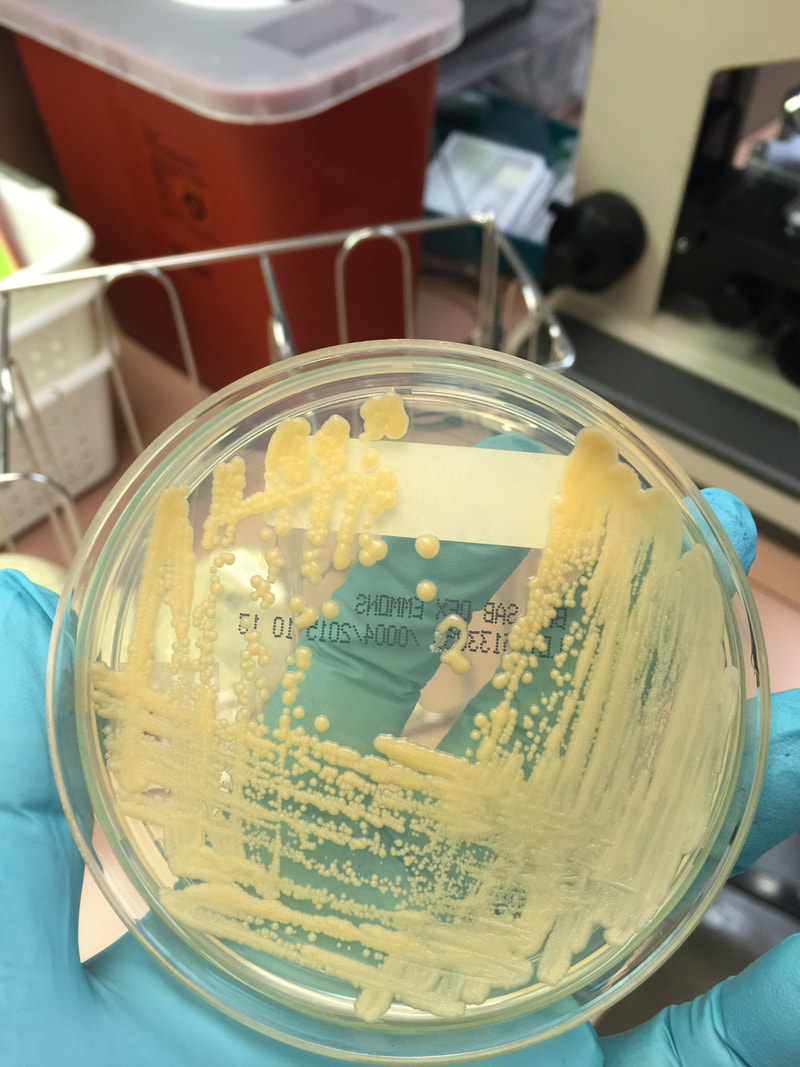
Image by Jeanette Reynolds, MT-AMT, M-ASCP (cm), 2015, own work
|
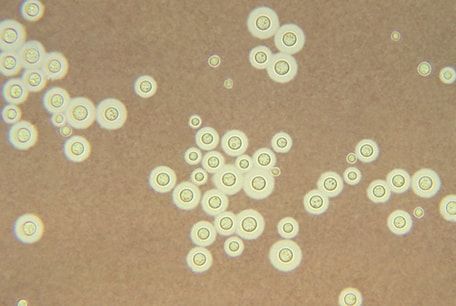
India Ink stain: Cryptococcus neoformans in India Ink wet mount appears as round spheres with a large "halo" or clearing around them due to the encapsulated cells
|
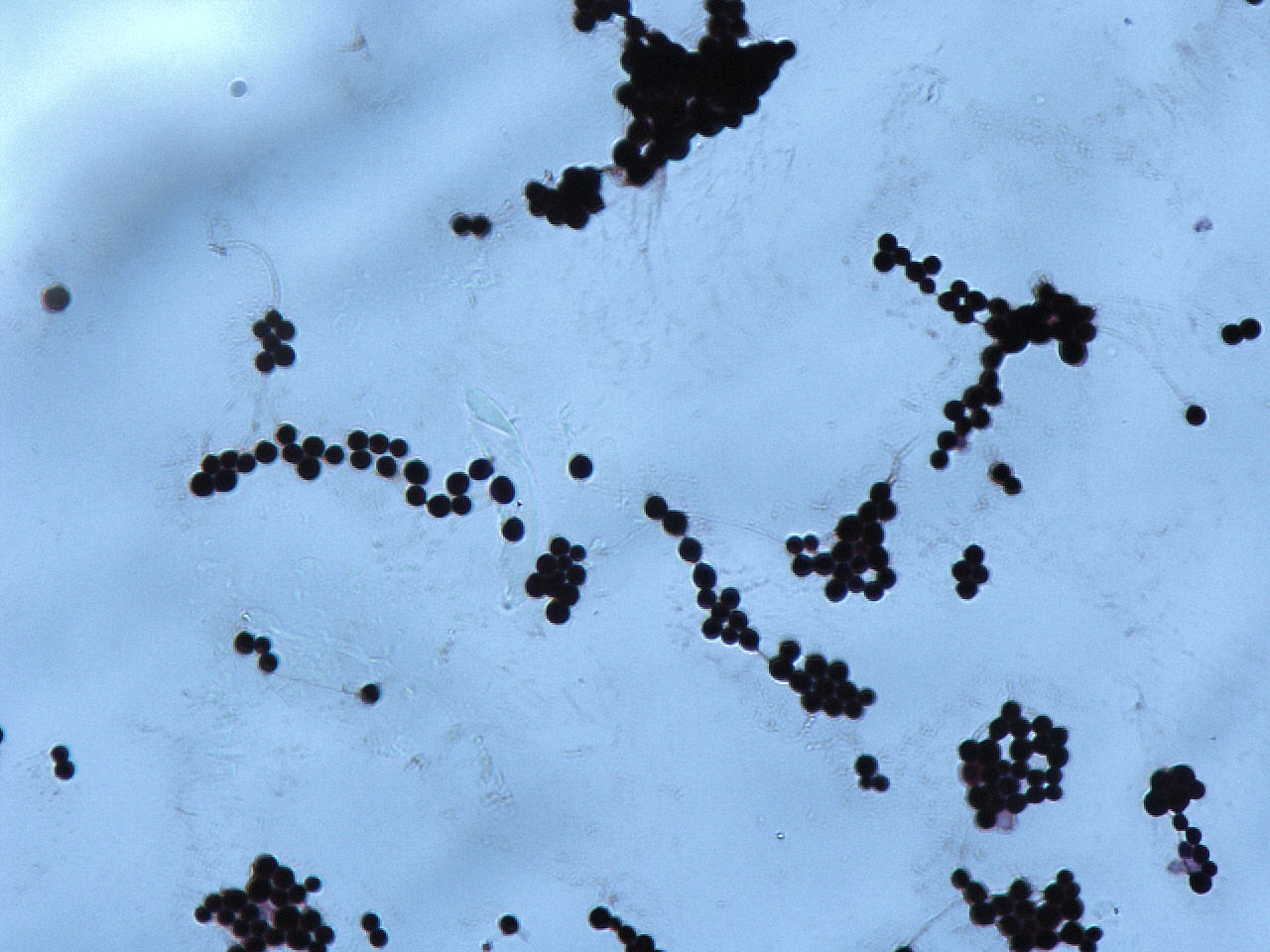
Here is a Gram Stain of Cryptococcus neoformans
|
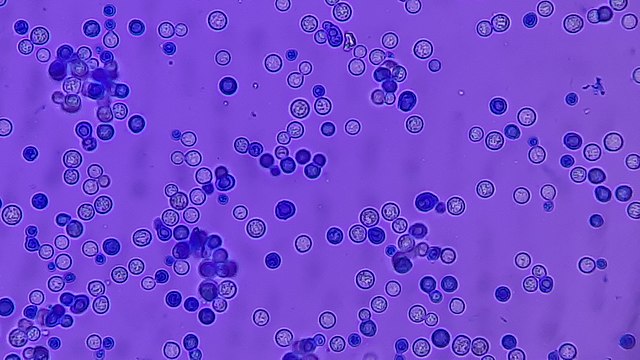
LPCB, https://upload.wikimedia.org/wikipedia/commons/thumb/4/46/Cryptococcus_in_LPCB_mount_of_Culture.jpg/640px-Cryptococcus_in_LPCB_mount_of_Culture.jpg
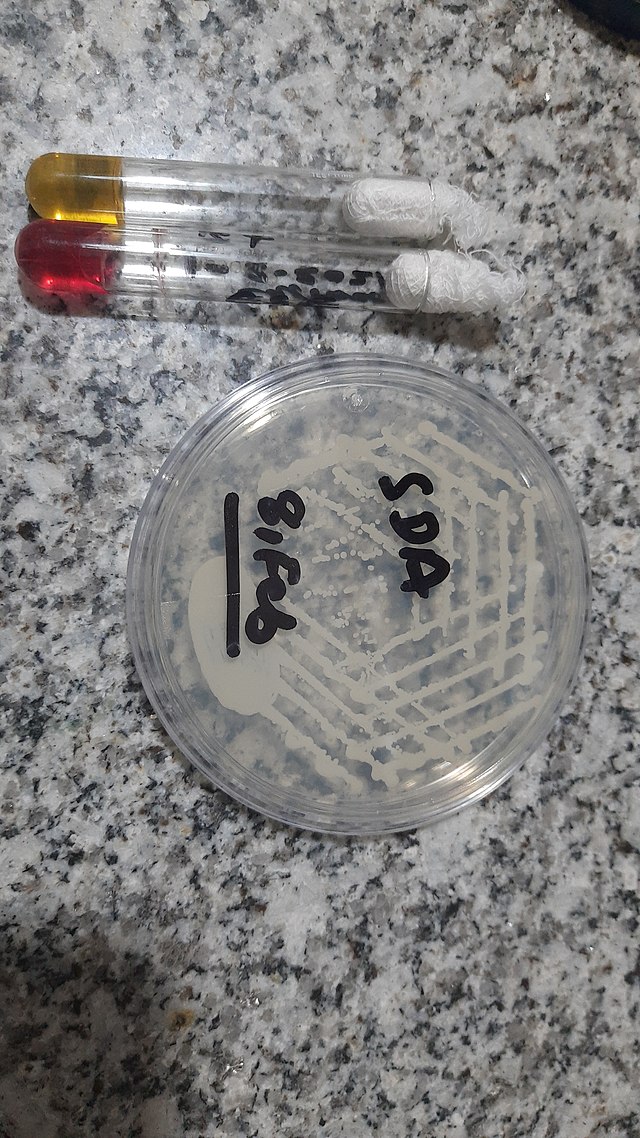
https://upload.wikimedia.org/wikipedia/commons/thumb/1/1a/Cryptococcus_neoformans_growth_on_SDA_and_Urease_test_Positive.jpg/640px-Cryptococcus_neoformans_growth_on_SDA_and_Urease_test_Positive.jpg
|
C. gattii growing on birdseed agar, and C. neoformans growing as brown colonies on birdseed agar, https://upload.wikimedia.org/wikipedia/commons/thumb/2/2f/Cryptococcus_gattii_selection.jpg/640px-Cryptococcus_gattii_selection.jpg
|
This is an India Ink microscope test that is positive for Cryptococcus in the cerebrospinal fluid (CSF), https://upload.wikimedia.org/wikipedia/commons/thumb/9/9a/Cryptococcus_in_cerebrospinal_fluid%2C_India_ink_prep._%2849623531757%29.jpg/640px-Cryptococcus_in_cerebrospinal_fluid%2C_India_ink_prep._%2849623531757%29.jpg
|
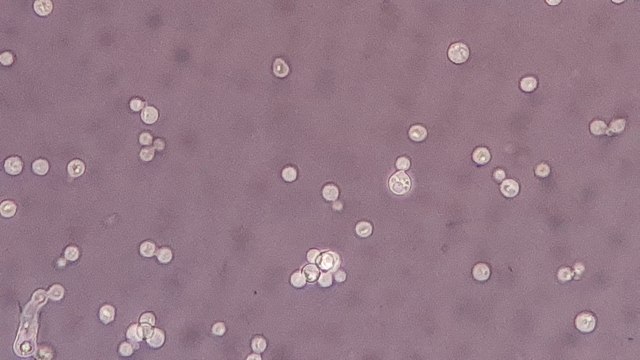
India Ink test revealing C. albicans yeast cells, https://upload.wikimedia.org/wikipedia/commons/thumb/d/dd/Cryptococcus_neoformans_in_India_Ink_from_culture_Microscopic_Footage.jpg/640px-Cryptococcus_neoformans_in_India_Ink_from_culture_Microscopic_Footage.jpg
|
Rhodotorula spp:
Normally a ubiquitous organism, the saprophytic Rhodotorula spp discovered in 1985 by Harrison are common contaminants of the air, water, showerheads, soil, milk, and even fruit juice, however, they can cause opportunistic infections in patients at terminal stages of debilitating diseases such as cancer (leukemia or carcinoma in particular) or bacterial endocarditis. They have been recovered in the sputum, urine and blood. They are not a virulent spp.
According to the American Society for Microbiology (ASM) and the National Institute for Health (NIH), those who are immunosuppressed, have underlying health conditions, malignancies, who are on corticosteroids, cytotoxic drugs, broad spectrum antibiotics, or who have central intravenous catheters are at risk for infection with this organism. Prior to 1985, there were no known infections with this yeast, however, it is an emerging pathogen and documented infections have been on the rise.
This yeast grows well at 35 degrees Celsius. It is susceptible to amphotericin B and flucytosine whenever there is an infection associated with it. Infections associated with Rhodotorula spp include skin infections (dermatitis), onychomycosis, meningitis, ocular infections, peritonitis, prosthetic joints, and dialysis-associated infections.
Morphologically, the yeast produces salmon, coral or pink-colored colonies that are mucoid on SAB dextrose agar. Microscopically, the budding yeasts are medium-to-large round-to-oval-to-elonaged in shape, and there are no hyphae or pseudohyphae.
Normally a ubiquitous organism, the saprophytic Rhodotorula spp discovered in 1985 by Harrison are common contaminants of the air, water, showerheads, soil, milk, and even fruit juice, however, they can cause opportunistic infections in patients at terminal stages of debilitating diseases such as cancer (leukemia or carcinoma in particular) or bacterial endocarditis. They have been recovered in the sputum, urine and blood. They are not a virulent spp.
According to the American Society for Microbiology (ASM) and the National Institute for Health (NIH), those who are immunosuppressed, have underlying health conditions, malignancies, who are on corticosteroids, cytotoxic drugs, broad spectrum antibiotics, or who have central intravenous catheters are at risk for infection with this organism. Prior to 1985, there were no known infections with this yeast, however, it is an emerging pathogen and documented infections have been on the rise.
This yeast grows well at 35 degrees Celsius. It is susceptible to amphotericin B and flucytosine whenever there is an infection associated with it. Infections associated with Rhodotorula spp include skin infections (dermatitis), onychomycosis, meningitis, ocular infections, peritonitis, prosthetic joints, and dialysis-associated infections.
Morphologically, the yeast produces salmon, coral or pink-colored colonies that are mucoid on SAB dextrose agar. Microscopically, the budding yeasts are medium-to-large round-to-oval-to-elonaged in shape, and there are no hyphae or pseudohyphae.
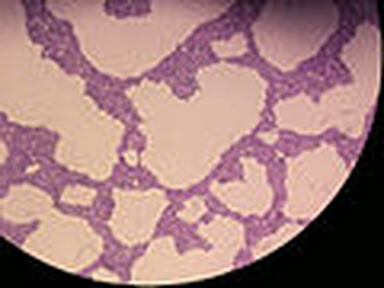
Rhodotorula are budding yeasts that are round or oval. Occasionally, a few pseudohyphae may be seen. Faint capsules may form.
|
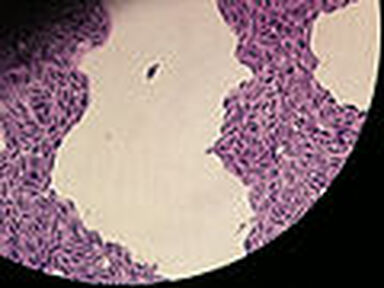
Budding yeasts of Rhodotorula measure 2-5.5 by 2.5-14 microns in diameter.
|
Rhodotorula muciliaginosa on SAB agar (coral-salmon color)
|

Rhodotorula spp rapidly grow and mature in 4 days as beautiful pink-to-coral-to-red-to-orange colonies on Cornmeal-Tween 80 agar. Colonies are yeastlike, smooth, moist, mucoid, and soft.
|

Rhodotorula rubra on SAB
|
Rhodotorula glutinis
|
saccharomyces:
Saccharomyces cerevisiae is a nonpathogenic yeast also known as "Brewer's Yeast". It is the yeast used to make bread, beer and wine. It has hardly been known to cause disease until recently, but there have been increasing cases of invasive infection and fungemia in immunocompromised or critically ill patients. Most patients who have gotten infected with this organism had taken a probiotic containing the yeast, in treatment for antibiotic-associated diarrhea, often cause by C. difficile.
Nosocomial infections have also occurred and has been assocated with contamination of the central vascular catheter hub or insertion-site contamination where it entered the bloodstream.
Colonies are moist, smooth, and white or cream-colored. In a wet mount, it produces large, oval budding cells.
Nosocomial infections have also occurred and has been assocated with contamination of the central vascular catheter hub or insertion-site contamination where it entered the bloodstream.
Colonies are moist, smooth, and white or cream-colored. In a wet mount, it produces large, oval budding cells.

|
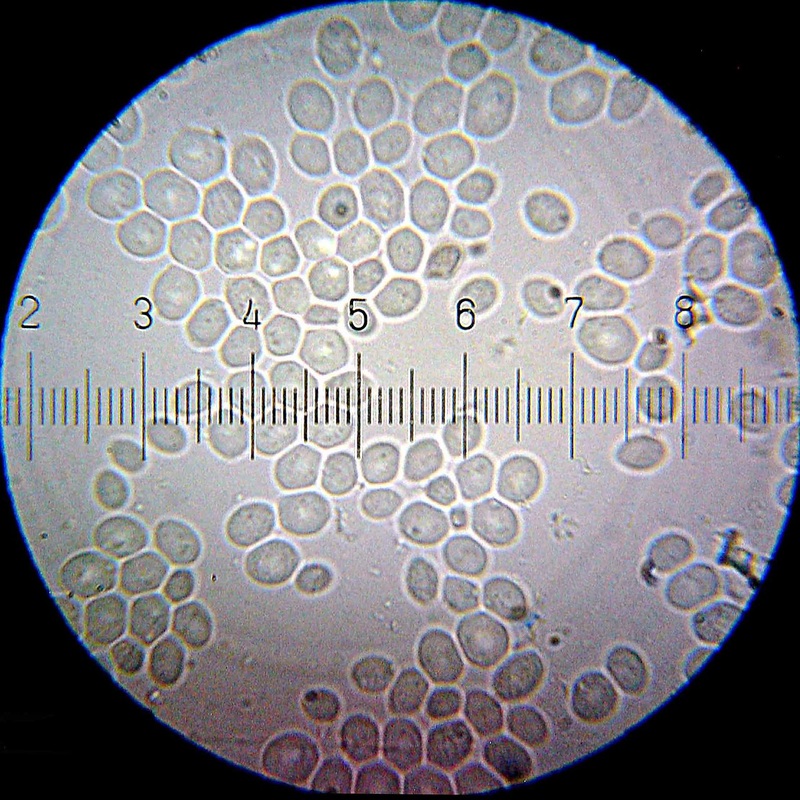
|
superficial mycoses: trichosporon spp:
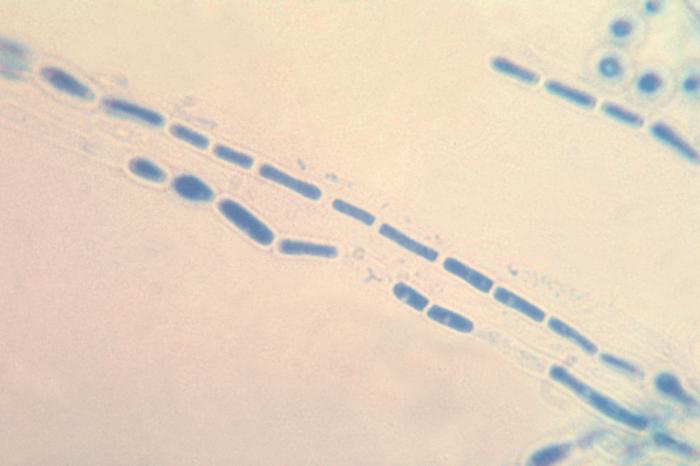
Arthroconidia and true hyphae and pseudohyphae bearing single blastoconidia in singles or short chains are seen
|

T. beigelii causes white piedra, which is a superfical ectothrix infection of the hair. Soft, white nodules form along the shafts of the hair of the beard and mustache, scalp or pubic region. Some strains are normal flora of teh skin, mouth and nails.
|
Geotrichum candidum:
This species causes geotrichosis, a rare infection that occasionally produces lesions in the lungs, vagina, mouth, intestines, skin, and is linked to fungemia and disseminated infection in immunocompromised patients.
Colonies mature within 5 days and produce white, moist, yeast-like colonies surrounded by hyphae at the periphery. This is known as "ground glass" appearance.
Microscopic morphology reveals arthroconidia that fragment from true hyphae, and they are rectangle-shaped arthroconidia.
This species causes geotrichosis, a rare infection that occasionally produces lesions in the lungs, vagina, mouth, intestines, skin, and is linked to fungemia and disseminated infection in immunocompromised patients.
Colonies mature within 5 days and produce white, moist, yeast-like colonies surrounded by hyphae at the periphery. This is known as "ground glass" appearance.
Microscopic morphology reveals arthroconidia that fragment from true hyphae, and they are rectangle-shaped arthroconidia.
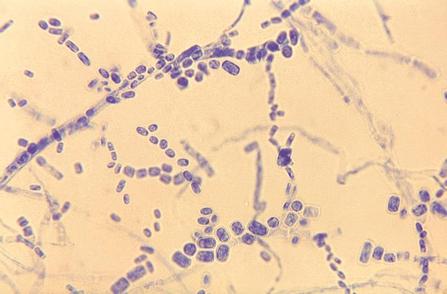
No pseudohyphae are formed, only true hyphae (coarse) that break apart into rectangle-shaped arthroconidia. They are "barrel-shaped".
|
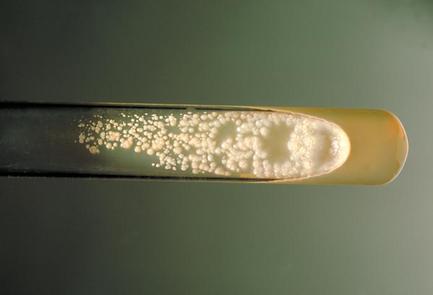
Colonies rapidly mature in 4 days as white, moist, yeast-like, with a "ground glass" appearance
|
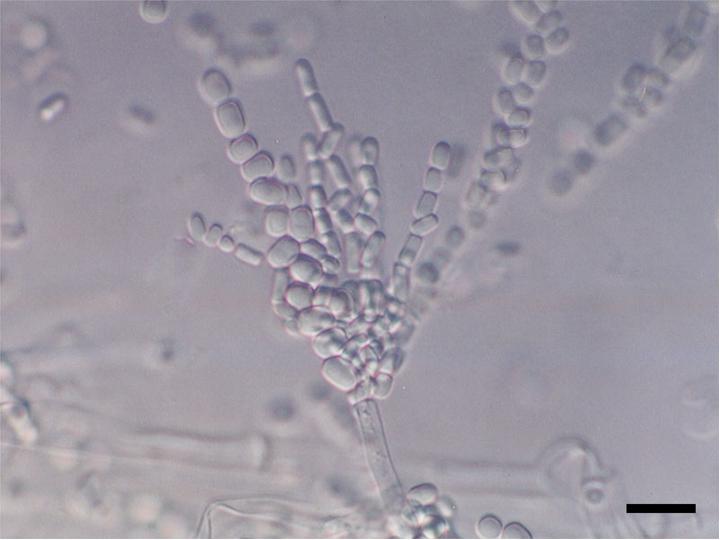
|

|

https://upload.wikimedia.org/wikipedia/commons/thumb/7/7d/Geotrichium_candidum.jpg/800px-Geotrichium_candidum.jpg
|
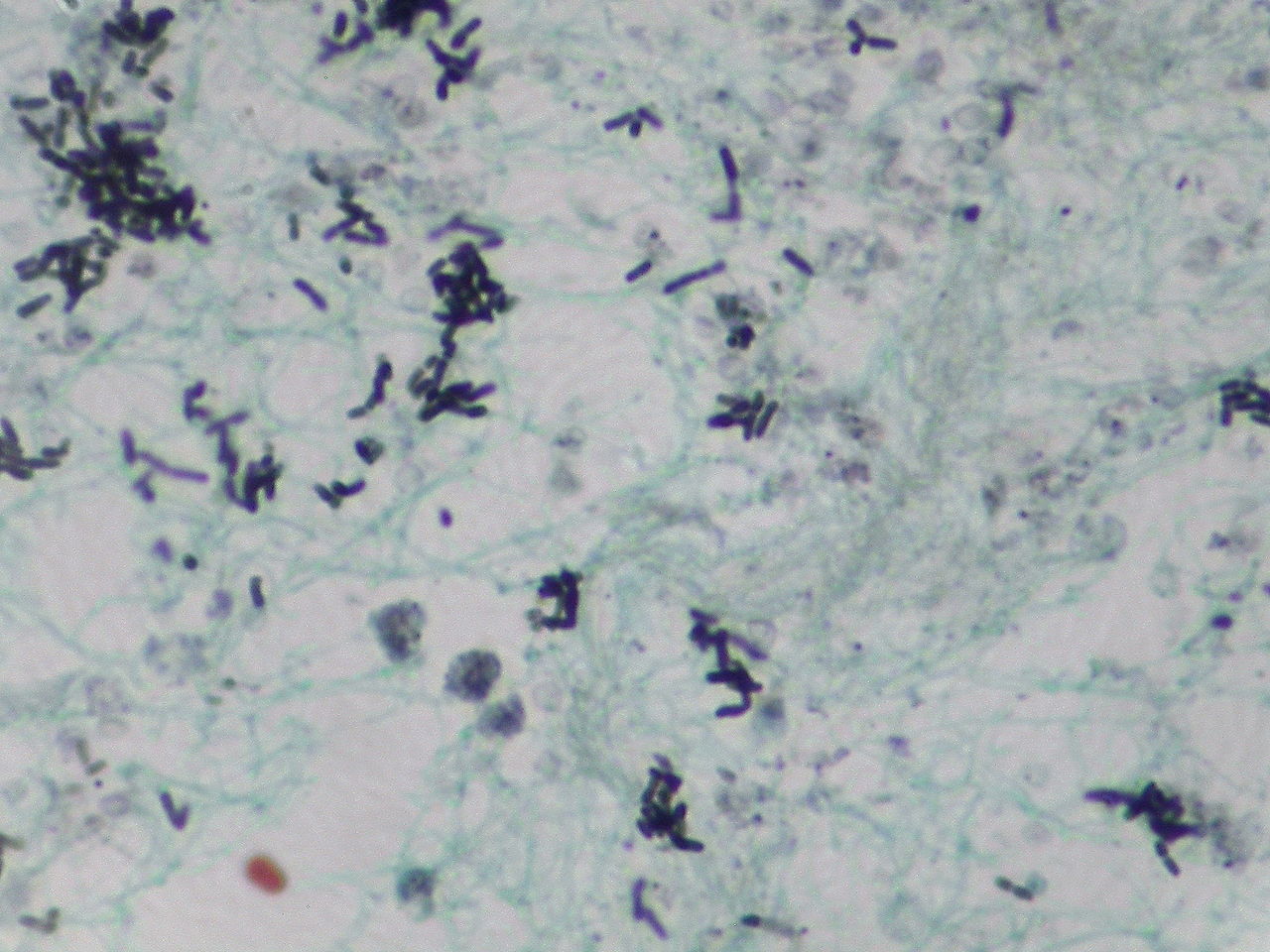
https://upload.wikimedia.org/wikipedia/commons/thumb/d/d3/Geotrichosis_Case_151%282%29.jpg/1280px-Geotrichosis_Case_151%282%29.jpg
|
subcutaneous mycoses:
Subcutaneous organisms include dematiaceous molds, hyaline molds, and funguslike bacteria. These molds are often slow-growers, taking up to 3-4 weeks to develop, so these should be held for at least a month. Identification is primarily microscopic morphology.
Subcutaneous mycoses are those that occur when the skin is accidentally punctured with a splinter, thorn, or other material that is contaminated with soil fungi. At first, a local infection forms, which forms at the skin, spreading to the underlying tissue, and then the lymph nodes. Every once in awhile, it will spread, but most of the time, this is a local infection.
Subcutaneous lesions form, which become chronic, not healing, hard, lumpy, crusted over, and even ulcerated, exuding fluid and/or pus. The most common extremity affected is the foot. Since these organisms are ubiquitous, they are found worldwide. Since they can invade tissues, histology and cytology preparations are also looked at in addition to mycology specimens from the microbiology lab.
Samples should come from active lesions, and if any granules or black dots are seen, they should also be included. Any oozing fluid or pus should be collected and sent for analysis as well.
Macroscopic and microscopic exams should include colony descriptions, granule descriptions, and microscopic morphology and color. Histology stains and KOH potassium hydroxide wet mounts from suspected chromoblastomycosis will reveal thick-walled, dark brown, round sclerotic bodies resembling copper pennies. They will also have cross-walls. Granules from suspected mycetoma will either be pigmented hyphae with chlamydoconidia, or club-shaped granules.
Granules should be rinsed several times with sterile saline or sterile water to remove cell debris and contamination, then be crushed and plated to SABHI with and without antibiotics.
Subcutaneous mycoses are those that occur when the skin is accidentally punctured with a splinter, thorn, or other material that is contaminated with soil fungi. At first, a local infection forms, which forms at the skin, spreading to the underlying tissue, and then the lymph nodes. Every once in awhile, it will spread, but most of the time, this is a local infection.
Subcutaneous lesions form, which become chronic, not healing, hard, lumpy, crusted over, and even ulcerated, exuding fluid and/or pus. The most common extremity affected is the foot. Since these organisms are ubiquitous, they are found worldwide. Since they can invade tissues, histology and cytology preparations are also looked at in addition to mycology specimens from the microbiology lab.
Samples should come from active lesions, and if any granules or black dots are seen, they should also be included. Any oozing fluid or pus should be collected and sent for analysis as well.
Macroscopic and microscopic exams should include colony descriptions, granule descriptions, and microscopic morphology and color. Histology stains and KOH potassium hydroxide wet mounts from suspected chromoblastomycosis will reveal thick-walled, dark brown, round sclerotic bodies resembling copper pennies. They will also have cross-walls. Granules from suspected mycetoma will either be pigmented hyphae with chlamydoconidia, or club-shaped granules.
Granules should be rinsed several times with sterile saline or sterile water to remove cell debris and contamination, then be crushed and plated to SABHI with and without antibiotics.
Cladosporium and Cladophialophora spp:
This dematiaceous mold causes chromoblastomycosis if the case is a true infection, otherwise, this is one of the most common indoor and outdoor molds. It can result in sinus infection, pulmonary allergic asthma, or a nail infection.
Cladosporium spp and Cladophialophora spp may initially appear as black yeasts on SABHI agar, but then later form velvety, short, aerial hyphae and conidia. They contain the pigment melanin, making them dark and dangerous. They are found everywhere, and can colonize cactus, cactus needles, wood, pine trees and pine cones, eucalyptus, and soil. A prick with one of these organisms can cause human infection, resulting in crusty subcutaneous lesions or cauliflower-like nodes that look like tumors, or scaly plaques or granulomas.
Cladosporium carrionii was renamed to Cladophialophora carrionii in 1980 by Dante' Borelli. Both molds are from the family Herpotrichiellaceae, and there are about 35 species.
Cladophialophora carrionii:
Macroscopic Exam:
Microscopic Exam:
Cladophialophora bantianum:
This organism is very dangerous, because it not only causes subcutaneous disease, but it can also cause cerebral infection in humans. For this reason, it should always be treated with caution. ALWAYS work under a biological hood and NEVER set up slide cultures if this is suspected.
Macroscopic Exam:
Microscopic Exam:
This dematiaceous mold causes chromoblastomycosis if the case is a true infection, otherwise, this is one of the most common indoor and outdoor molds. It can result in sinus infection, pulmonary allergic asthma, or a nail infection.
Cladosporium spp and Cladophialophora spp may initially appear as black yeasts on SABHI agar, but then later form velvety, short, aerial hyphae and conidia. They contain the pigment melanin, making them dark and dangerous. They are found everywhere, and can colonize cactus, cactus needles, wood, pine trees and pine cones, eucalyptus, and soil. A prick with one of these organisms can cause human infection, resulting in crusty subcutaneous lesions or cauliflower-like nodes that look like tumors, or scaly plaques or granulomas.
Cladosporium carrionii was renamed to Cladophialophora carrionii in 1980 by Dante' Borelli. Both molds are from the family Herpotrichiellaceae, and there are about 35 species.
Cladophialophora carrionii:
Macroscopic Exam:
- On SABHi agar at room temperature, this organism is a slow-grower, producing black colonies with dark, velvety mycelium.
- It does not grow at 42 degrees Celsius.
- It does not have neutropenic propensity.
- It causes chromoblastomycosis.
Microscopic Exam:
- It produces hyphae that are dark with long or short conidiophores that support repeatedly branching short chains of oval-shaped blastoconidia.
Cladophialophora bantianum:
This organism is very dangerous, because it not only causes subcutaneous disease, but it can also cause cerebral infection in humans. For this reason, it should always be treated with caution. ALWAYS work under a biological hood and NEVER set up slide cultures if this is suspected.
Macroscopic Exam:
- On SABHI agar at room temperature, this organism produces a black, compact colony with a black reverse. It grows quickly, as opposed to the other strain listed above.
- It grows well at 42 degrees Celsius.
Microscopic Exam:
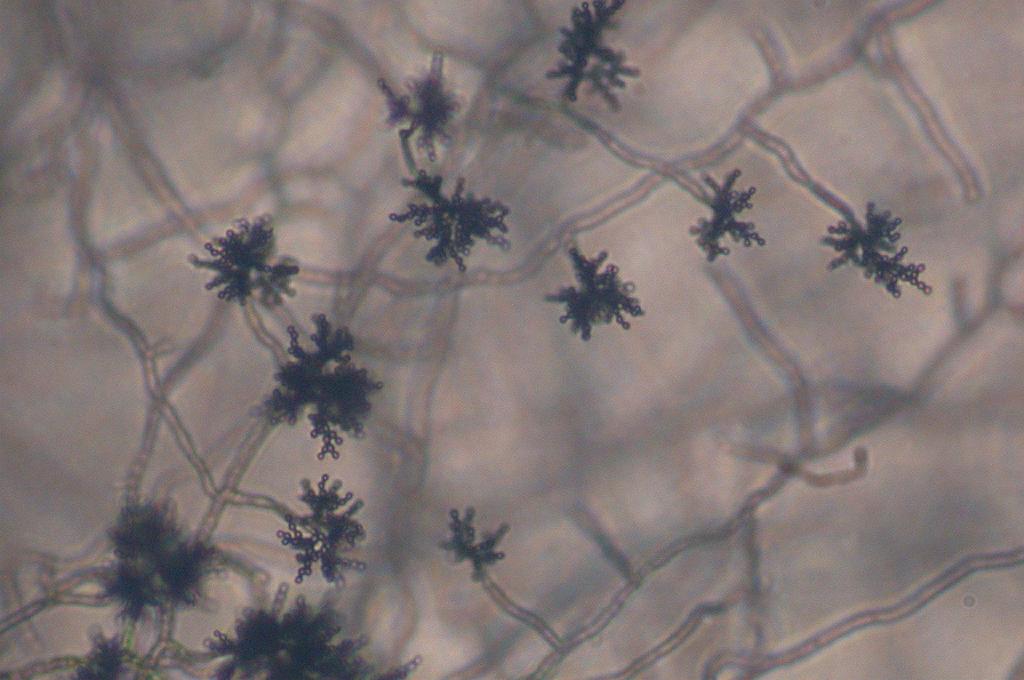
This species produces dark, septate hyphae that bear lateral and terminal conidiophores. Conidiophores produce long, branching chains of conidia that are dark brown, smooth, round-to-oval shaped that easily disperse.
|
Colonies grow as dark, olive green to gray green to brown, velvety, flat colonies with a slightly raised center. The reverse is black.
|
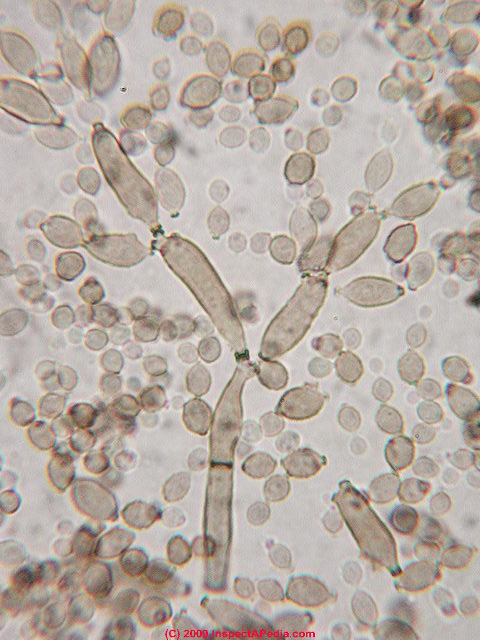
|

|
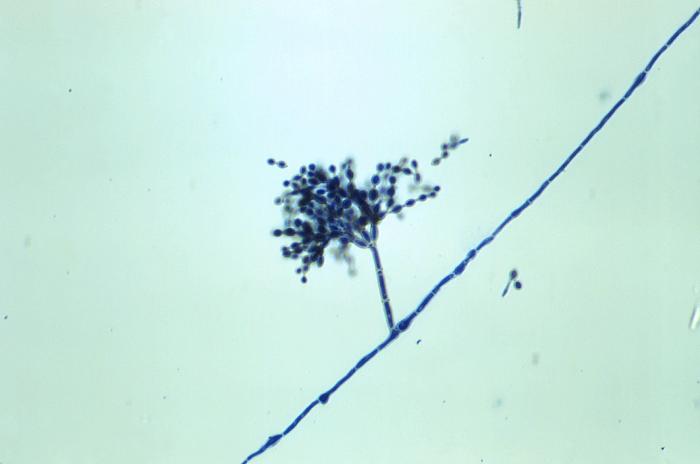
Exophiala spp: (Dematiaceous Mold)
Exophiala spp was discovered in 1966 by J.W. Carmichael. This fungus can cause infection in woodwind instrumental players who play on a contaminated woodwind instrument, such as a saxophone, clarinet, oboe or flute. It results in an allergic pulmonary disease or hypersensitivity pneumonitis or "Saxophone Lung".
- Causes mycetoma and phaeohyphomycosis, which manifests as invasive sinusitis, nodules under the skin, abscesses, osteomyelitis, keratitis, lung mass, mycotic arthritis, endocarditis, brain abscess, or dissimenated infection
- Predisposed individuals: immunocompromised, surgery, medications, transplants, diabetes mellitus
Exophiala spp was discovered in 1966 by J.W. Carmichael. This fungus can cause infection in woodwind instrumental players who play on a contaminated woodwind instrument, such as a saxophone, clarinet, oboe or flute. It results in an allergic pulmonary disease or hypersensitivity pneumonitis or "Saxophone Lung".
- E. werneckii results in an infection of the skin known as tinea nigra.
- E. jeanselmei can cause an infection called maduromycosis or black grain mycetoma, and can also cause phaeohyphomycosis.
- E. xenobiotica is a segretative subtype of E. jeanselmei and is associated with the infections listed above. It has less melanized conidiogenous cells under the microscopic examination.
- E. dermatitidis was formerly known as Wangiella dermatitidis. It is linked to phaeohyphomycosis and can infect the central nervous system, leading to infections of the brain, lungs, eyes, cutaneous and subcutaneous tissue.
- E. hortaea is now known as Hortaea werneckii. It is linked to tinea nigra, a superficial fungal infection of the skin. It is usually seen on the palms of the hands and looks like a "birthmark" because it is flat, smooth, not scaly, and is irregular. It is more common in tropical areas of the world, and rare in the USA.

Hortaea werneckii

E. dermatitidis
|
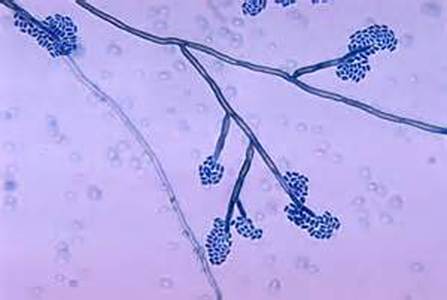
E. jeanselmei is a slow-grower (14 days) at 25-30 degrees Celsius. Colonies are brown-black or green-black and velvety with a black reverse. Numerous yeast-like budding cells are born on slender annellides on septate hyphae. The oval-shaped conidia are born in clusters at the terminal ends and sides of the conidiophores.
|

Classic Exophiala jeanselmei spp complex in lactophenol cotton blue stain
Exophiala werneckii is a dimorphic yeast/mold that, in yeast form, produces dark brown-to-olive-to-black, moist colonies on SAB dextrose and PDA agar. In mold form, it produces mycelium, which resemble "feet" on the agar, giving colonies a fuzzy appearance.

Tinea nigra
|

Tinea nigra is a skin infection caused by this organism, which invades only the superficial skin, and resembles a birthmark.
|
Exophiala xenobiotica:
Images taken by Jeanette Reynolds, MS-Biology, M-ASCP, MT-AMT (recovered from a finger wound)
- Black yeast (dematiaceous)
- At 37 degrees: Olive-to-black mold form (matte, heaped, fuzzy perimeter)-grows slowly
- At 25 degrees (Room Temp): Black yeast form (creamy, shiny, flat to wrinkled, soft)-grows really well and faster
- Black reverse
- Identification confirmed by the U. of TX Health Sciences
Images taken by Jeanette Reynolds, MS-Biology, M-ASCP, MT-AMT (recovered from a finger wound)
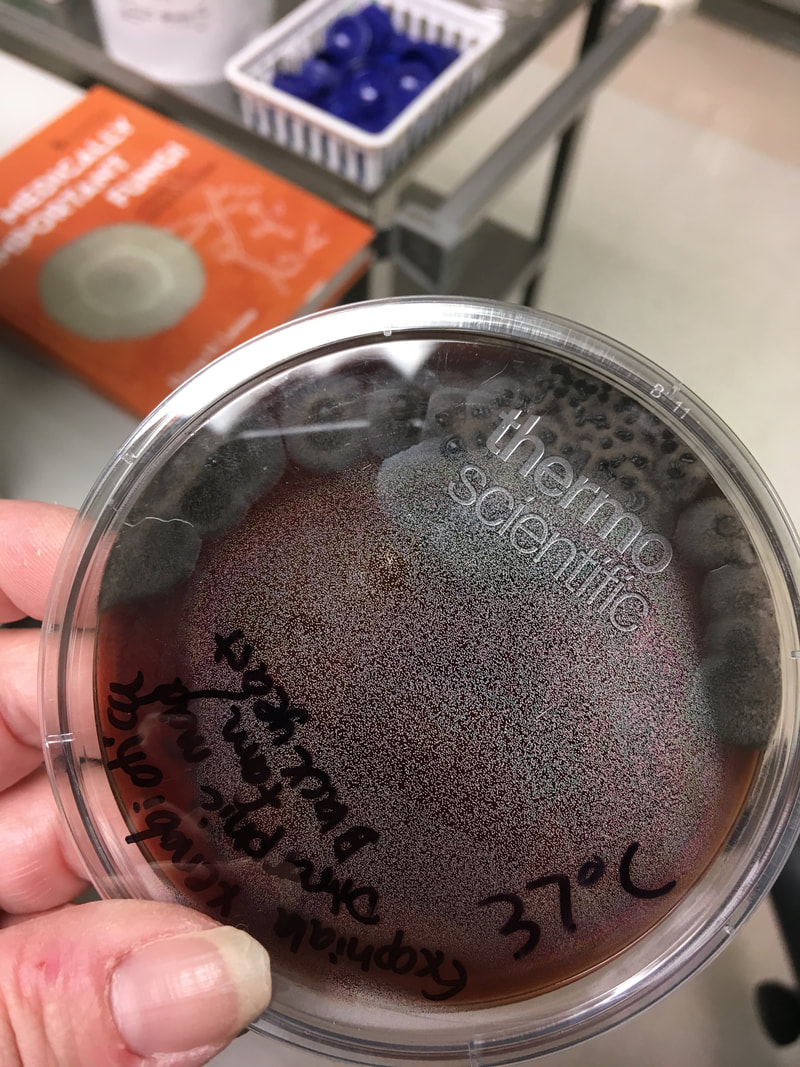
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
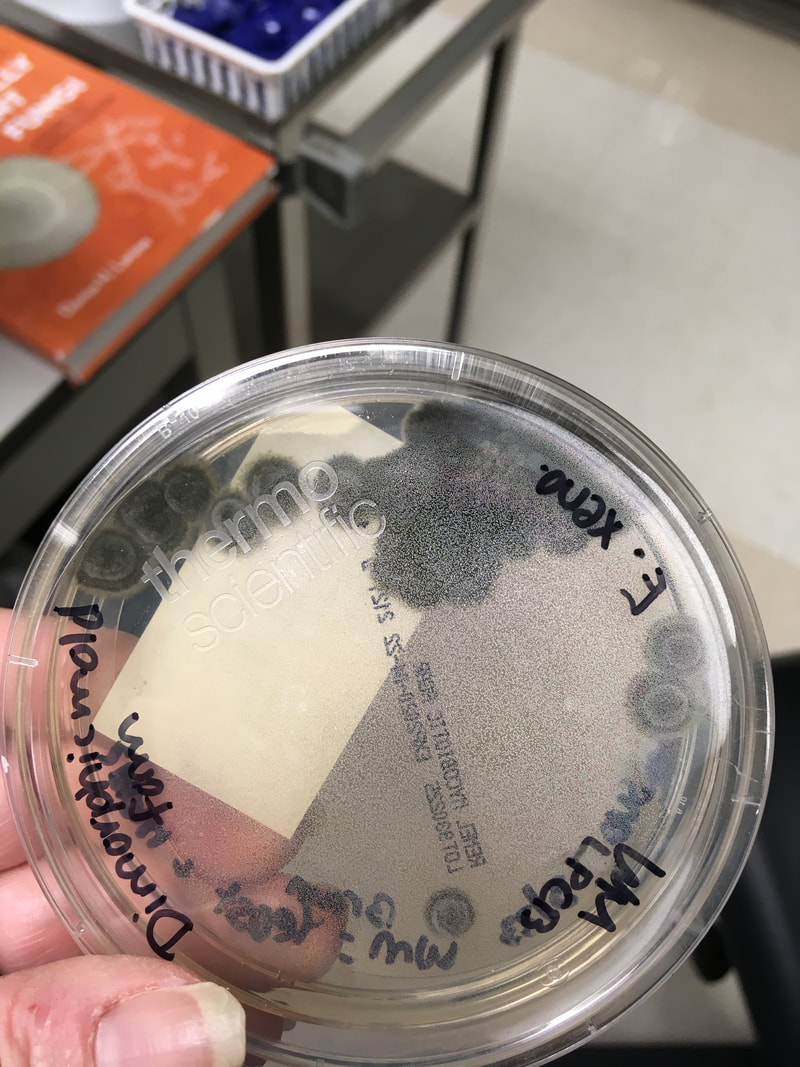
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
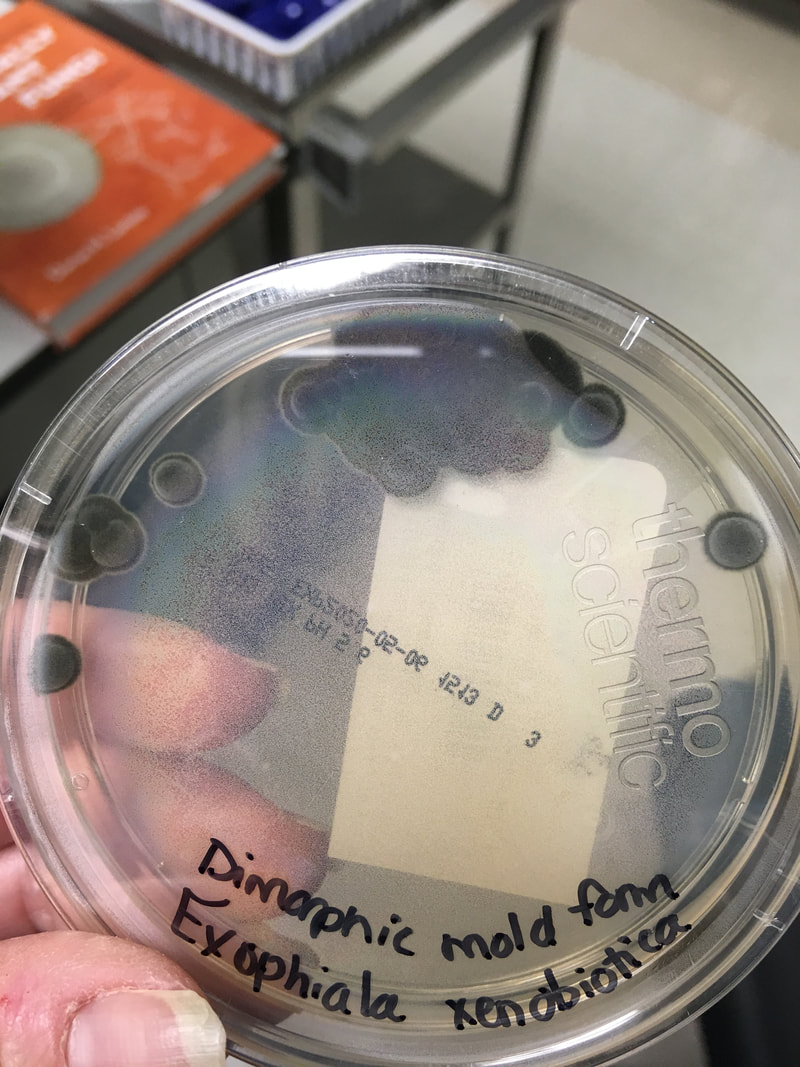
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
Image by Jeanette Reynolds, MLS-AMT, M-ASCP, MS-Biology, Certified in Emerging Diseases, Certified Instructor
|
Fonsecaeae spp:
Fonsecaea compacta:
This organism causes chromoblastomycosis, and is the most common cause of it. Lesions develop in the subcutaneous tissues on the lower extremities. Rarely, it has been linked to internal infections.
Macroscopic Exam:
Microscopic Exam:
Fonsecaea pedrosoi:
This organism can cause chromoblastomycosis OR systemic phaeohyphomycosis.
Macroscopic Exam:
Microscopic Exam:
Fonsecaea compacta:
This organism causes chromoblastomycosis, and is the most common cause of it. Lesions develop in the subcutaneous tissues on the lower extremities. Rarely, it has been linked to internal infections.
Macroscopic Exam:
- On SABHI at room temperature, it is a very slow-grower, and it will grow small black colonies with very low, dark, velvety mycelium.
Microscopic Exam:
- It produces dark hyphae with primary blastoconidia at the tips of the conidiophores, each one supporting 1-4 secondary blastoconidia, which may also produce 1-4 tertiary conidia.
- The blastoconidia resemble compact conidial heads in four different formations:
- Closely compact with loosely organized blastoconidia, resembling vases with flowers
- Chains of oval-shaped blastoconidia on branched conidiphores, resembling Cladosporium spp, Cladophialophora spp
- Bottle-brush resemblance of oval-shaped blastoconidia attached to the conidiophore
- Resembling one vase with flowers of oval-shaped blastoconidia
Fonsecaea pedrosoi:
This organism can cause chromoblastomycosis OR systemic phaeohyphomycosis.
Macroscopic Exam:
- On SABHI at room temperature, colonies are slow-growers, revealing a black colony with low black or dark olive aerial mycelium.
Microscopic Exam:
- It produces dark hyphae with primary blastoconidia at the tips of the conidiophores, each one supporting 1-4 secondary blastoconidia, which may also produce 1-4 tertiary conidia.
- The blastoconidia resemble compact conidial heads in four different formations:
- Closely compact with loosely organized blastoconidia, resembling vases with flowers
- Chains of oval-shaped blastoconidia on branched conidiphores, resembling Cladosporium spp, Cladophialophora spp
- Bottle-brush resemblance of oval-shaped blastoconidia attached to the conidiophore
- Resembling one vase with flowers of oval-shaped blastoconidia
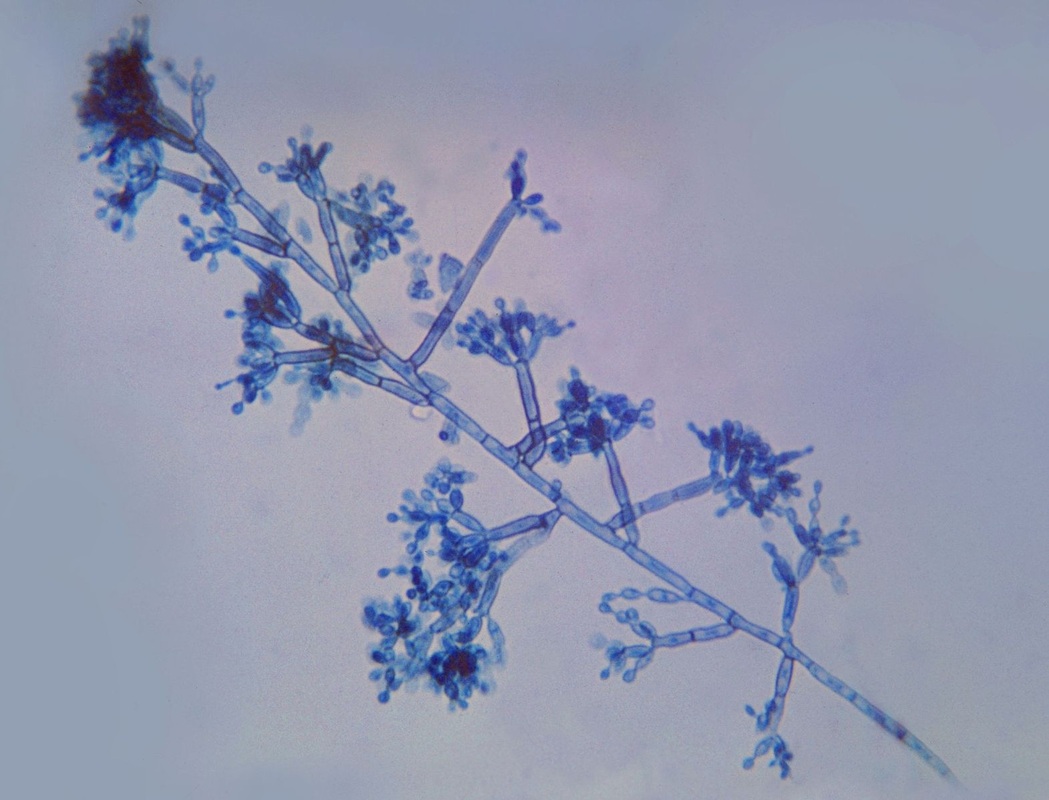
F. compacta: As seen here, septate hyphae that are branched bear conidiophores that produce short chains and clusters of round-to-oval conidia.
|
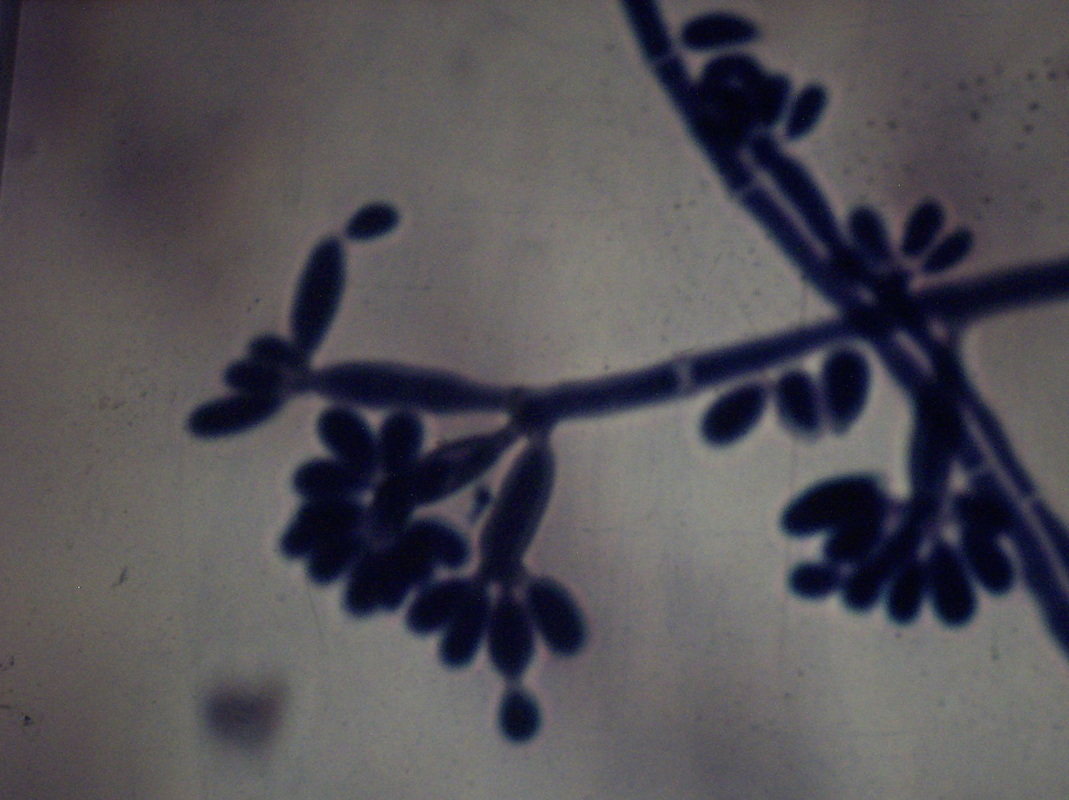
F. pedrosoi: As seen in the image here, hyphae are septate, branched, with dark, oval-shaped conidia born on conidiophores with swollen denticles that bear the primary, single-celled conidia
|
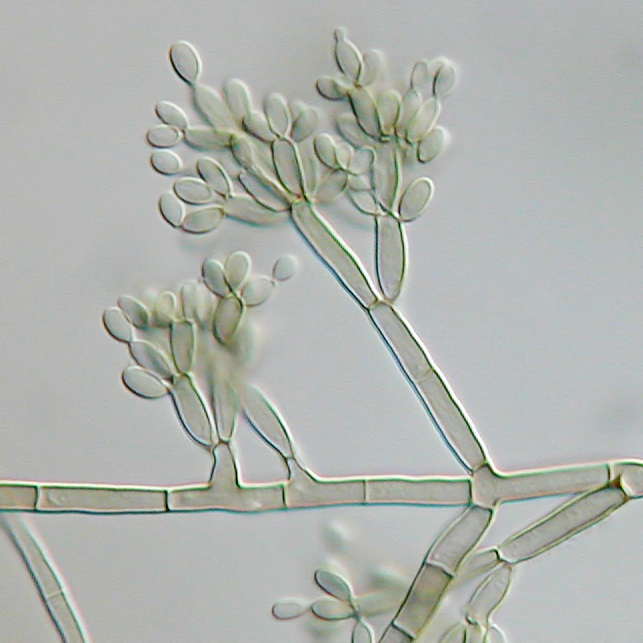
Phialophora spp:
This organism causes chromoblastomycosis (2nd most common cause) worldwide, and is the most common cause of it in North America. It also causes phaeohyphomycosis and occasionally, mycetoma.
Phialophora verrucosa:
It causes chromoblastomycosis, subcutaneous phaeohyphomycosis, and keratomycosis.
Macroscopic Exam:
Microscopic Exam:
Phialophora jeanselmei:
It causes mycetoma, subcutaneous and systemic phaeohyphomycosis and keratomycosis.
Macroscopic Exam:
Phialophora Exophiala (Wangiella):
It causes phaeohyphomycosis.
Macroscopic Exam:
This organism causes chromoblastomycosis (2nd most common cause) worldwide, and is the most common cause of it in North America. It also causes phaeohyphomycosis and occasionally, mycetoma.
Phialophora verrucosa:
It causes chromoblastomycosis, subcutaneous phaeohyphomycosis, and keratomycosis.
Macroscopic Exam:
- It produces a slow-growing black colony with matted dark mycelium.
Microscopic Exam:
- It produces dark hyphae with flask-shaped phialides that have a cup-shaped collarette with terminal balls of oval-shaped phialoconidia.
Phialophora jeanselmei:
It causes mycetoma, subcutaneous and systemic phaeohyphomycosis and keratomycosis.
Macroscopic Exam:
- It produces a black yeast that gradually develops dark velvety mycelium.
- It produces dark budding yeasts, but with age, annellides on annellophores will be seen producing clusters of oval annelloconidia at the tips.
Phialophora Exophiala (Wangiella):
It causes phaeohyphomycosis.
Macroscopic Exam:
- Colonies are shiny black and yeast-like at first, but gradually develop dark velvety mycelium at the periphery.
- Dark budding yeasts are observed at first, but with age, a few tube-like phialides will be seen without collarettes and with terminal balls of conidia that may resemble bottle brushes.

P. verrucosa consists of dark brown, branched, septate hyphae bearing vase-shaped phialides with flared, cuplike collarettes bearing round-to-oval conidia. This species resembles a vase full of flowers.
|

|
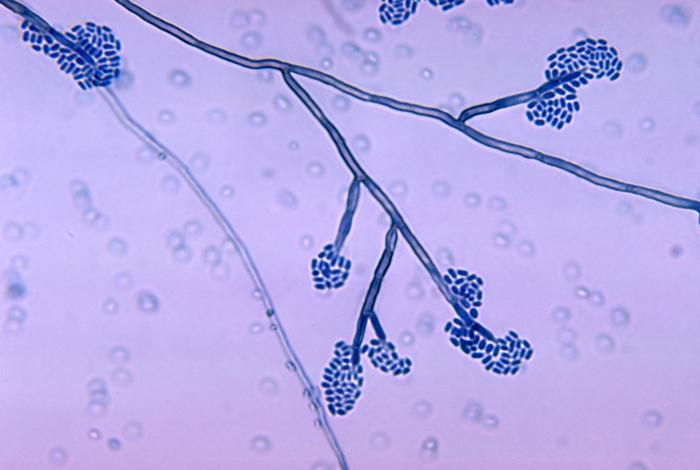
Wangiella dermatiditis:
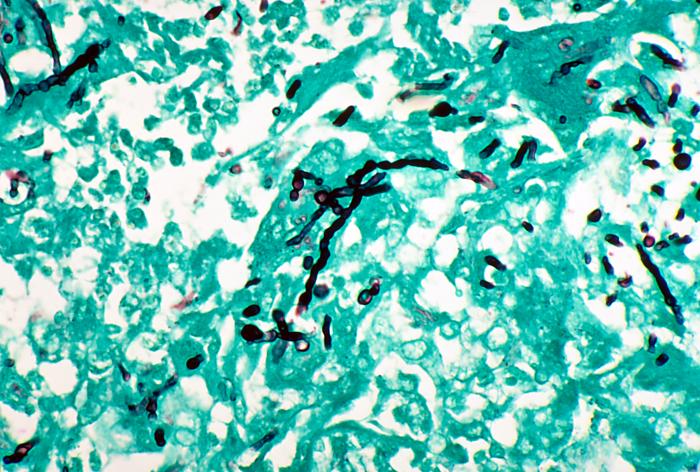
W. dermatitidis found in the tissues and stained with silver stain. It causes phaeohyphomycosis and causes central nervous system infections (brain), eye infections, and cutaneous and subcutaneous tissue infections.
Scedosporium spp:
Scedosporium is an opportunistic pathogen and is a causative agent of invasive arthritis or osteomyelitis with joint and/or bone infection, localized and disseminated infections that are often resistant to antifungals. Most infections occur in individuals are are immunosuppressed or immunocompromised. Infections can be fatal if they become systemic.
The conidia are oval/lemon-shaped and sit on a swollen base somewhat resembling a vase.
On the plate, colonies are grey-brown and resemble a cobweb or a moth-eaten wool garment. This is more of a slow-grower, often requiring around 4 weeks to grow.
This is a soil fungus, which is one reason why hospitals discourage the bringing or harboring of plants or flowers in patient rooms. Traumatic injury from splinters or thorns is the most common cause of infection with this organism.
Scedosporium is an opportunistic pathogen and is a causative agent of invasive arthritis or osteomyelitis with joint and/or bone infection, localized and disseminated infections that are often resistant to antifungals. Most infections occur in individuals are are immunosuppressed or immunocompromised. Infections can be fatal if they become systemic.
The conidia are oval/lemon-shaped and sit on a swollen base somewhat resembling a vase.
On the plate, colonies are grey-brown and resemble a cobweb or a moth-eaten wool garment. This is more of a slow-grower, often requiring around 4 weeks to grow.
This is a soil fungus, which is one reason why hospitals discourage the bringing or harboring of plants or flowers in patient rooms. Traumatic injury from splinters or thorns is the most common cause of infection with this organism.

Septate hyphae bear unbranched conidigenous cells called "annellides", which have a swollen base and an elongated neck with small clusters of conidia at the tip
|

The rose-like/flower-like growth pattern of Scedosporium spp
|
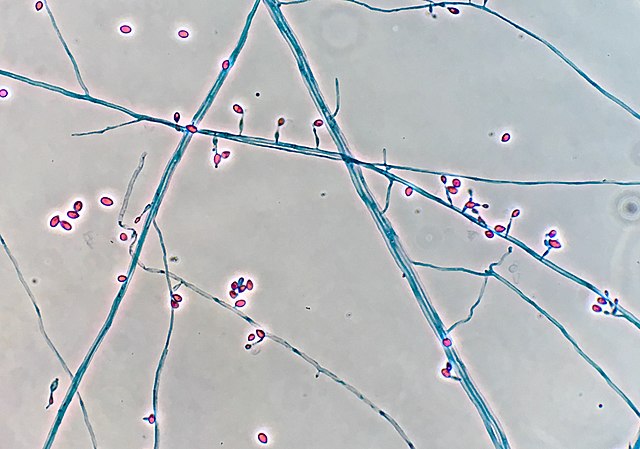
https://upload.wikimedia.org/wikipedia/commons/thumb/8/8e/Lomentospora_Family_Portrait.jpg/640px-Lomentospora_Family_Portrait.jpg
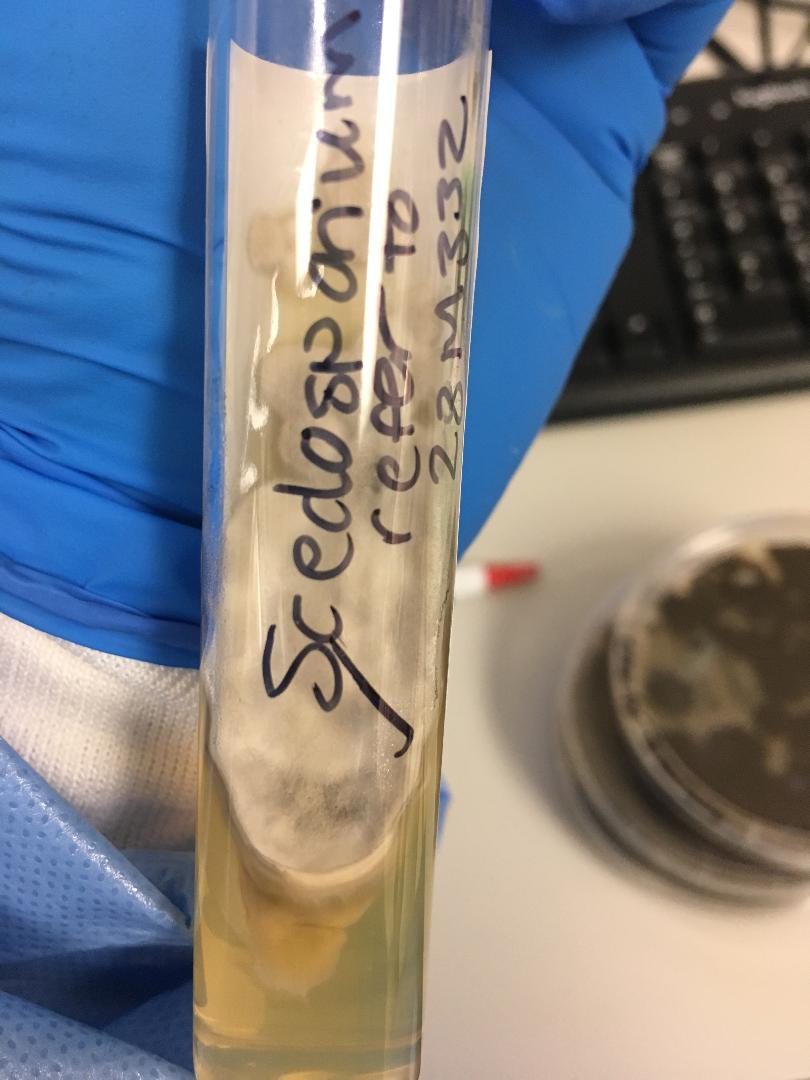
Scedosporium spp grown and taken by Jeanette Reynolds, MLS-AMT, M-ASCP.
|

Scedosporium spp grown and taken by Jeanette Reynolds, MLS-AMT, M-ASCP.
|
Scedosporium spp grown and taken by Jeanette Reynolds, MLS-AMT, M-ASCP.
Sporothrix schenckii:
In 1896, a medical student named Benjamen Schenk discovered this fungus, which causes sporotrichosis, which is a chronic infection that starts out as skin lesions that progresses to the subcutaneous tissue, invades the lymphatic system and nodes, and spreading throughout the bloodstream and skeletal system.
Chronic alcoholics are particularly at risk for infection. Initial lesions are often caused by accidental traumatic entry into the skin, such as through rose thorn pricks by contaminated plants when gardening without gloves. "Sporotrichosis" is also known as the "rose handler's disease". It can also be transmitted via cat bites or scratches. It is thermally dimorphic, meaning it is a yeast in host tissue and a mold at room temp. Remember the following for thermally dimorphic species: "Mold in the cold; Yeast in the heat".
On the plate, colonies appear as cream to dark brown and are moist. Septate hyphae bear oval-shaped conidia. On SAB agar, the yeast form appears as white to creamy white colonies and microscopially as "cigar-shaped" elongated yeast cells.
In 1896, a medical student named Benjamen Schenk discovered this fungus, which causes sporotrichosis, which is a chronic infection that starts out as skin lesions that progresses to the subcutaneous tissue, invades the lymphatic system and nodes, and spreading throughout the bloodstream and skeletal system.
Chronic alcoholics are particularly at risk for infection. Initial lesions are often caused by accidental traumatic entry into the skin, such as through rose thorn pricks by contaminated plants when gardening without gloves. "Sporotrichosis" is also known as the "rose handler's disease". It can also be transmitted via cat bites or scratches. It is thermally dimorphic, meaning it is a yeast in host tissue and a mold at room temp. Remember the following for thermally dimorphic species: "Mold in the cold; Yeast in the heat".
On the plate, colonies appear as cream to dark brown and are moist. Septate hyphae bear oval-shaped conidia. On SAB agar, the yeast form appears as white to creamy white colonies and microscopially as "cigar-shaped" elongated yeast cells.

Microscopically, this fungus produces hyphae that are thin and narrow, septate, branching, with conidiphores that taper and bear numerous small, pear-shaped conidia in clusters.
|
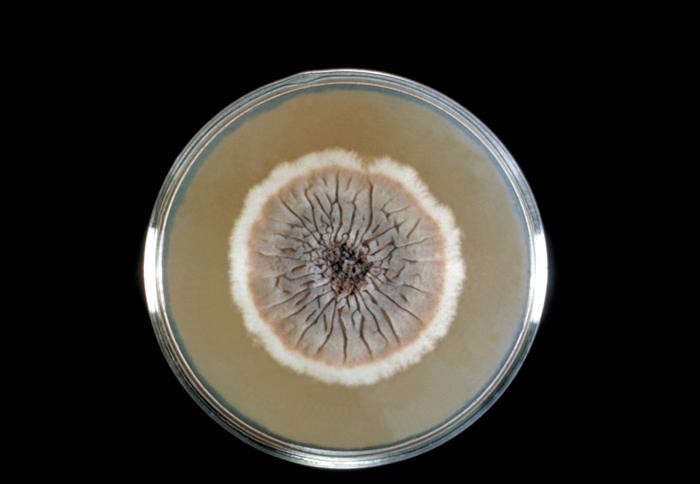
This thermally dimorphic fungus rapidly matures in 4 days and grows as small, white colonies maturing to moist, wrinkled, leathery, velvety, dark brown-to-black colonies.
|
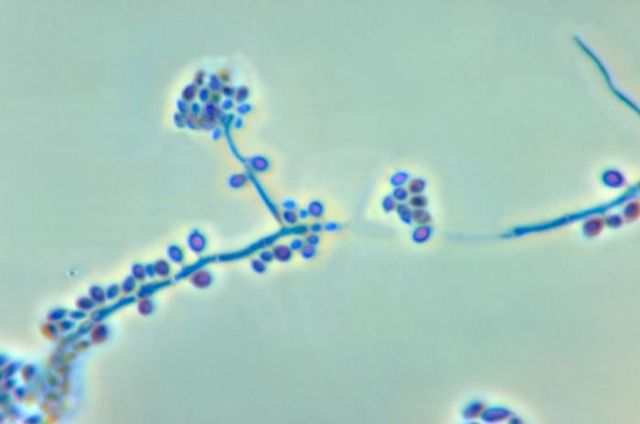
https://upload.wikimedia.org/wikipedia/commons/thumb/a/ac/Conidiophores_and_conidia_of_the_fungus_Sporothrix_schenckii_PHIL_4208_lores.jpg/640px-Conidiophores_and_conidia_of_the_fungus_Sporothrix_schenckii_PHIL_4208_lores.jpg
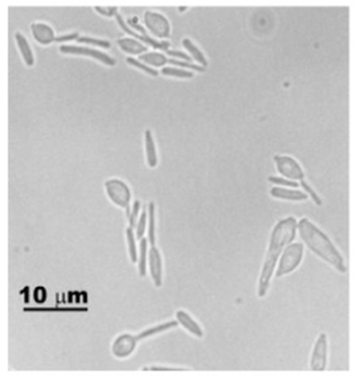
Saline wet mount of S. schenckii reveals elongated cigar-shaped yeast cells
fungus-like bacteria:
Fungus-like bacteria are true bacteria that resemble fungi, so we discuss them here in order to be able to differentiate them from true fungi. Additionally, these are often found growing in and on the media we use in the mycology and mycobacteriology laboratory sections, so the testing is very similar.
They fall under the bacterial subdivision Schizomycota, and under the order Actinomycetales. The actinomycetes are the umbrella term for all Actinomycetales except the Mycobacteriales (AFB).
Colonies and thin, microscopic filaments branch, produce conidia, and cause mycotic-like diseases, similar to fungi. There are two types of actinomycetes: anaerobic and aerobic. Here, we focus on the aerobic actinomycetes, and there are four of them:
They fall under the bacterial subdivision Schizomycota, and under the order Actinomycetales. The actinomycetes are the umbrella term for all Actinomycetales except the Mycobacteriales (AFB).
Colonies and thin, microscopic filaments branch, produce conidia, and cause mycotic-like diseases, similar to fungi. There are two types of actinomycetes: anaerobic and aerobic. Here, we focus on the aerobic actinomycetes, and there are four of them:
- Actinomadura spp
- Nocardia spp
- Nocardiopsis spp
- Streptomyces spp
Actinomyces spp:
This is an anaerobic actinomycete bacteria that causes actinomycosis. Because it is an anaerobe, it has been associated with dental infections of the tooth (deep), abscesses, and deep systemic infections. It is found in wound infections with mixed bacteria.
It is a Gram-positive, short bacillus that branches and forms spider-like clusters. On media, colonies are white with ruffled edges, resembling pot pies or fried eggs. Some colonies appear "tooth-like" and resemble a molar tooth. This organism is NOT acid-fast and it grows in 7-10 days in 37 degrees Celsius with 5% CO2. It grows in THIO broth, resembling bread crumbs.True infections produce sulfur-colored granules in some strains. This bacterium is catalase positive, which will produce bubbling.
Some strains are normal flora found in the mouth, in saliva, and in the tonsillar crypts.
This is an anaerobic actinomycete bacteria that causes actinomycosis. Because it is an anaerobe, it has been associated with dental infections of the tooth (deep), abscesses, and deep systemic infections. It is found in wound infections with mixed bacteria.
It is a Gram-positive, short bacillus that branches and forms spider-like clusters. On media, colonies are white with ruffled edges, resembling pot pies or fried eggs. Some colonies appear "tooth-like" and resemble a molar tooth. This organism is NOT acid-fast and it grows in 7-10 days in 37 degrees Celsius with 5% CO2. It grows in THIO broth, resembling bread crumbs.True infections produce sulfur-colored granules in some strains. This bacterium is catalase positive, which will produce bubbling.
Some strains are normal flora found in the mouth, in saliva, and in the tonsillar crypts.
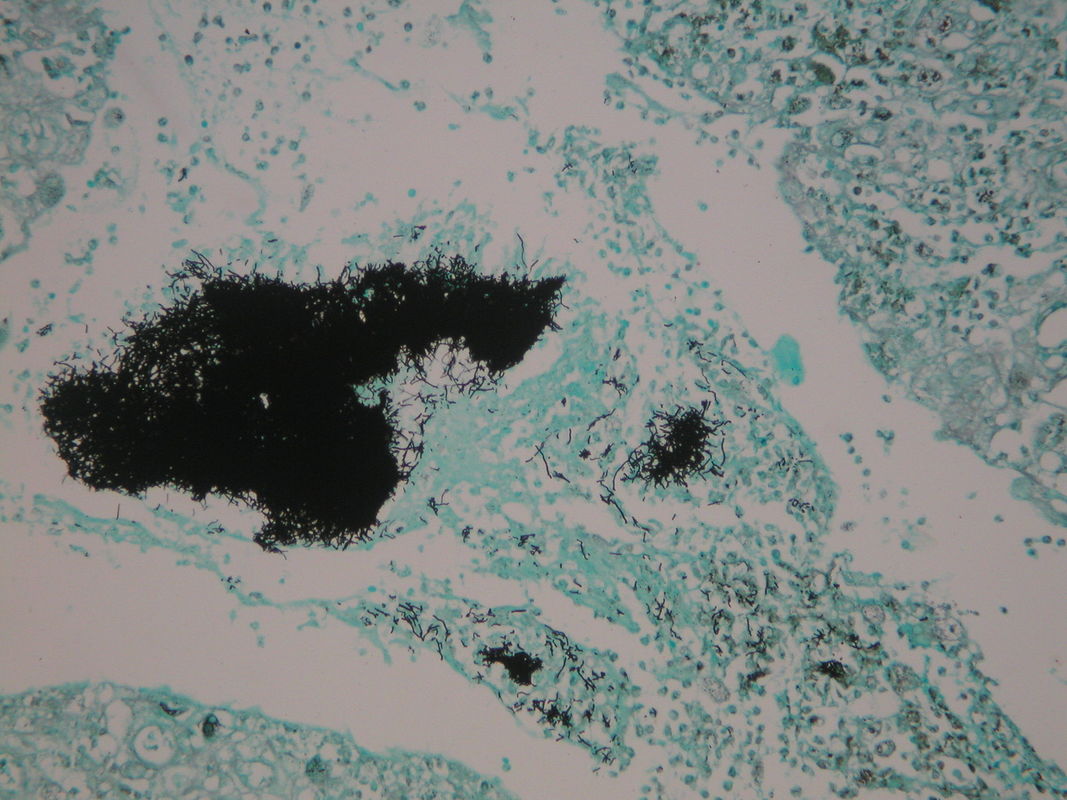
https://upload.wikimedia.org/wikipedia/commons/thumb/1/1e/Actinomycosis_GROCOTT%27S.JPG/1920px-Actinomycosis_GROCOTT%27S.JPG; Actinomyces in a GMS tissue stain
|
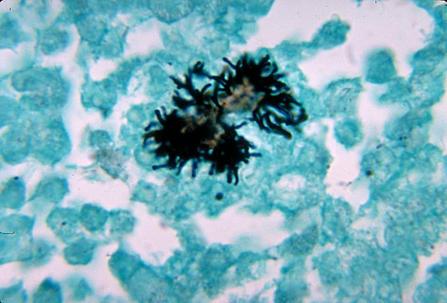
|
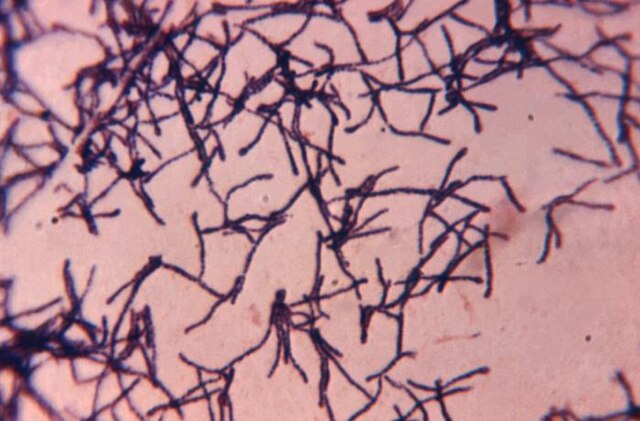
https://upload.wikimedia.org/wikipedia/commons/thumb/c/c2/22293_lores.jpg/640px-22293_lores.jpg

Nocardia spp:
Nocardia spp causes nocardiosis, in which symptoms resemble that of tuberculosis or actinomycosis (more info. about this bacterium is under the Mycobacterium/AFB tab), and is partially acid-fast. It is not a yeast, mold or AFB, however, it grows well on all the media and has a close appearance to both, both microscopically and macroscopically. Some strains are yeast-like, and some are chalky, powdery and mold-like. Occasionally, the organism has been associated with actinomycotic mycetoma. Repeat infections are very common, it is hard to clear, and tissue granules may be observed with second and subsequent infections.
Macroscopic Exam:
Microscopic Exam:
Nocardia spp causes nocardiosis, in which symptoms resemble that of tuberculosis or actinomycosis (more info. about this bacterium is under the Mycobacterium/AFB tab), and is partially acid-fast. It is not a yeast, mold or AFB, however, it grows well on all the media and has a close appearance to both, both microscopically and macroscopically. Some strains are yeast-like, and some are chalky, powdery and mold-like. Occasionally, the organism has been associated with actinomycotic mycetoma. Repeat infections are very common, it is hard to clear, and tissue granules may be observed with second and subsequent infections.
Macroscopic Exam:
- It grows well on Middlebrook 7H10 and 7H11 agars, which will enhance the acid-fast properites of the microbe, whereas growth on SABHI agar or BHI agar will not.
- It survives the mycobacterial concentration procedures in respiratory specimens, so it will grow quickly on mycobacterial media and LJ slants.
- Colonies resemble those of mycobacteria, but they are brittle, chalky, verrucose, and white, brown, or orange. I think they look like popcorn.
- They often have short aerial hyphae, which can be seen microscopically if you put the agar on the stage under the microscope, but cannot be seen macroscopically.
- Colonies have an earthy odor, like dirt or mud or rain.
- UREASE POSITIVE (This test can be used to differentiate Nocardia spp from other actinomycetes, but not from each other
- Modified Acid-Fast Stain Positive (This test can be used to differentiate Nocardia spp from other actinomycetes, but not from each other
Microscopic Exam:
- It stains purple, Gram-positive, and reveals branching, thin, filamentous, spotty bacteria on Gram-stain, which may fragment, and tiny conidia may be produced in older cultures with age. Many people miss this at first on the direct exam.
- It is partially acid-fast in the modified acid-fast stain, which reveals pink-red branching, thin, filamentous bacteria against a blue or green background.

Delicate, branching, beaded, intertwining filaments breaking off into bacillary and coccoid forms; Partially acid-fast
|

Grows rapidly, in 7-9 days, on SDA, L-J, and Middlebrook 7H11 medias aerobically, forming irregular, raised, somewhat folded colonies that are crumbly and dry, white-to-orange in color, and are glabrous or chalky
|

Chalky, cream-white colonies
|
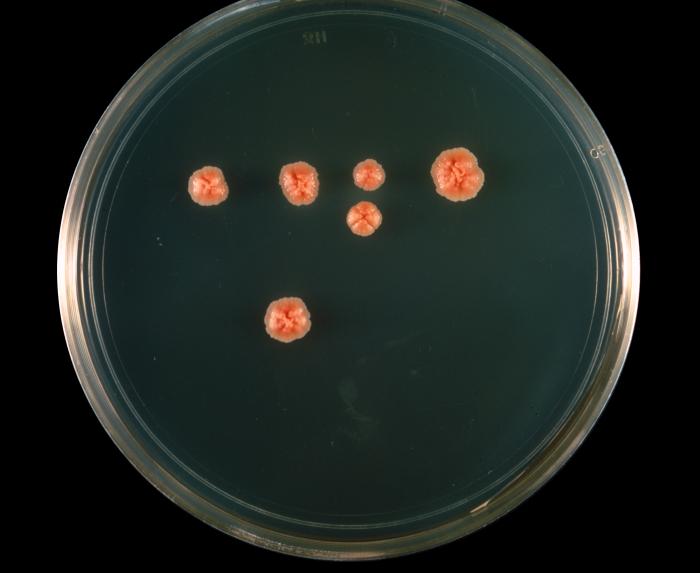
Glabrous, orange colonies
|
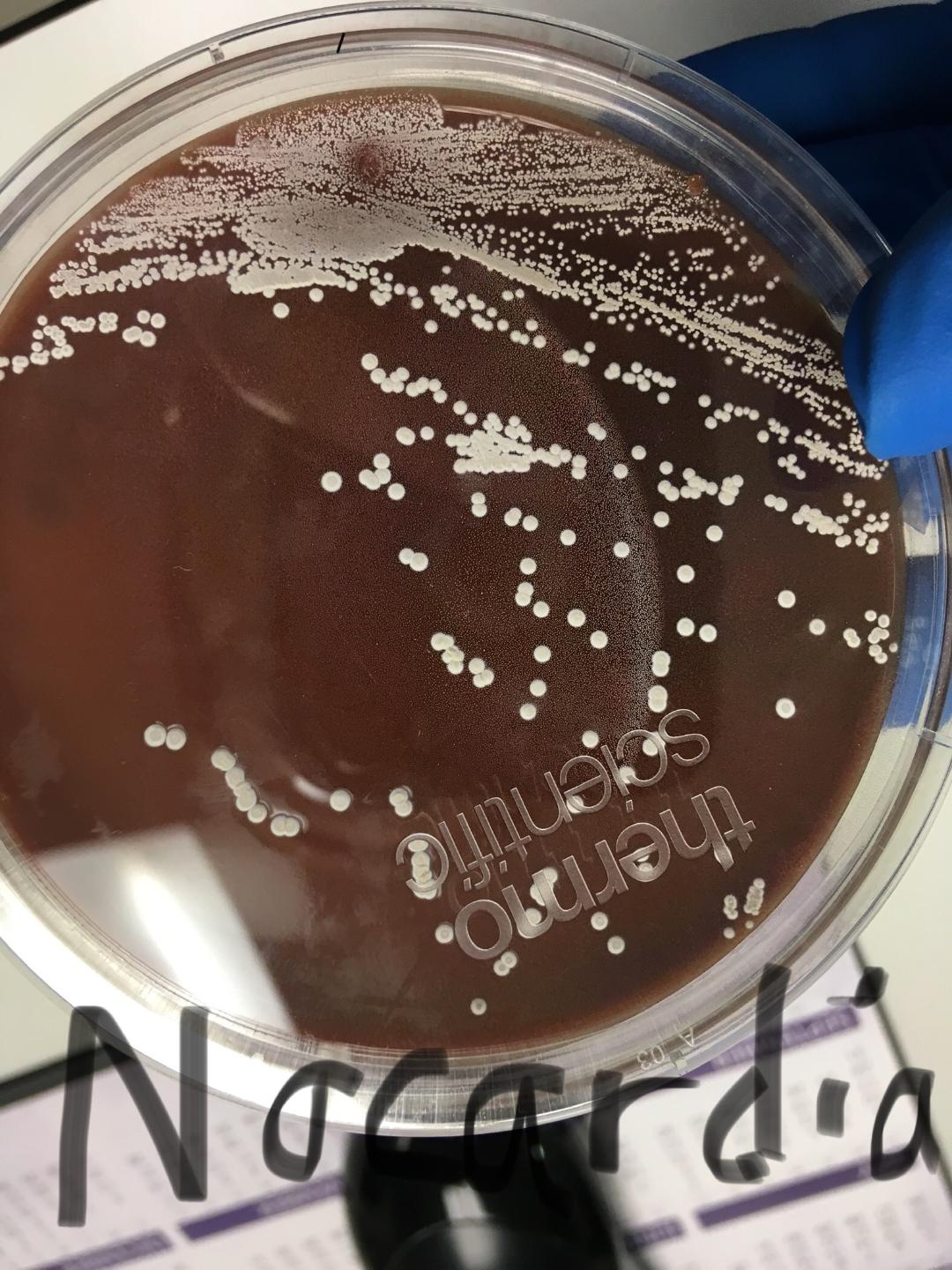
White, chalky colonies as part of Nocardia africana/nova complex; Image by Jeanette Reynolds, M-ASCP, MT-AMT, MS-Biology, Microbiologist
|

Brown mold-like colonies as part of Nocardia africana/nova complex; Image by Jeanette Reynolds, M-ASCP, MT-AMT, MS-Biology, Microbiologist
|

Orange, chalk-like colonies as part of Nocardia africana/nova complex; Image by Jeanette Reynolds, M-ASCP, MT-AMT, MS-Biology, Microbiologist
|
Gram stain from liquid media that was positive for Nocardia africana/nova complex; Image by Jeanette Reynolds, M-ASCP, MT-AMT, MS-Biology, Microbiologist
|
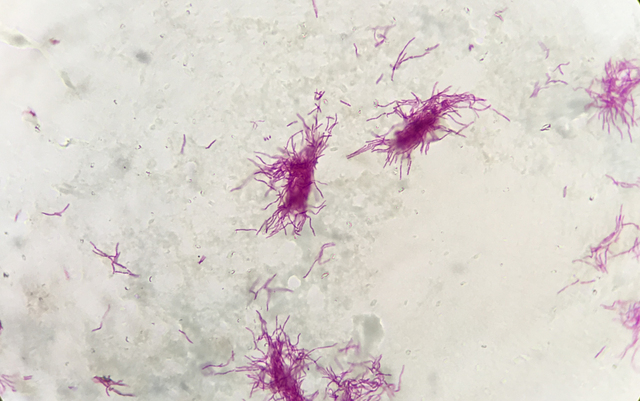
Modified acid-fast stain revealing Nocardia spp. https://upload.wikimedia.org/wikipedia/commons/thumb/f/fa/Nocardia.png/640px-Nocardia.png
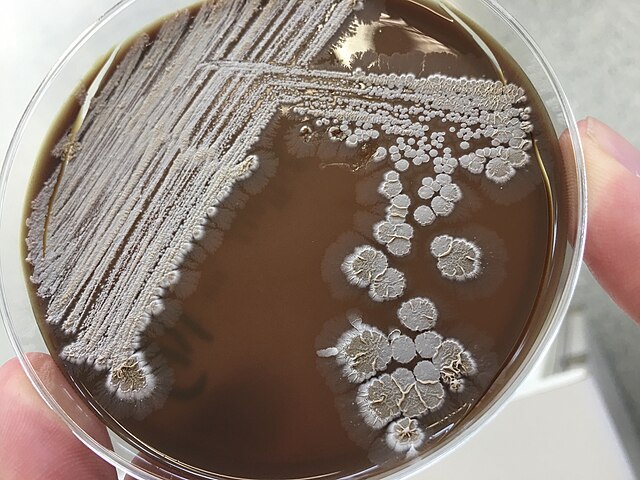
https://upload.wikimedia.org/wikipedia/commons/thumb/f/f6/Nocardia_species_CNA_plate_approximately_five_days_old.jpg/640px-Nocardia_species_CNA_plate_approximately_five_days_old.jpg

https://upload.wikimedia.org/wikipedia/commons/thumb/2/25/Four_different_Nocardia_species.jpg/1280px-Four_different_Nocardia_species.jpg
|
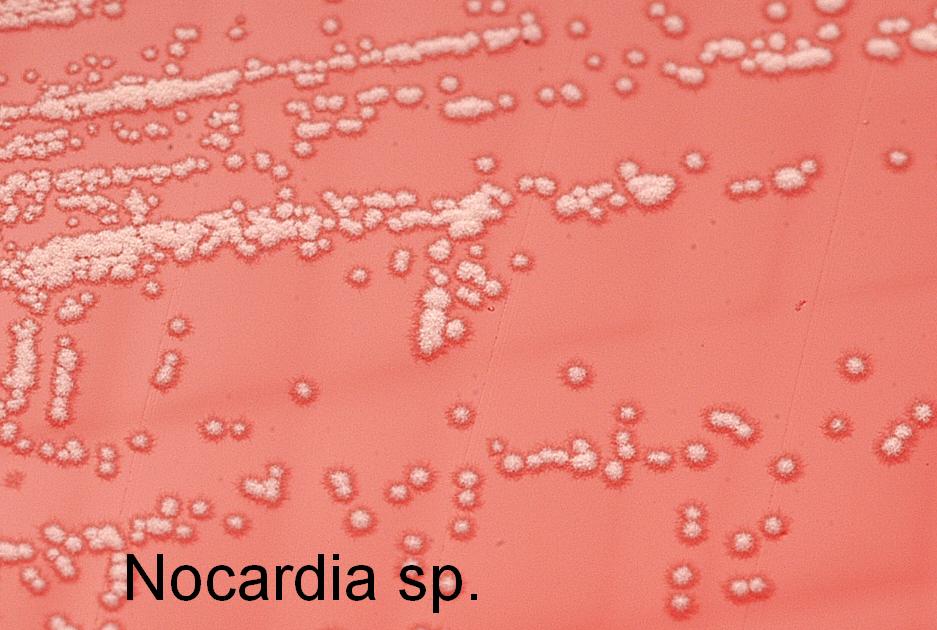
https://upload.wikimedia.org/wikipedia/commons/b/b8/Nocardia_species_close-up_detail.jpg
|
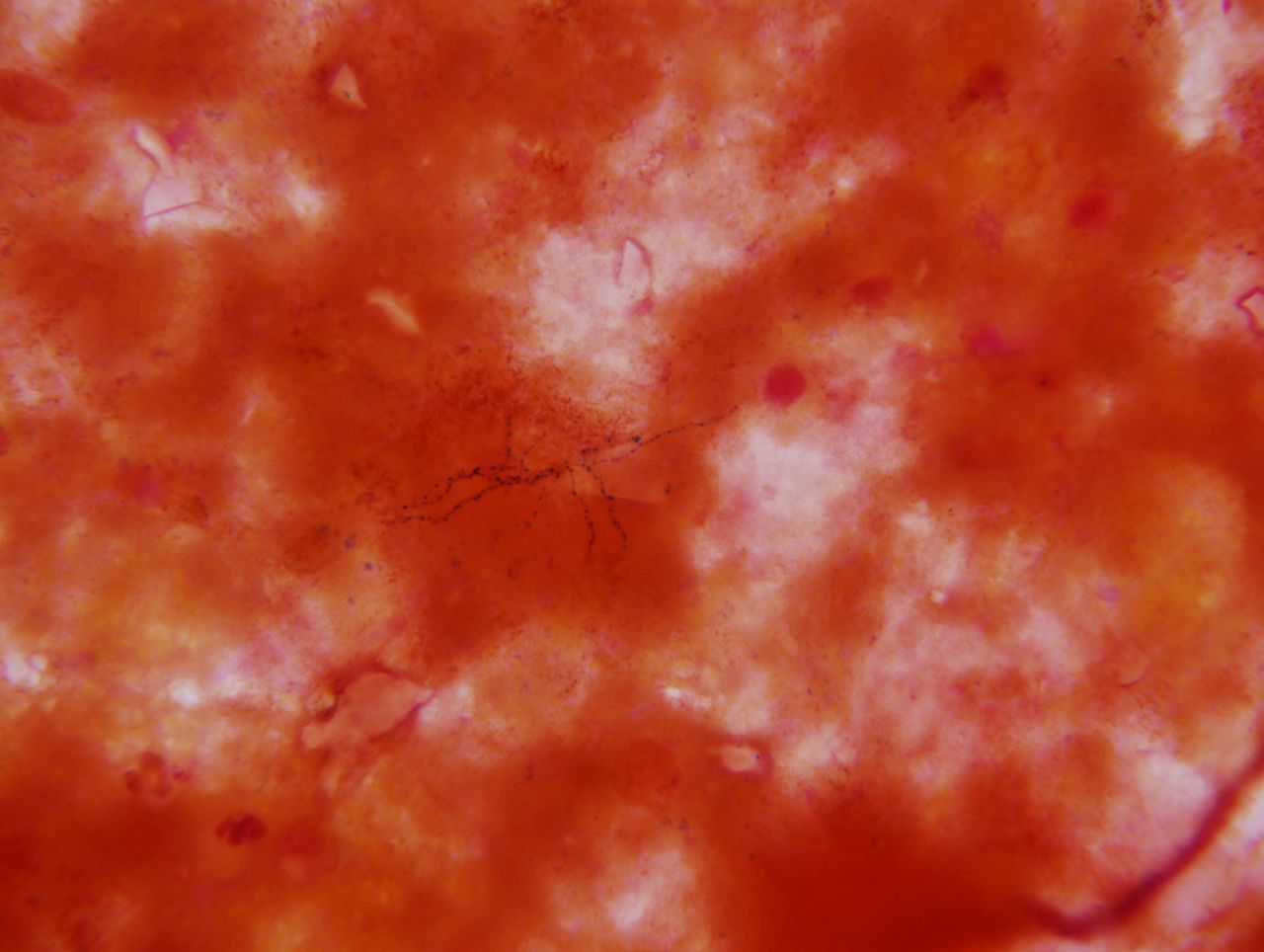
https://upload.wikimedia.org/wikipedia/commons/thumb/a/a9/Nocardia_Brain_Autopsy.jpg/1280px-Nocardia_Brain_Autopsy.jpg
Streptomyces:
This soil organism is typically nonpathogenic, however, in rare cases, it can cause mycetomas and other infections on occasion. In fact, 40% of this species are soil bacteria. This organism actually strengthens the soil texture, protecting it from the effects of wind and rain and erosion. When found in hay, it is a natural pesticide. It is found in manure, manured soil, and manured compost. It is a natural saprobic bacteria that aids in breaking things down to make rich organic material.
When raindrops hit the soil, it hits this bacteria, causing it to release a chemical that creates an earthy odor, a scent known as "petrichor", which is what you smell when it rains.
Did you know that 2/3rds of these strains are used to produce antibiotics to kill bacteria?
S. somaliensis: actinomycotic mycetoma
S. sudanensis, S. albus: occasional actinomycotic mycetoma
S. griseus: occasional subcutaneous abscesses and mycetomas
Most are nonpathogenic strains to humans, but are plant pathogens. Both S. tuberosum and S. scabies produce potato scabs.
Macroscopic Exam:
Microscopic Exam:
This soil organism is typically nonpathogenic, however, in rare cases, it can cause mycetomas and other infections on occasion. In fact, 40% of this species are soil bacteria. This organism actually strengthens the soil texture, protecting it from the effects of wind and rain and erosion. When found in hay, it is a natural pesticide. It is found in manure, manured soil, and manured compost. It is a natural saprobic bacteria that aids in breaking things down to make rich organic material.
When raindrops hit the soil, it hits this bacteria, causing it to release a chemical that creates an earthy odor, a scent known as "petrichor", which is what you smell when it rains.
Did you know that 2/3rds of these strains are used to produce antibiotics to kill bacteria?
S. somaliensis: actinomycotic mycetoma
S. sudanensis, S. albus: occasional actinomycotic mycetoma
S. griseus: occasional subcutaneous abscesses and mycetomas
Most are nonpathogenic strains to humans, but are plant pathogens. Both S. tuberosum and S. scabies produce potato scabs.
Macroscopic Exam:
- Rapid-growing on most primary isolation media, including the AFB slants
- Suppressed on media containing the antibiotics cycloheximide and chloramphenicol
- Exude an "earthy odor" (petrichor), which smells like "rain"
- Short aerial hyphae form on a range of colors of wrinkled, rugose, white-to-gray, buff, or tan colonies
- Some strains produce white or yellow granules
Microscopic Exam:
- NON-ACID-FAST, thin, branching, filamentous bacteria that stain Gram-positive and do not fragment easily
- Conidia may be produced with age
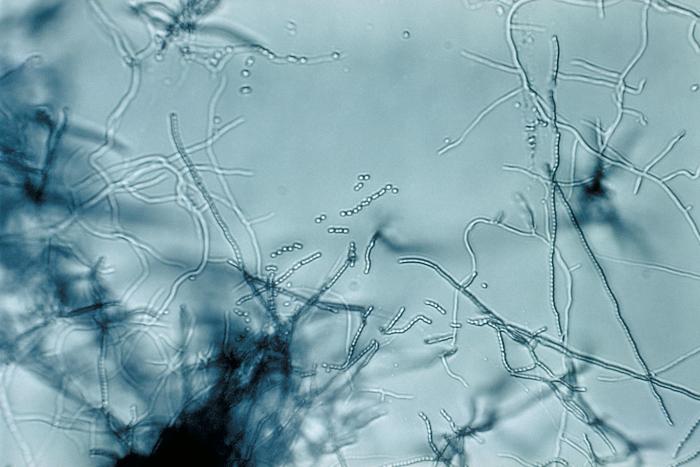
Microscopically, hyphae appear as thin, long, branching filaments that are straight, wavy, spiral, bearing small round-to-oval conidia
|
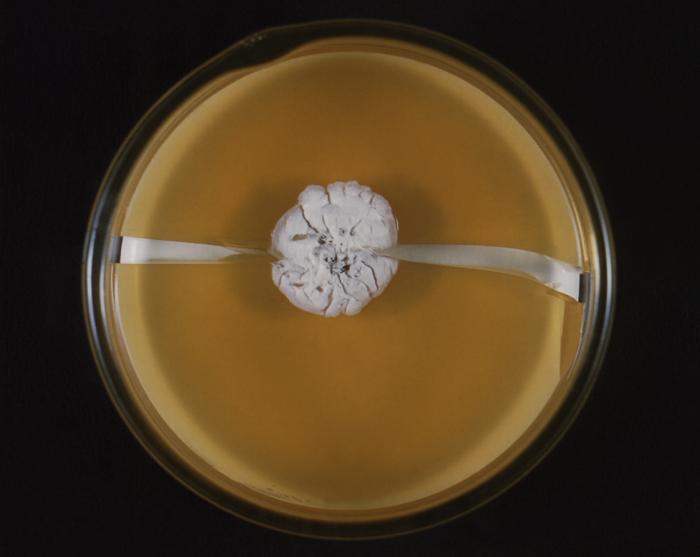
Colonies grow quickly and mature in 4-10 days, growing as folded, hard, whitish-gray, leathery, powdery, chalky colonies and produce an earthy aroma of soil
|
Actinomadura spp:
This is a frequent cause of actinomycotic mycetoma, particularly in the USA. These are NON-ACID-FAST, Gram-positive, filamentous bacilli that quickly grow on mycobacterial media, such as MHA agar and other primary isolation agars. Growth is excellent at 37 degrees Celsius.
Macroscopic Exam:
Microscopic Exam:
This is a frequent cause of actinomycotic mycetoma, particularly in the USA. These are NON-ACID-FAST, Gram-positive, filamentous bacilli that quickly grow on mycobacterial media, such as MHA agar and other primary isolation agars. Growth is excellent at 37 degrees Celsius.
Macroscopic Exam:
- It produces waxy colonies that are wrinkled and bear aerial hyphae.
- Colors are white-to-pink that redden with age.
- White-to-yellow or red granules may also be seen.
Microscopic Exam:
- These are NON-ACID-FAST, Gram-positive, filamentous, branching bacilli that quickly grow on mycobacterial media, such as MHA agar and other primary isolation agars.
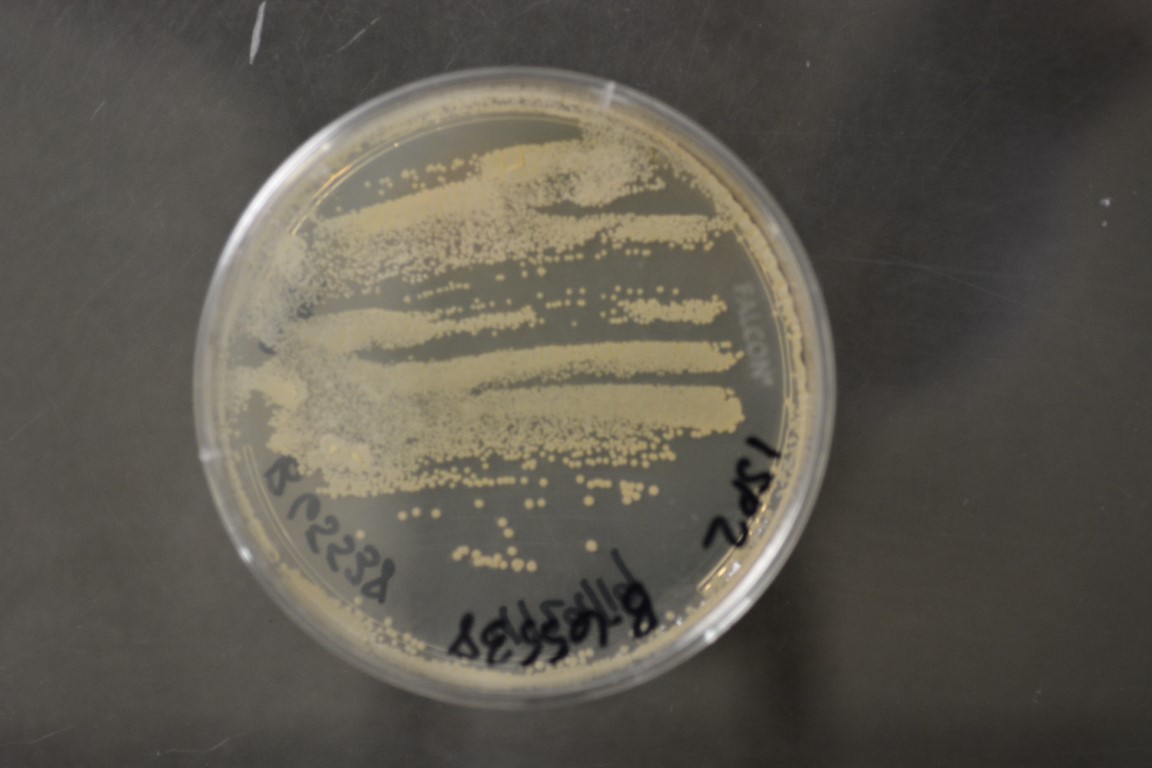
https://upload.wikimedia.org/wikipedia/commons/c/cb/Actinomadura_macrotermitis_sp._NRRL_B-65538_%28Type_Strain%29.jpg
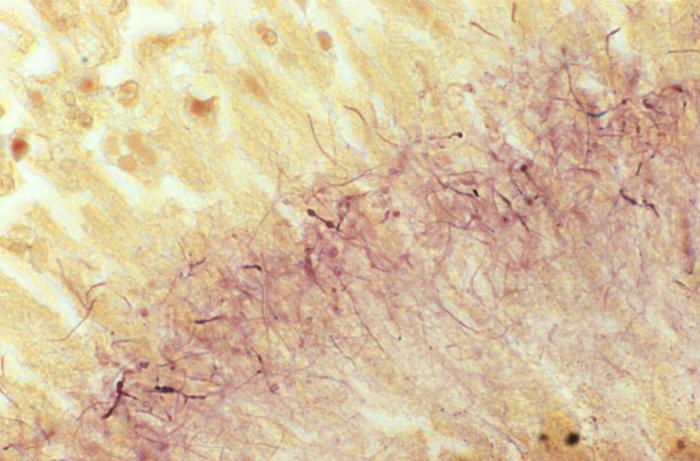
This rapid-grower produces waxy, folded, mucoid or membranous colonies on J-J or SAB agar. Colonies range in color from white to pink to red to orange. Microscopically, many Gram-positive, branched, thin filaments may be observed. Actinomadura spp is not acid-fast and does not fragment. Short chains of round conidia may form.
|
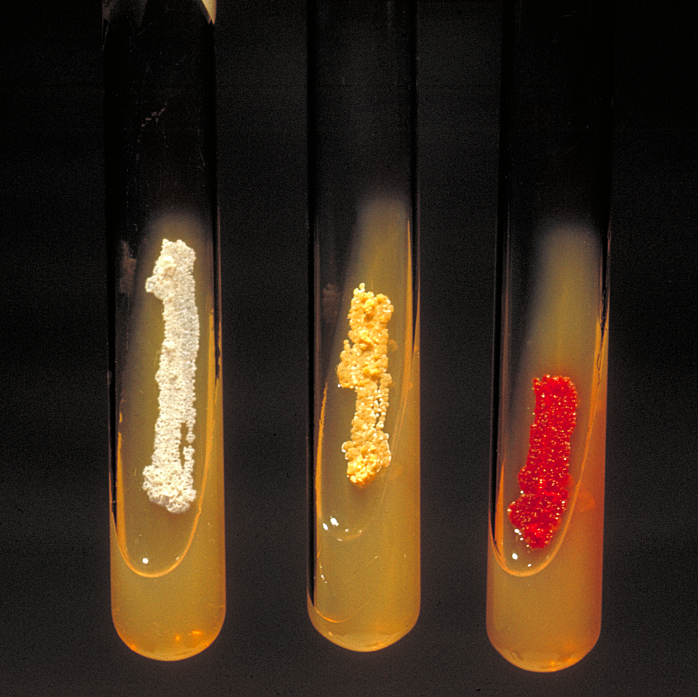
|
Nocardiopsis species:
This organism is common in the USA and is linked to actinomycotic mycetoma.
Macroscopic Exam:
Microscopic Exam:
This organism is common in the USA and is linked to actinomycotic mycetoma.
Macroscopic Exam:
- Colonies resemble those of Actinomadura spp, growing as a yellow, heaped colony on SABHI.
- Some strains produce cream-colored, irregularly-shaped granules.
Microscopic Exam:
- It stains Gram-positive, forming thin, branching, filamentous bacteria.
- It is NOT acid-fast.

https://upload.wikimedia.org/wikipedia/commons/thumb/9/92/Nocardiopsis_prasina.jpg/640px-Nocardiopsis_prasina.jpg
organisms that cause systemic mycoses: dimorphic molds
This section discusses the molds that are pathogenic and that have the ability to cause serious systemic disease. There are five major molds associated with systemic infection:
The concern with these fungi are that they have the ability to disseminate and spread throughout the body, infecting the tissues and organs and organ systems. The primary manifestation is often cutaneous, leading to secondary spread in some cases.
It is important to perform direct mounts, as well as perform conversion tests, since these molds are dimorphic molds and are slow-growers. Histology stains are helpful as well in terms of tissue staining. Brain heart infusion agar with blood is important in growing and culturing these organisms, since it provides nutrients to support their growth.
It is important to note that the mold forms of all of these are highly infectious, so proper PPE and work under the microbiology hood is criticial to avoid accidental infection.
- Blastomyces dermatididis
- Paraccodicioides brasiliensis
- Histoplasma capsulatum
- Coccidioides immitis
- Pneumocystis carinii
The concern with these fungi are that they have the ability to disseminate and spread throughout the body, infecting the tissues and organs and organ systems. The primary manifestation is often cutaneous, leading to secondary spread in some cases.
It is important to perform direct mounts, as well as perform conversion tests, since these molds are dimorphic molds and are slow-growers. Histology stains are helpful as well in terms of tissue staining. Brain heart infusion agar with blood is important in growing and culturing these organisms, since it provides nutrients to support their growth.
It is important to note that the mold forms of all of these are highly infectious, so proper PPE and work under the microbiology hood is criticial to avoid accidental infection.
Blastomyces dermatiditis:
This organism is the causative agent of Blastomycosis (chronic infection with granulomatous and suppurative lesions). Infection commonly starts out in the lungs, disseminating to the skin and bones. This disease is also known as North American Blastomycosis or Gilchrist's Disease.
It is most often observed south of the Ohio River and east of the Mississippi River. Cases have been found in other areas as well. It is thought that the conidia are inhaled first, producing a mild respiratory infection at first. Symptoms gradually persist and worsen over time. The sputum often becomes purulent and streaked with blood, resemblant of tuberculosis. Without treatment, it spreads to the rest of the body, including nearby tissues, skin, bone, and system spread.
The cutaneous form results in skin lesions that become ulcerated, crusted over, and weepy over time, forming abscesses in the middle. The mucosal surfaces may also become infected. Bone lesions are painful and lead to loss of function. It can lead to fungemia and sepsis, being isolated from blood cultures. Prognosis is poor if it doesn't respond to amphotericin B or one of the azoles or if it remains untreated.
Macroscopic Exam:
Microscopic Exam:
This organism is the causative agent of Blastomycosis (chronic infection with granulomatous and suppurative lesions). Infection commonly starts out in the lungs, disseminating to the skin and bones. This disease is also known as North American Blastomycosis or Gilchrist's Disease.
It is most often observed south of the Ohio River and east of the Mississippi River. Cases have been found in other areas as well. It is thought that the conidia are inhaled first, producing a mild respiratory infection at first. Symptoms gradually persist and worsen over time. The sputum often becomes purulent and streaked with blood, resemblant of tuberculosis. Without treatment, it spreads to the rest of the body, including nearby tissues, skin, bone, and system spread.
The cutaneous form results in skin lesions that become ulcerated, crusted over, and weepy over time, forming abscesses in the middle. The mucosal surfaces may also become infected. Bone lesions are painful and lead to loss of function. It can lead to fungemia and sepsis, being isolated from blood cultures. Prognosis is poor if it doesn't respond to amphotericin B or one of the azoles or if it remains untreated.
Macroscopic Exam:
- MOLD: On SABHI agar at room temperature, initially, a yeast-like colony can be seen. The middle becomes prickly, and with age, it will turn fluffy white or tan.
- YEAST: On BHI with blood, incubated at 37 degrees Celsius, colonies appear waxy, wrinkled, and are cream or tan in color. Conversion from mold to yeast phase takes 4-5 days.
Microscopic Exam:
- MOLD: Perform a tease mount of the mold at room temperature. It will reveal single, smooth-walled, round or oval conidia at the ends of short conidiophores or on the sides of the hyphae. It will resemble some other molds we've covered.
- YEAST: Exhibits large, round, thick-walled budding yeasts with a broad base of attachment (isthmus) between the mother and daughter cells.
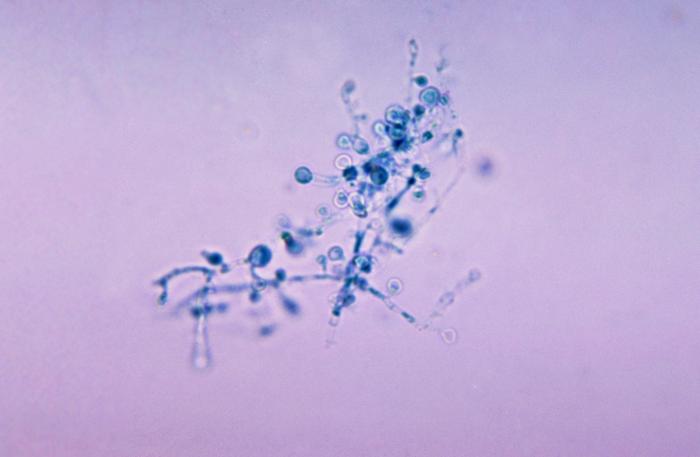
B. dermatitidis forms septate hyphae that bear slightly oval, pear-shaped conidia. May be converted to yeast phase for identification.
|
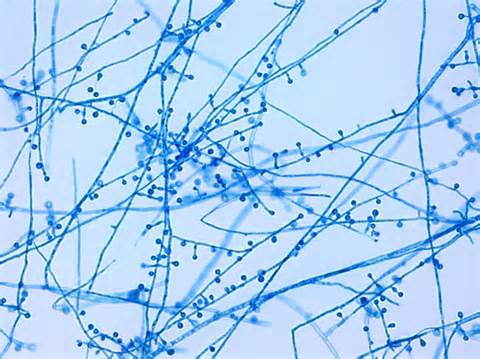
Mold phase LPCB stained B. dermatitidis showing mostly oval-shaped conidia borne along the sides of the hyphae
|

Mold form of B. dermatitidis, revealing a fluffy white-tan colony on SABHI agar
|

B. dermatitidis even grows well on the LJ slants used for AFB mycobacterium.
|
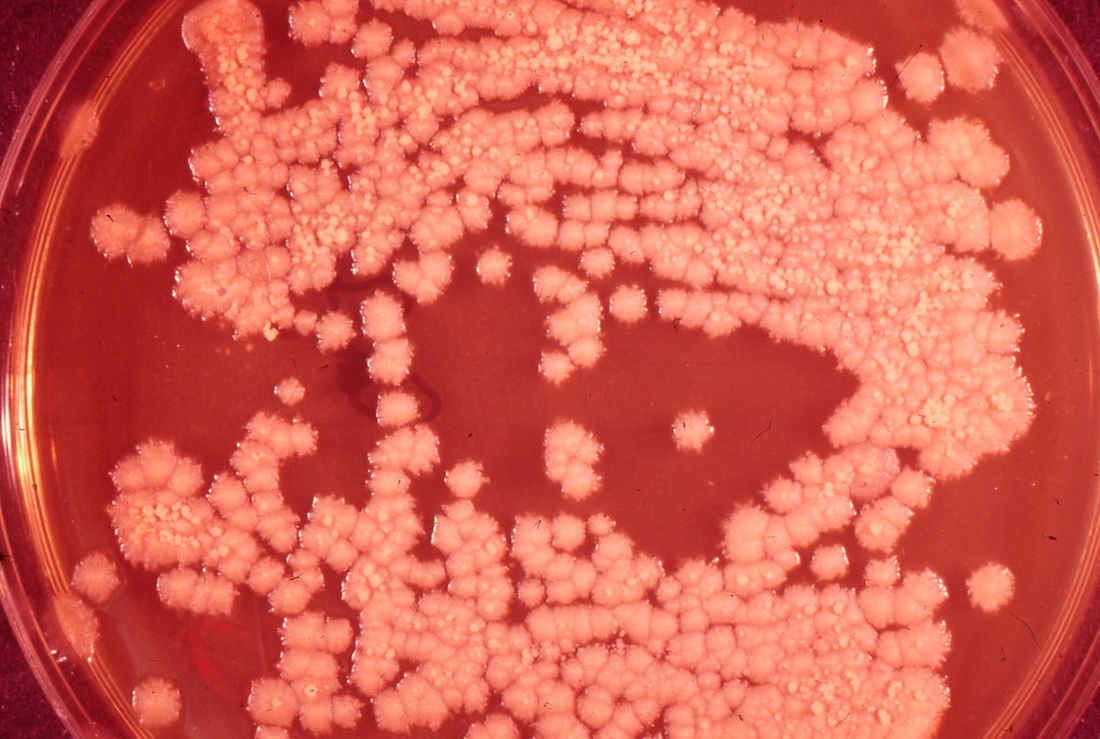
This is BHI agar with 10% blood, revealing the conversion stage from mold to yeast of B. dermatitidis
|
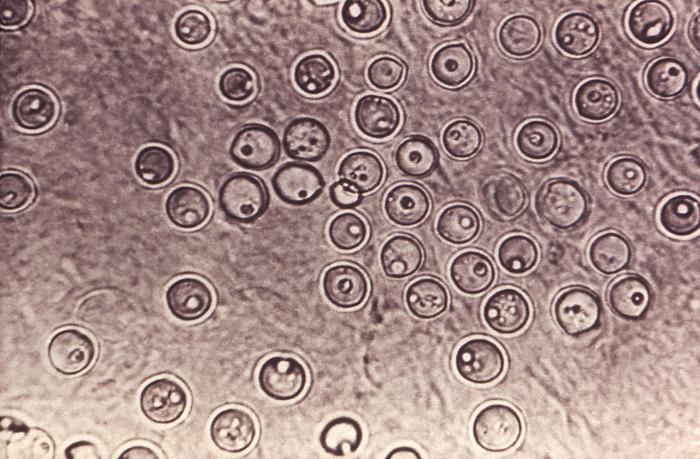
These are the yeast form of B. dermatitidis on wet mount
|
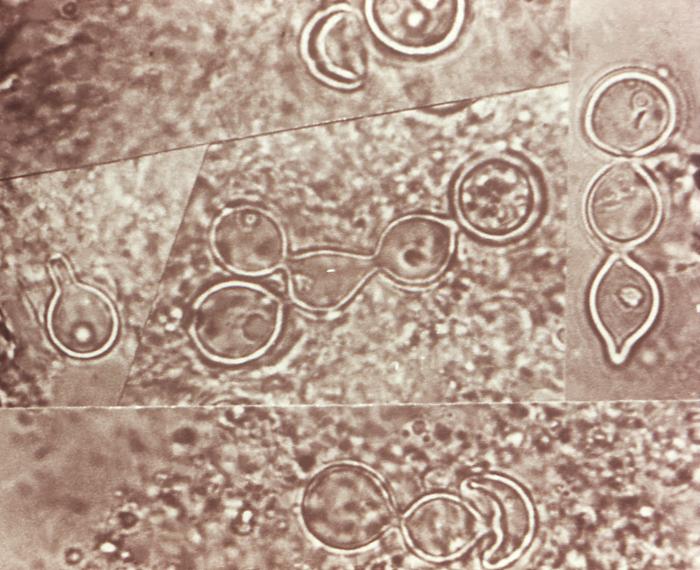
These are budding yeast forms of B. dermatitidis on wet mount
|
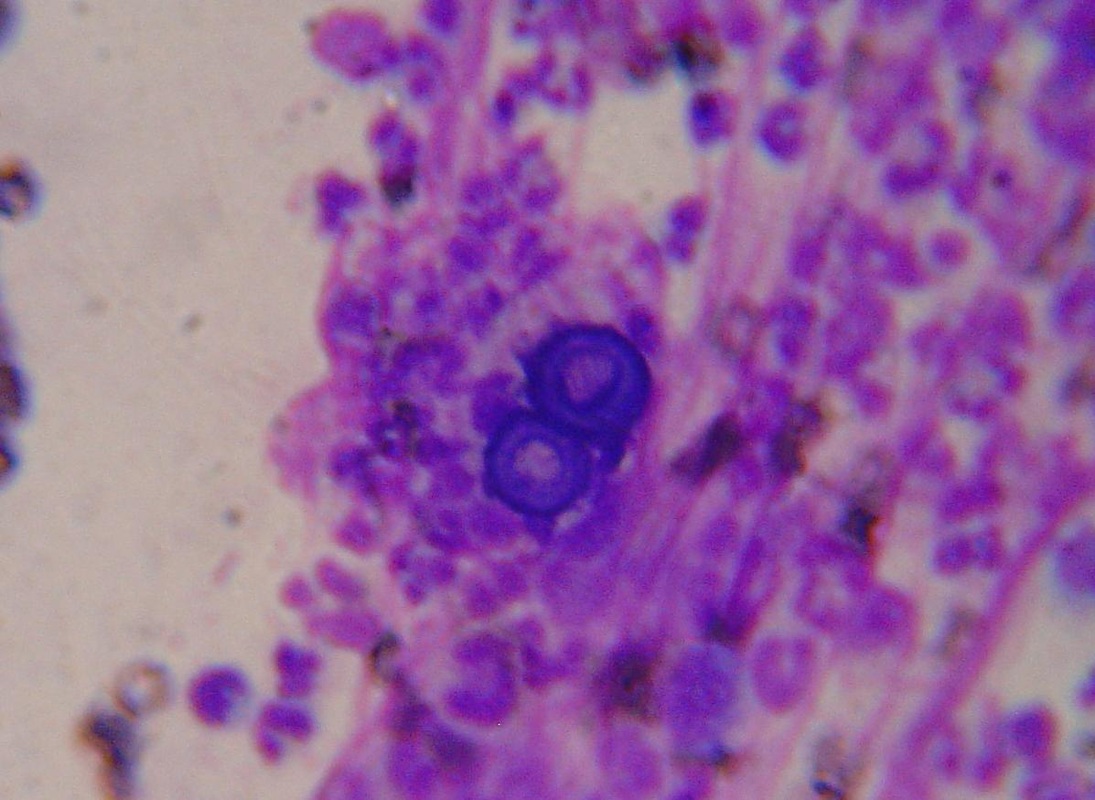
B. dermatitidis yeast form stains purple, Gram-positive, in Gram stain, which is often missed in the direct exam, particularly by new or inexperienced techs
|
Histoplasma capsulatum:
This is the causative agent of Histoplasmosis (an acute, benign pulmonary illness or a chronic, progressive, and/or fatal disease), also known as Darling's disease. This may affect the reticuloendothelial system and may involve numerous tissues and/or organs throughout the body. It is carried by pigeons and other birds.
This organism is endemic in the Mississippi River area, the Ohio River valley, and along the Appalachian Mountains. The fungus multiplies in bird droppings, and in chicken droppings and bat guano. The fungus colonizes the GI tract of bats. Wind transports the fungus when the particles are disturbed, or when contaminated soil is disturbed.
The disease is NOT spread from human-to-human or from animal-to-human. It is either directly inoculated into the skin or inhaled. Of all infections, 90-95% are asymptomatic or mild, with a self-limiting respiratory flu-like illness. In endemic areas, it produces a positive skin test.
Those who do get really sick from the disease exhibit signs and symptoms resembling tuberculosis, with an acute form of pulmonary disease with night sweats, fever, chills, cough, weight loss, and sometimes pulmonary cavitation. In some cases, it can spread through the bloodstream to the kidneys, adrenal glands, spleen, liver, skin, oral mucosa, eye, central nervous system, or other organs, becoming chronic in those who were otherwise healthy prior to the disease, or in a severe, fulminant disease in those who are immunocompromised.
In those with HIV/AIDS, about 53% from the endemic areas develop histoplasmosis. These patients often experience the symptoms discussed above, plus splenomegaly, adenopathy, anemia, leukopenia, thrombocytopenia, and abnormal chest radiographs with interstitial infiltrates.
Treatment includes amphotericin B or one of the azoles.
Macroscopic Exam:
Microscopic Exam:
This is the causative agent of Histoplasmosis (an acute, benign pulmonary illness or a chronic, progressive, and/or fatal disease), also known as Darling's disease. This may affect the reticuloendothelial system and may involve numerous tissues and/or organs throughout the body. It is carried by pigeons and other birds.
This organism is endemic in the Mississippi River area, the Ohio River valley, and along the Appalachian Mountains. The fungus multiplies in bird droppings, and in chicken droppings and bat guano. The fungus colonizes the GI tract of bats. Wind transports the fungus when the particles are disturbed, or when contaminated soil is disturbed.
The disease is NOT spread from human-to-human or from animal-to-human. It is either directly inoculated into the skin or inhaled. Of all infections, 90-95% are asymptomatic or mild, with a self-limiting respiratory flu-like illness. In endemic areas, it produces a positive skin test.
Those who do get really sick from the disease exhibit signs and symptoms resembling tuberculosis, with an acute form of pulmonary disease with night sweats, fever, chills, cough, weight loss, and sometimes pulmonary cavitation. In some cases, it can spread through the bloodstream to the kidneys, adrenal glands, spleen, liver, skin, oral mucosa, eye, central nervous system, or other organs, becoming chronic in those who were otherwise healthy prior to the disease, or in a severe, fulminant disease in those who are immunocompromised.
In those with HIV/AIDS, about 53% from the endemic areas develop histoplasmosis. These patients often experience the symptoms discussed above, plus splenomegaly, adenopathy, anemia, leukopenia, thrombocytopenia, and abnormal chest radiographs with interstitial infiltrates.
Treatment includes amphotericin B or one of the azoles.
Macroscopic Exam:
- MOLD: On BHI with blood at room temperature, it grows slowly, and the initial colony is moist. With age, it develops low white or brown aerial mycelium, causing the colony to be a mix of glabrous, velvety, or woolly appearance.
- On SABHI agar, the characteristic microscopic structures will develop.
- YEAST: Subculture to BHI agar with blood at 37 degrees Celsius for conversion to yeast form. Colonies will be rough, mucoid, cream or tan. It might take a few transfers to convert it from mold to yeast form.
Microscopic Exam:
- MOLD: Perform a LPCB tease mount of the mold phase from SABHI agar. You will see conidiophores at 90-degree angles to the hyphae, bearing large, round macroconidia with smooth, spiny, or finlike, tuberculate edges, which support small, round or teardrop-shaped microconidia that are rough or smooth along the sides of the hyphae. These are called TUBERCULATE MACROCONIDIA.
- YEAST: The yeast phase appears as small, single budding yeast cells.
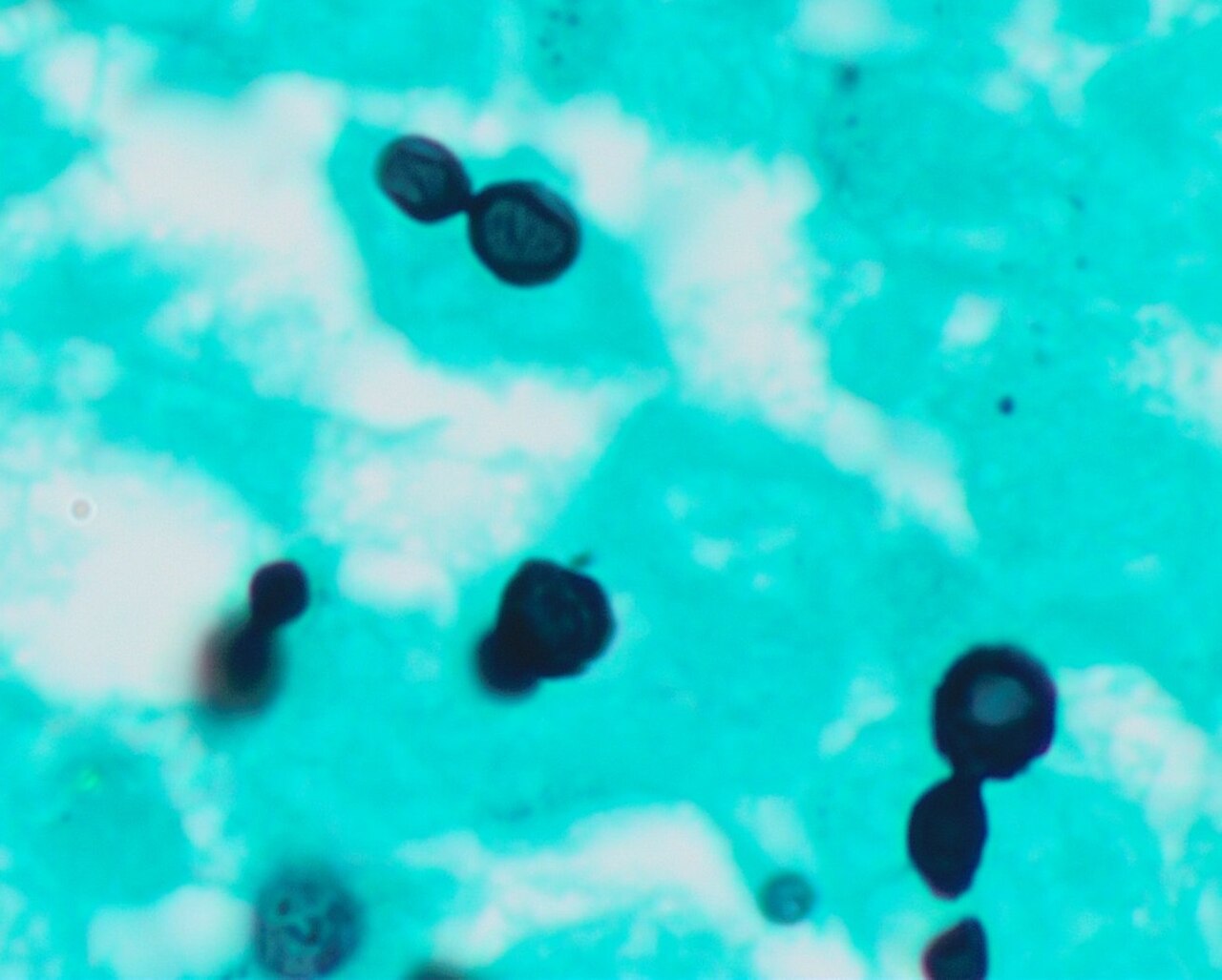
Yeast form of H. capsulatum; https://upload.wikimedia.org/wikipedia/commons/thumb/2/2d/Histopathology_of_Histoplasma_capsulatum%2C_GMS_stain.jpg/1280px-Histopathology_of_Histoplasma_capsulatum%2C_GMS_stain.jpg
|
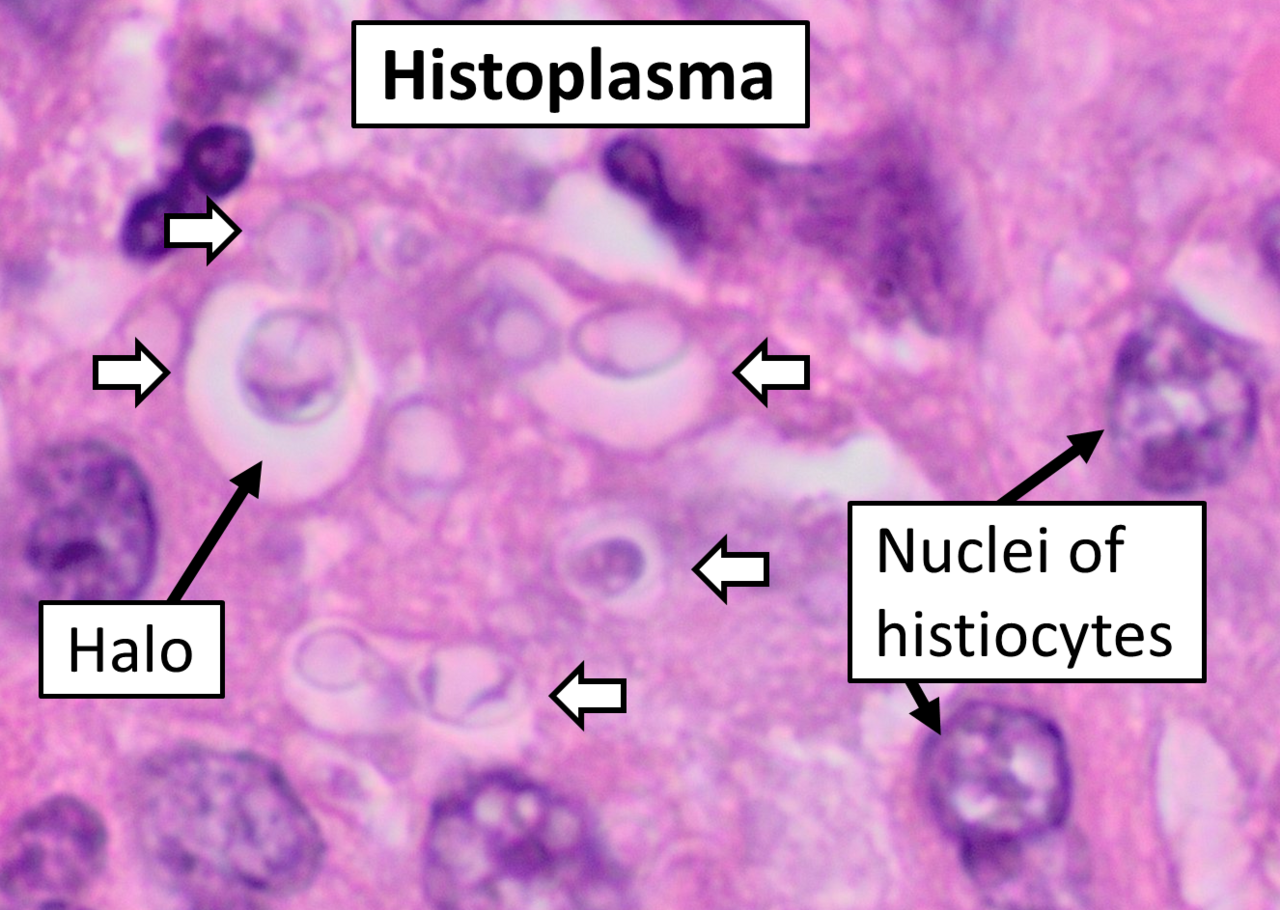
Yeast form of H. capsulatum; https://upload.wikimedia.org/wikipedia/commons/thumb/3/3f/Histopathology_of_histoplasma%2C_HE_stain.png/1280px-Histopathology_of_histoplasma%2C_HE_stain.png
|

This fungus is characterized by septate hyphae bearing round conidia with spines, resembling a flower or a ship's wheel. This is called tuberculate macroconidia. Conversion to the yeast phase is required for identification.
|
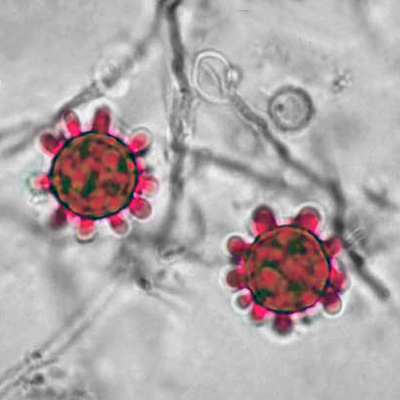
uberculate macroconidia; https://upload.wikimedia.org/wikipedia/commons/0/06/Histoplasma_capsulatum_%288538519681%29.jpg
|
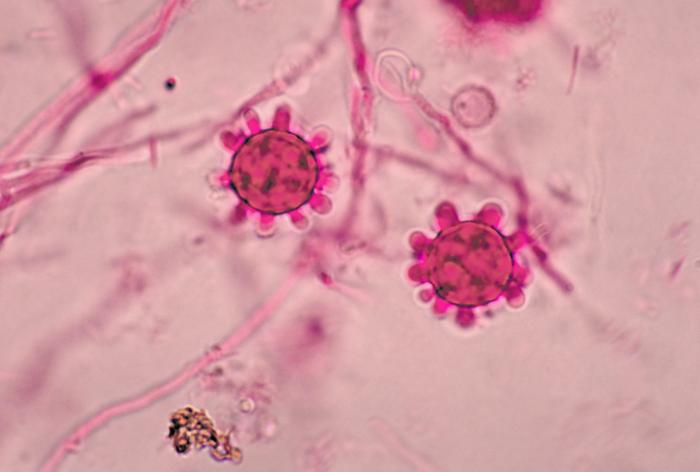
Tuberculate macroconidia of H. capsulatum
|
Paracoccidioides brasiliensis:
This is the causative agent of Paracoccidioidomycosis (chronic granulomatous disease). It is also known as South American Blastomycosis. Typically, this illness starts out in the lungs and disseminates to the mucous membranes, skin, lymph nodes, and even the internal organs throughout the body.
This disease is endemic in South America, particularly Brazil. This fungus is a saprobe, and it colonizes soil, water, and plants. The mold form causes disease if it is inhaled, producing pulmonary lesions resemblant of mycobacterium and other mycoses. It can also infect the oral mucosa or gums following chewing of contaminated vegetation. These lesions crust over, and can spread to the tonsils, nasal mucosa, and even the face. It can also cause oral ulcers. If swallowed, it can cause GI manifestations. The fungus can spread to the liver, spleen, and adrenal glands above the kidneys.
Lymph node enlargement is common an can be biopsied for culture and stain. If disease becomes disseminated, the prognosis is not good, and patients are typically given a 2-3 year life expectancy. HIV/AIDS patients who ecome infected may also get very ill and have an even lower life expectancy.
Therapy includes trimethoprim sulfamethoxazole or one of the other fungal azoles.
Macroscopic Exam:
Microscopic Exam:
This is the causative agent of Paracoccidioidomycosis (chronic granulomatous disease). It is also known as South American Blastomycosis. Typically, this illness starts out in the lungs and disseminates to the mucous membranes, skin, lymph nodes, and even the internal organs throughout the body.
This disease is endemic in South America, particularly Brazil. This fungus is a saprobe, and it colonizes soil, water, and plants. The mold form causes disease if it is inhaled, producing pulmonary lesions resemblant of mycobacterium and other mycoses. It can also infect the oral mucosa or gums following chewing of contaminated vegetation. These lesions crust over, and can spread to the tonsils, nasal mucosa, and even the face. It can also cause oral ulcers. If swallowed, it can cause GI manifestations. The fungus can spread to the liver, spleen, and adrenal glands above the kidneys.
Lymph node enlargement is common an can be biopsied for culture and stain. If disease becomes disseminated, the prognosis is not good, and patients are typically given a 2-3 year life expectancy. HIV/AIDS patients who ecome infected may also get very ill and have an even lower life expectancy.
Therapy includes trimethoprim sulfamethoxazole or one of the other fungal azoles.
Macroscopic Exam:
- MOLD: On SABHI agar at room temperature, colonies take about 2-3 weeks to grow, revealing smooth colonies, which later become covered with aerial mycelium, and they are white or tan in color.
- YEAST: On BHI with blood agar at 37 degrees Celcius, colonies are waxy, wrinkled, and are cream or tan in color. Conversion to the yeast phase takes about 3-7 days.
Microscopic Exam:
- MOLD: Perform a LPCB tease mount of the mold phase, and you will see mainly hyphae with intercalary and terminal chlamydoconidia.
- YEAST: The LPCB stain of the yeast phase will reveal large, thick-walled, multiple budding yeast cells with narrow necks where the daughter cells attach. They bear a close resemblance to a SHIP'S WHEEL.

https://upload.wikimedia.org/wikipedia/commons/thumb/0/05/Paracoccidioides_brasiliensis_slant_culture.jpg/640px-Paracoccidioides_brasiliensis_slant_culture.jpg
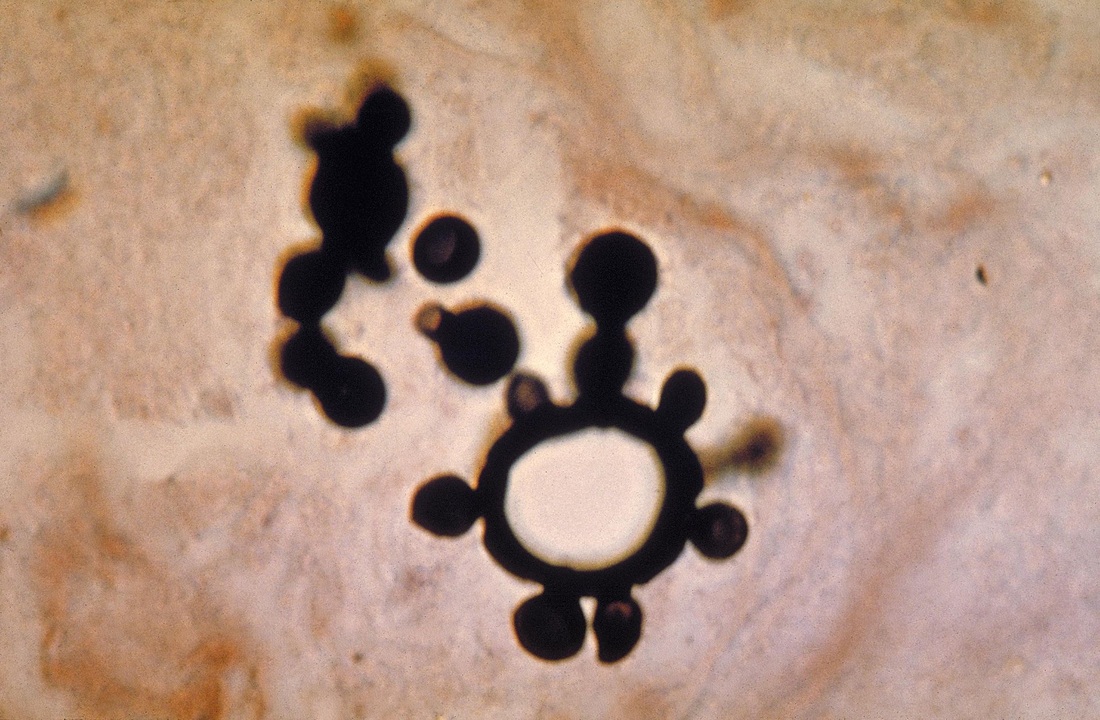
This fungus produces septate, branched hyphae with some intercalary and terminal chlamydospores. This needs to be converted to the yeast phase for identification. The yeast phase looks like a ship's wheel due to the knobby appearance of the large, round, thick-walled single and multiple buds. The buds nearly completely surround the mother cell.
|
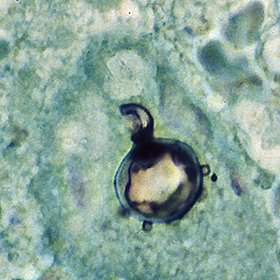
https://upload.wikimedia.org/wikipedia/commons/8/8c/Paracoccidioides_brasiliensis_tissue_GMS.jpg
|
Coccidioides immitis:
This organism is the causative agent of Coccidioidomycosis, also known as San Joaquin Fever. It is named for the desert where it was discovered, as it is endemic in the desert areas of the southwestern corner of the USA.
Arthroconidia in the sand are very resistant to heat, dry conditions, and salinity, and they colonize the soil. After inhaling arthroconidia, about 10-14 days later, 60% of those who become infected exhibit asymptomatic respiratory infection, but the remaining 40% experience symptoms of mild, intermediate, or severe flu-like respiratory symptoms. This is followed by recovery in immunocompetent individuals. If an individual has underlying illness or is otherwise immunocompromised or immunosuppressed, it can case severe illness and rapid dissemination to other parts of the body. 3% of the population in these areas carries the fungus without any symptoms, and will test positive on a skin test. More than 20% of HIV/AIDS patients in these endemic areas will develop a clearly symptomatic coccidioidomycosis each year, which can lead to pulmonary complications, including cavitation of the lung, or persistent pneumonia.
This is a highly infectious disease that may either be self-limiting or chronic, malignant and life-threatening. Infection that may involve not only the respiratory system, but may also spread to the skin, bone, joints, lymph nodes, adrenal glands, and/or central nervous system as well. It is treated by amphotericin B or the azoles.
The concern about this organsim is the worry that it it might be used as a bioterrorism agent, so techs should be trained to quickly identify this organism.
Macroscopic Exam:
Microscopic Exam:
This organism is the causative agent of Coccidioidomycosis, also known as San Joaquin Fever. It is named for the desert where it was discovered, as it is endemic in the desert areas of the southwestern corner of the USA.
Arthroconidia in the sand are very resistant to heat, dry conditions, and salinity, and they colonize the soil. After inhaling arthroconidia, about 10-14 days later, 60% of those who become infected exhibit asymptomatic respiratory infection, but the remaining 40% experience symptoms of mild, intermediate, or severe flu-like respiratory symptoms. This is followed by recovery in immunocompetent individuals. If an individual has underlying illness or is otherwise immunocompromised or immunosuppressed, it can case severe illness and rapid dissemination to other parts of the body. 3% of the population in these areas carries the fungus without any symptoms, and will test positive on a skin test. More than 20% of HIV/AIDS patients in these endemic areas will develop a clearly symptomatic coccidioidomycosis each year, which can lead to pulmonary complications, including cavitation of the lung, or persistent pneumonia.
This is a highly infectious disease that may either be self-limiting or chronic, malignant and life-threatening. Infection that may involve not only the respiratory system, but may also spread to the skin, bone, joints, lymph nodes, adrenal glands, and/or central nervous system as well. It is treated by amphotericin B or the azoles.
The concern about this organsim is the worry that it it might be used as a bioterrorism agent, so techs should be trained to quickly identify this organism.
Macroscopic Exam:
- MOLD: On SABHI agar at room temperature or at 37 degrees Celsius, a moist white colony forms in 5-7 days, which later becomes covered with aerial mycelium, turning it white and fluffy.
- It takes about 2 weeks of growth for characteristic arthroconidia to form.
- Colonies can also be grown on Sheep Blood Agar or Chocolate Agar.
- YEAST: Conversion to yeast form from mold form occurs by inoculating BHI agar with 10% blood and incubation at 37 degrees Celsius.
Microscopic Exam:
- MOLD: A tease mount in LPCB should be performed on colonies that are at least 2 weeks old. It will reveal hyphae branching at 90-degree angles with many thick-walled, barrel-shaped or rectangular arthroconidia, alternating with empty disjunctor cells.
- YEAST: The tissue phase produces spherules, which are grown under special conditions, and are round, thick-walled sporangia filled with tiny endospores.
- Spherules form germ-tubes after 24-hour incubation at 37 degrees.

https://upload.wikimedia.org/wikipedia/commons/thumb/f/f2/Coccidioides_immitis.jpg/640px-Coccidioides_immitis.jpg

Characteristic barrel-shaped, thick-walled arthroconidia of C. immitis, which are highly infectious and some racquet hyphae
|
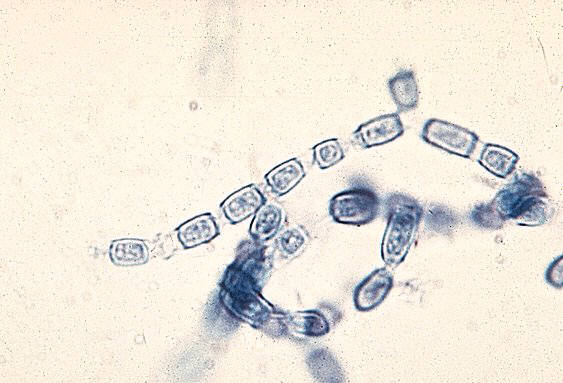
Typical "barrel-shaped" arthroconidia characteristic of C. immitis
|
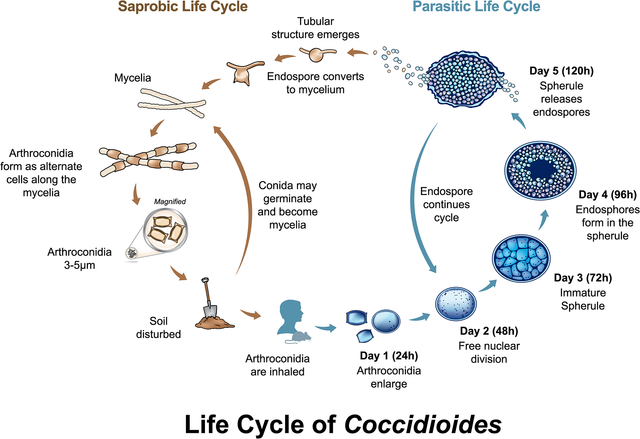
https://upload.wikimedia.org/wikipedia/commons/thumb/1/19/Life_cycle_of_Coccidioides.PNG/640px-Life_cycle_of_Coccidioides.PNG
Stachybotrys:
This is a black mold that, if found in the environment, can cause severe, even life-threatening, allergic reactions/responses in some people. It is also responsible for causing "sick building syndrome" in some people. Sick building syndrome is a condition in which individuals suffer from symptoms of illness and feeling unwell, and the more time that is spent in a building contaminated with the mold causing this syndrome, the more severe the symptoms become. Individuals may notice they actually feel better when away from the building. Symptoms typically include headache, eye, nose, throat irritation, fatigue, brain fog, dizziness, and even nausea. Poor air quality associated with mold growth is the cause of these symptoms. The mold may be hidden and be growing due to dampness, moisture, a water pipe leak or burst, or after water damage due to leaks.
Most of the time, this mold is considered a contaminant but Stachybotrys alternans produces a very potent toxin that may be lethal. Reactions occur via inhalation of spores or absorption through the skin or traumatic injury. The mold is filamentous and produces spores. It is referred to as a "black mold". It produces mycotoxins that are potent and can be toxic to humans. It grows in moist, humid conditions and cellulose-rich environments, such as plaster, wallpaper, and gypsum. Soap, water and bleach can be used to remove the mold.
This is a black mold that, if found in the environment, can cause severe, even life-threatening, allergic reactions/responses in some people. It is also responsible for causing "sick building syndrome" in some people. Sick building syndrome is a condition in which individuals suffer from symptoms of illness and feeling unwell, and the more time that is spent in a building contaminated with the mold causing this syndrome, the more severe the symptoms become. Individuals may notice they actually feel better when away from the building. Symptoms typically include headache, eye, nose, throat irritation, fatigue, brain fog, dizziness, and even nausea. Poor air quality associated with mold growth is the cause of these symptoms. The mold may be hidden and be growing due to dampness, moisture, a water pipe leak or burst, or after water damage due to leaks.
Most of the time, this mold is considered a contaminant but Stachybotrys alternans produces a very potent toxin that may be lethal. Reactions occur via inhalation of spores or absorption through the skin or traumatic injury. The mold is filamentous and produces spores. It is referred to as a "black mold". It produces mycotoxins that are potent and can be toxic to humans. It grows in moist, humid conditions and cellulose-rich environments, such as plaster, wallpaper, and gypsum. Soap, water and bleach can be used to remove the mold.

This fast-grower matures in 4 days, with a surface that starts out as white changing to black as it ages. The texture is cottony and spreading. The reverse starts out light and transforms to dark. Hyphae are septate and hyaline, some dark. Single or branched, the conidiaphores may be pigmented as seen in the image above, and rough. Colorless or pigmented phialides bear upper swellings with dark, oval conidia.
|
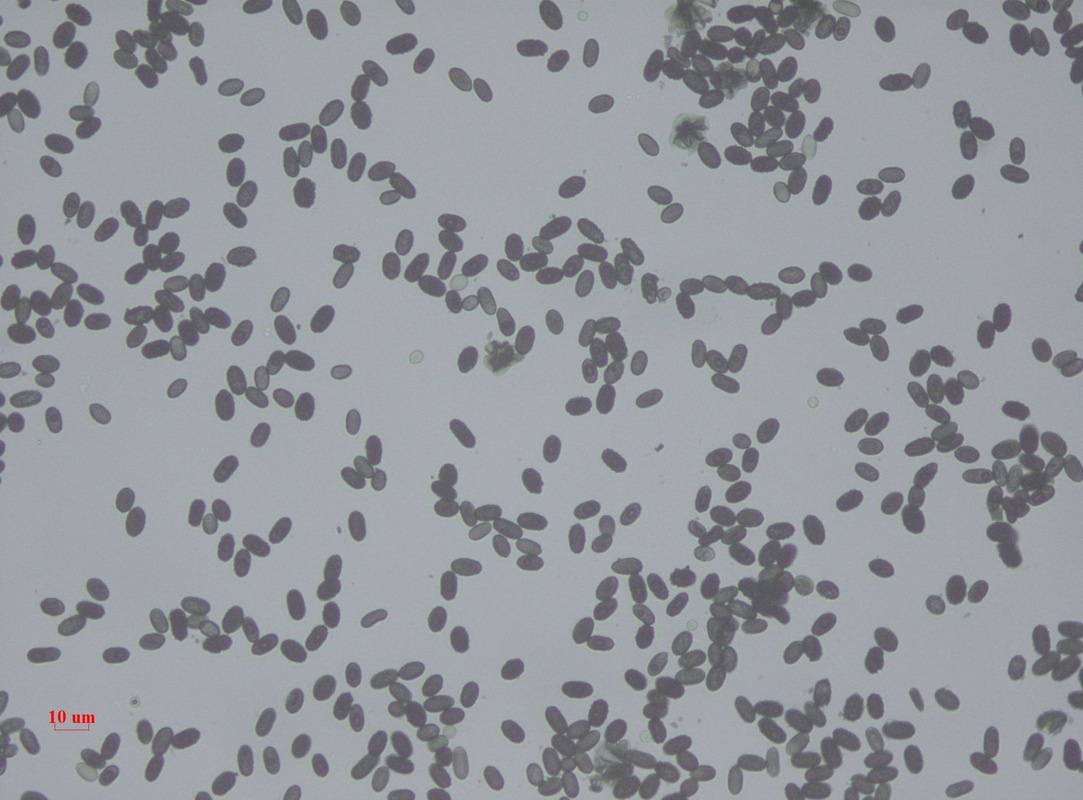
Oval, single-celled conidia with smooth or rough walls form in clusters. Sporulation and dispersion of spores seen here.By Dr. Sahay - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=28382983
|
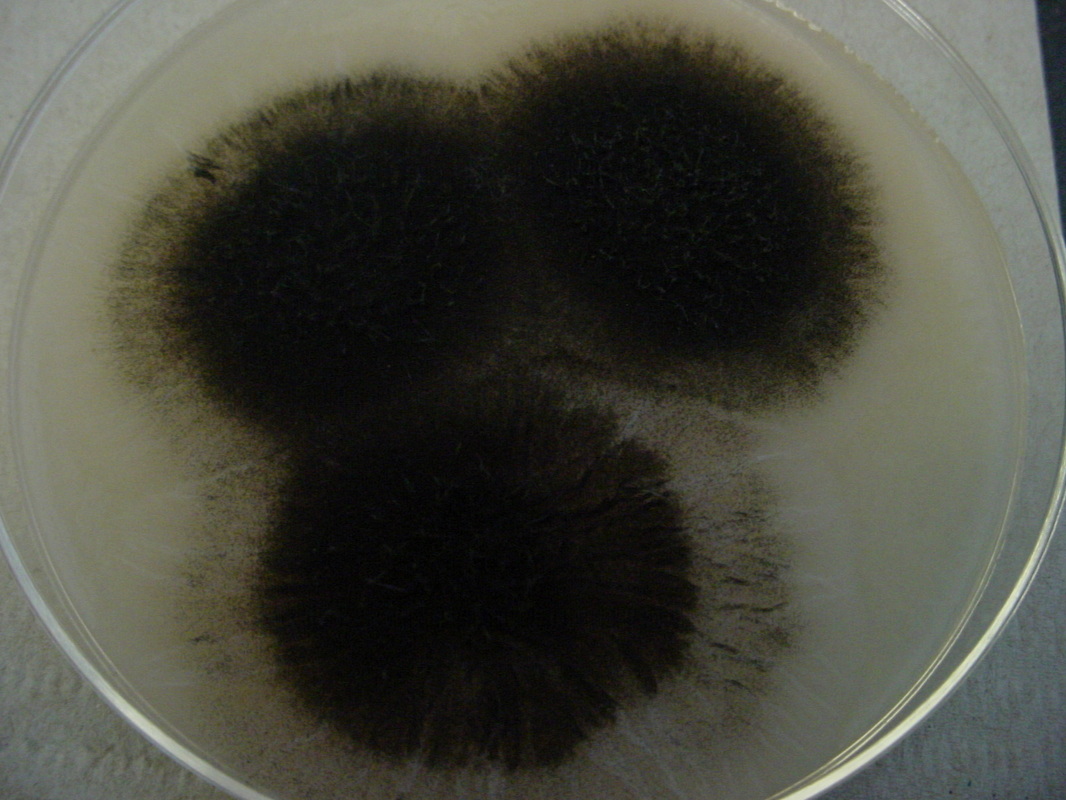
Black mold Stachybotrys
|
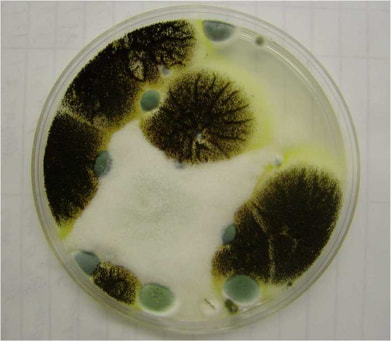
Stachybotrys (black) mold and Aspergillus molds growing on SABHI agar
|
Mycotoxins:
Some molds excrete potent toxins, or poisons, referred to as mycotoxins. Certain environmental conditions, such as moisture and humidity, water-damage, warmth, and pH provoke the production of such toxins, which are secondary metabolites produced by the molds. Unfortunately, low levels of fungicides have been linked to increased production of mycotoxins, a survival mechanism of molds, proving they are able to adapt and become stronger and hardier with time and resistant to fungicides. Some mycotoxins are lethal to both humans and animals.
Exposure to high levels of mycotoxins, or chronic exposure over time, can lead to symptoms in animals and humans, including neurological symptoms such as headaches, fatigue, brain fog, and nausea, as well as irritation to the mucous membranes and hypersensitivity reactions. Ingestion of mycotoxins, accidental traumatic entry into the body, inhalation of spores, and immune reaction to mold antigens are what result in symptoms if conditions are just right and the individual or animal is susceptible. Chronic exposure leads to chronic inflammation in some individuals, which puts them at higher risk for developing certain cancers. Mycotoxins are not constantly produced, but are only produced when conditions are just right. They are found on both the mold spore and on fragments of molds.
Types of mycotoxins include the following:
Human exposure is due to contaminated buildings and air that has been contaminated with substantial mold growth or from ingesting contaminated foodstuffs. Humidity, water-damage or water leaks, or floods can lead to environments that are just right for this type of mold growth, so prevention and treatment are key to stopping its growth and harmful effects. Another thing that many people are unaware of is furniture placement. If you block the air vents, you block ventilation, which can lead to mold growth inside the vents.
The US FDA closely monitors and inspects food, grains and animal feed to make sure they are free from contamination.
It is important to change your air filters monthly (unless otherwise stated) to reduce the risk of mold growth, allergies, asthma, and fungal infections. It is highly recommended that you clean the vents so that they remain free of dust and molds.
It is also highly recommended that you check to make sure all seals are intact, including those on your dishwasher, refrigerator, washing machine, and the bottoms of your doors, to prevent moisture buildup and toxic molds from growing. If you have a leak, get it repaired as soon as possible and clean it up to prevent mold growth. Remove wet laundry from the washing machine as soon as possible and put it in the dryer and make sure it dries thoroughly prior to putting it away.
Check expiration dates on products, use within the timeframe, and if you see any mold on cheeses, cereals, breads, vegetation, fresh flowers, etc..., throw them away to reduce the risk of exposure to molds.
Exposure to high levels of mycotoxins, or chronic exposure over time, can lead to symptoms in animals and humans, including neurological symptoms such as headaches, fatigue, brain fog, and nausea, as well as irritation to the mucous membranes and hypersensitivity reactions. Ingestion of mycotoxins, accidental traumatic entry into the body, inhalation of spores, and immune reaction to mold antigens are what result in symptoms if conditions are just right and the individual or animal is susceptible. Chronic exposure leads to chronic inflammation in some individuals, which puts them at higher risk for developing certain cancers. Mycotoxins are not constantly produced, but are only produced when conditions are just right. They are found on both the mold spore and on fragments of molds.
Types of mycotoxins include the following:
- Aflatoxins
- Carcinogenic compounds produced by some species of molds, including Aspergillus fumigatus and A. flavus, and may contaminate things like grains, peanuts, rice, cereals, breads, and are found in the environment. Most of the time this causes no harm in the healthy individual, but those with underlying immune disorders are at risk for illness.
- Aflatoxin B1, the most potent aflatoxin known thus far, is a known carcinogen, and is linked to A. flavus and A. parasiticus. It is linked to liver cancer. The WHO and CDC estimate that as much as 25% of food worldwide may actually be contaminated with aflatoxins. You should avoid consumption of moldy foods at all costs and frequently clean your refrigerator. This toxin is so potent that not only is it able to be ingested, but it also can permeate through the skin as well.
- It has been found in things like moldy peanuts, moldy cereals, moldy bread, fruit and vegetables, moldy grains, contaminated peanut butter and other things.
- It has been found in things like moldy peanuts, moldy cereals, moldy bread, fruit and vegetables, moldy grains, contaminated peanut butter and other things.
- Aflatoxin B2 is also produced by both molds.
- Aflatoxins M1 and M2 are also produced by A. parasiticus, but M2 is produced when the infected liver metabolizes aflatoxins B1 and B2.
- Aflatoxins G1 and G2 are also produced by both molds.
- Aflatoxin Q1
- Aflatoxicol
- Pillows have been linked to harboring over 40 species of molds and mycotoxins.
- High or chronic exposure can lead to illness, such as liver cancer, acute hepatic necrosis, or liver cirrhosis.
- Pillows have been linked to harboring over 40 species of molds and mycotoxins.
- Carcinogenic compounds produced by some species of molds, including Aspergillus fumigatus and A. flavus, and may contaminate things like grains, peanuts, rice, cereals, breads, and are found in the environment. Most of the time this causes no harm in the healthy individual, but those with underlying immune disorders are at risk for illness.
- Trilongins
- Trilongins are small toxic peptides containing amino acids, such as alpha-aminoisobutyric acid, which block ion channels in cells whose crucial role is to transport potassium and sodium between cells. This affects neurons, myocytes (heart cells), and muscle cells, which can cause problems with the neurological system, cardiovascular system, and muscular system. In addition to all this, the trilongins are resistant to heat and many antimicrobials. One common household mold that produces these is Trichoderma longibrachiatum.
- Trilongins are small toxic peptides containing amino acids, such as alpha-aminoisobutyric acid, which block ion channels in cells whose crucial role is to transport potassium and sodium between cells. This affects neurons, myocytes (heart cells), and muscle cells, which can cause problems with the neurological system, cardiovascular system, and muscular system. In addition to all this, the trilongins are resistant to heat and many antimicrobials. One common household mold that produces these is Trichoderma longibrachiatum.
Human exposure is due to contaminated buildings and air that has been contaminated with substantial mold growth or from ingesting contaminated foodstuffs. Humidity, water-damage or water leaks, or floods can lead to environments that are just right for this type of mold growth, so prevention and treatment are key to stopping its growth and harmful effects. Another thing that many people are unaware of is furniture placement. If you block the air vents, you block ventilation, which can lead to mold growth inside the vents.
The US FDA closely monitors and inspects food, grains and animal feed to make sure they are free from contamination.
It is important to change your air filters monthly (unless otherwise stated) to reduce the risk of mold growth, allergies, asthma, and fungal infections. It is highly recommended that you clean the vents so that they remain free of dust and molds.
It is also highly recommended that you check to make sure all seals are intact, including those on your dishwasher, refrigerator, washing machine, and the bottoms of your doors, to prevent moisture buildup and toxic molds from growing. If you have a leak, get it repaired as soon as possible and clean it up to prevent mold growth. Remove wet laundry from the washing machine as soon as possible and put it in the dryer and make sure it dries thoroughly prior to putting it away.
Check expiration dates on products, use within the timeframe, and if you see any mold on cheeses, cereals, breads, vegetation, fresh flowers, etc..., throw them away to reduce the risk of exposure to molds.
antifungal therapy agents for mycoses:
Overview:
Because fungi are eukaryotes, and our cells are eukaryote cells, unfortunately, many antifungals have side effects and some can be toxic to the liver and kidney, however, the benefits outweigh the risks in most cases. For this reason, it is critical to treat only true fungal infections and rule out contaminants and not prescribe antifungal agents unnecessarily. Antifungal treatments can be lifesaving measures.
Classes:
1. Polyene Macrolides:
According to Kern (1985), the polyene macrolides are the oldest and most potent, and they include amphotericin B (amp B) and Nystatin. In the early 1900's, Elizabeth Lee Hazen and Rachel Fuller Brown collaborated long-distance to develop Nystatin, the very first antifungal drug. Amp B was developed from the mold Streptomyces, and there is a low incidence of resistance.
Amp B is insoluble in saline with a pH of 7.0, so it is given with sodium deoxycholate in low doses, and it should be infused slowly. Rapid infusions have been known to cause infusion reactions, so a slow infusion rate can prevent this risk from occurring.
They are the most potent antifungals, and are typically saved for either systemic or disseminated fungal infections, or those not responding to other antifungals. They bind to ergesterol, a sterol in the plasma (cell) membrane, where they depolarize it. They work by inserting into the phospholipid bilayer membrane of the fungus, poking holes in it like a pin in a water balloon, which increases membrane permeability, causing the small molecules and cytoplasm to leak out.
IV Amp B is the empiric chosen therapy for suspected or confirmed systemic fungemia, especially in neutropenic or pancytopenic patients. It is used to treat the following conditions:
Since it is so potent, there are potential side effects and risks, which can occur as early as 1-3 hours after starting IV Amp B:
Preventative measures include providing adequate hydration with normal saline before and after the antifungal, as well as administration of potassium and magnesium supplements.
They include:
2. Pyrimidine Analogues:
5-Fluorocytosine (5-FC) is an antifungal in this class. It functions by incorporating into RNA and it makes a nonsense protein, which is dysfunctional. It also has the ability to stop the production of DNA by converting itself into a strong thymidylate synthetase inhibitor. In otherwords, this inserts "false building blocks" into DNA or RNA synthesis to "trick" the molecule, making it a nonfunctional one, thereby killing the fungus.
This antifungal is used to treat candidiasis, cryptococcosis, and chromoblastomycosis. It should be noted that many organisms are starting to show resistance to this antifungal medication. In severe cases of candidiasis or cryptococcosis, it canbe combined with Amp B to work synergistically and to lessen the chances of resistance. It can also be given in combination with fluconazole for candidiasis caused by Candida albicans, acting synergistically to enable the effects to last longer.
3. The Azole Antifungals (Azole Antifungals, 2024):
The azole class of antifungals is a big class, and these are very common and successfully used antifungals, and they can be administered topically, orally, or intravenously. They are divided into two groups: the triazoles and the imidazoles. They include:
The method by which the azoles function is that they bind to the heme (iron-carrying) plate of cytochrome P450 and this interferes with and blocks mixed oxidase functions and formation of ergosterol that is found in the cell membrane of the fungus. It inhibits their growth.
Most of the azoles are fungistatic, meaning the the levels are reduced significantly, but it does not kill them. Some of the topical formulations, on the other hand, are fungicidal (kill fungi).
The azoles are prescribed to treat body and skin infections, including athlete's foot, jock itch, vaginal candidiasis, ringworm, onychomycosis, candidiasis, cryptococcosis, blastomycosis, histoplasmosis, scedosporiosis, pityriasis versicolor, dermatophytosis (ringworm), aspergillosis, and sporotrichosis.
The new drug, rezafungin, has been FDA-approved and is an injection used to treat candidemia and invasive candidiasis. It is also known as Cidara, and it is taken 1x/week. It is an echinocandin and a broad spectrum antifungal that can be used to target aspergillosis and pneumocystis.
Oral ketoconazole or itraconazole are used to treat candidiasis in immunocompromised or immunosuppressed patients, particularly transplant patients, due to lower toxicity than other antifungals. Fluconazole is used to treat oral or esophageal candidiasis in AIDS patients. It absorbs well. More fungi are growing resistant to fluconazole, unfortunately. In this case, combining it with Amp B or itraconazole has shown to be more effective.
Fluconazole is also a drug of choice to treat cryptococcal meningitis.
Voriconazole is a triazone antifungal that is used if fluconazole is ineffective.
Oteseconazole (Mycovia) was developed in 2022 and it is FDA-approved from the treatment of recurrent (chronic) yeast infections in older women.
Ibrexafungerp is advantageous over fluconazole for vulvovaginal candidiasis, especially stubborn, resistant infections.
4. Griseofulvin (Mayo Clinic, 2024):
This antifungal is used to treat dermatophytosis of the skin, hair or nails. There is a tablet form, and it is found in Selsen Blue shampoo. It functions by interacting with polymerized microtubules and by unraveling the mitotic spindle during cell division, so it is fungicidal. There is an oral formulation for treatment of the dermatophytes and dermatophytosis, but treatment is ongoing until the infected skin, hair or nail has totally grown out and has been replaced by new ones. It is suggested by dermatologists that if a scalp or skin fungus is suspected, to try topical application with the shampoo containing this antifungal first to see if it will clear the fungal infection. The oral form needs to be taken with food, particularly a high-fat meal, where it will absorb better and be more effective (Mayo, 2024).
5. Allylamines:
The allylamines come in topical or oral formulations. Naftifine (Naftin) is a topical formulation. Lamisil (terbafine) is an oral or a topical formulation. They function by blocking squalene epoxidase, an enzyme that catalyzes ergosterol synthesis, which is a very potent process. These are used to treat the dermatophytes and dermatophytosis.
6. Echinocandins: (Drugs.Com, 2024)
The echinocandins are a class of antifungals that target the fungal cell wall, which is strong due to the presence of chitin, a polysaccharide. The echinocandins are lipopeptide molecules that inhibit (noncompetitively) an enzyme known as beta-d-glucan synthase enzyme. It forms a glucan, which is one of the building blocks of the fungal cell wall. It stops the building of the cell wall, so the fungus basically dies since its cell walls are now damaged. They include:
The echinocandins are used to treat invasive aspergillosis, candidiasis, candidemia, patients with neutropenia, systemic candidiasis, and are a drug of choice for prophylaxis treatment of fungal infections.
7. Flucytosine (Ancobon)
This is a potent antifungal often given along with amphotericin B. It is used to treat serious fungal infections that are systemic and invasive, such as bloodstream infections, fungal heart infections, lung infections, central nervous system infections, and stubborn urinary tract infections. It can have serious side effects, some of which can be severe, so it is closely monitored and reserved for difficult to treat infections.
Because fungi are eukaryotes, and our cells are eukaryote cells, unfortunately, many antifungals have side effects and some can be toxic to the liver and kidney, however, the benefits outweigh the risks in most cases. For this reason, it is critical to treat only true fungal infections and rule out contaminants and not prescribe antifungal agents unnecessarily. Antifungal treatments can be lifesaving measures.
Classes:
1. Polyene Macrolides:
According to Kern (1985), the polyene macrolides are the oldest and most potent, and they include amphotericin B (amp B) and Nystatin. In the early 1900's, Elizabeth Lee Hazen and Rachel Fuller Brown collaborated long-distance to develop Nystatin, the very first antifungal drug. Amp B was developed from the mold Streptomyces, and there is a low incidence of resistance.
Amp B is insoluble in saline with a pH of 7.0, so it is given with sodium deoxycholate in low doses, and it should be infused slowly. Rapid infusions have been known to cause infusion reactions, so a slow infusion rate can prevent this risk from occurring.
They are the most potent antifungals, and are typically saved for either systemic or disseminated fungal infections, or those not responding to other antifungals. They bind to ergesterol, a sterol in the plasma (cell) membrane, where they depolarize it. They work by inserting into the phospholipid bilayer membrane of the fungus, poking holes in it like a pin in a water balloon, which increases membrane permeability, causing the small molecules and cytoplasm to leak out.
IV Amp B is the empiric chosen therapy for suspected or confirmed systemic fungemia, especially in neutropenic or pancytopenic patients. It is used to treat the following conditions:
- Candidiasis
- Cryptococcosis
- Histoplasmosis
- Blastomycosis
- Paracoccidioidomycosis
- Coccidioidomycosis
- Aspergillosis
- Sporotrichosis
- Zygomycosis
Since it is so potent, there are potential side effects and risks, which can occur as early as 1-3 hours after starting IV Amp B:
- Renal toxicity
- Hypokalemia
- Hypomagnesia
- Anemia
- Fever and chills
- Headaches
- Drowsiness
- Weakness
- Dyspnea (air hunger, shortness of breath)
- Tachypnea
- Cardiac arrhythmias (vFib)
- Anaphylaxis
- Heart inflammation
- Decreased white blood cells
- Decreased platelets
Preventative measures include providing adequate hydration with normal saline before and after the antifungal, as well as administration of potassium and magnesium supplements.
They include:
- Nystatin is also known as Mycostatin or Nilstat or Biostatin. There are oral, vaginal suppository, and topical versions of this medication for candidiasis. There is no IV formulation for this medication, so there are fewer side effects than that of Amp B. It also must be administered for a longer period of time for it to work effectively.
- Amphoterecin B (discussed above) (also known as Fungizone, Amphotec, Amphocin, AmBisome, Abelcet)
2. Pyrimidine Analogues:
5-Fluorocytosine (5-FC) is an antifungal in this class. It functions by incorporating into RNA and it makes a nonsense protein, which is dysfunctional. It also has the ability to stop the production of DNA by converting itself into a strong thymidylate synthetase inhibitor. In otherwords, this inserts "false building blocks" into DNA or RNA synthesis to "trick" the molecule, making it a nonfunctional one, thereby killing the fungus.
This antifungal is used to treat candidiasis, cryptococcosis, and chromoblastomycosis. It should be noted that many organisms are starting to show resistance to this antifungal medication. In severe cases of candidiasis or cryptococcosis, it canbe combined with Amp B to work synergistically and to lessen the chances of resistance. It can also be given in combination with fluconazole for candidiasis caused by Candida albicans, acting synergistically to enable the effects to last longer.
3. The Azole Antifungals (Azole Antifungals, 2024):
The azole class of antifungals is a big class, and these are very common and successfully used antifungals, and they can be administered topically, orally, or intravenously. They are divided into two groups: the triazoles and the imidazoles. They include:
- Clotrimazole (Lotrimin): an imidazole
- Miconazole (Micatin, Monistat, Oravig): an imidazole
- Econazole: an imidazole
- Tioconazole: an imidazole
- Ketoconazole (Nizoral): an imidazole
- Itraconazole (Sporanox, Onmel, Tolsura): a triazole
- Fluconazole (Diflucan): a triazole
- Voriconazole (Vfend): a triazole
- Rezafungin (3/22/23)
- Oteseconazole (Vivjoa): (2022)
- Ibrexafungerp (Brexafemme)
- Posaconazole (Noxafil): a triazole
- Isavuconazole (Cresemba)
The method by which the azoles function is that they bind to the heme (iron-carrying) plate of cytochrome P450 and this interferes with and blocks mixed oxidase functions and formation of ergosterol that is found in the cell membrane of the fungus. It inhibits their growth.
Most of the azoles are fungistatic, meaning the the levels are reduced significantly, but it does not kill them. Some of the topical formulations, on the other hand, are fungicidal (kill fungi).
The azoles are prescribed to treat body and skin infections, including athlete's foot, jock itch, vaginal candidiasis, ringworm, onychomycosis, candidiasis, cryptococcosis, blastomycosis, histoplasmosis, scedosporiosis, pityriasis versicolor, dermatophytosis (ringworm), aspergillosis, and sporotrichosis.
The new drug, rezafungin, has been FDA-approved and is an injection used to treat candidemia and invasive candidiasis. It is also known as Cidara, and it is taken 1x/week. It is an echinocandin and a broad spectrum antifungal that can be used to target aspergillosis and pneumocystis.
Oral ketoconazole or itraconazole are used to treat candidiasis in immunocompromised or immunosuppressed patients, particularly transplant patients, due to lower toxicity than other antifungals. Fluconazole is used to treat oral or esophageal candidiasis in AIDS patients. It absorbs well. More fungi are growing resistant to fluconazole, unfortunately. In this case, combining it with Amp B or itraconazole has shown to be more effective.
Fluconazole is also a drug of choice to treat cryptococcal meningitis.
Voriconazole is a triazone antifungal that is used if fluconazole is ineffective.
Oteseconazole (Mycovia) was developed in 2022 and it is FDA-approved from the treatment of recurrent (chronic) yeast infections in older women.
Ibrexafungerp is advantageous over fluconazole for vulvovaginal candidiasis, especially stubborn, resistant infections.
4. Griseofulvin (Mayo Clinic, 2024):
This antifungal is used to treat dermatophytosis of the skin, hair or nails. There is a tablet form, and it is found in Selsen Blue shampoo. It functions by interacting with polymerized microtubules and by unraveling the mitotic spindle during cell division, so it is fungicidal. There is an oral formulation for treatment of the dermatophytes and dermatophytosis, but treatment is ongoing until the infected skin, hair or nail has totally grown out and has been replaced by new ones. It is suggested by dermatologists that if a scalp or skin fungus is suspected, to try topical application with the shampoo containing this antifungal first to see if it will clear the fungal infection. The oral form needs to be taken with food, particularly a high-fat meal, where it will absorb better and be more effective (Mayo, 2024).
5. Allylamines:
The allylamines come in topical or oral formulations. Naftifine (Naftin) is a topical formulation. Lamisil (terbafine) is an oral or a topical formulation. They function by blocking squalene epoxidase, an enzyme that catalyzes ergosterol synthesis, which is a very potent process. These are used to treat the dermatophytes and dermatophytosis.
6. Echinocandins: (Drugs.Com, 2024)
The echinocandins are a class of antifungals that target the fungal cell wall, which is strong due to the presence of chitin, a polysaccharide. The echinocandins are lipopeptide molecules that inhibit (noncompetitively) an enzyme known as beta-d-glucan synthase enzyme. It forms a glucan, which is one of the building blocks of the fungal cell wall. It stops the building of the cell wall, so the fungus basically dies since its cell walls are now damaged. They include:
- Rezafungin (Rezzayo)
- Micafungin (Mycamine)
- Anidulafungin (Eraxis)
- Caspofungin (Cancidas)
The echinocandins are used to treat invasive aspergillosis, candidiasis, candidemia, patients with neutropenia, systemic candidiasis, and are a drug of choice for prophylaxis treatment of fungal infections.
7. Flucytosine (Ancobon)
This is a potent antifungal often given along with amphotericin B. It is used to treat serious fungal infections that are systemic and invasive, such as bloodstream infections, fungal heart infections, lung infections, central nervous system infections, and stubborn urinary tract infections. It can have serious side effects, some of which can be severe, so it is closely monitored and reserved for difficult to treat infections.
references:
- Drugs.Com. Drug Classes: Anti-Infectives: Antifungals: Azole Antifungals. 2024. https://www.drugs.com/drug-class/azole-antifungals.html
- Centers for Disease Control and Prevention. Updated 2024. <https://www.cdc.gov/fungal/index.html>
- Cooper, Nancy (MLS-ASCP), 2015. Madigan Army Medical Center, Joint Base Lewis-McChord, Tacoma, WA (AFB/Mycology).
- Cornejo, Ana (MLS-ASCP), 2015. Madigan Army Medical Center, Joint Base Lewis-McChord, Tacoma, WA (AFB/Mycology).
- Emmons, C. Binford, C. Utz, J. Kwon-Chung, K.J. 1977 Medical Mycology, 3rd Edition. Philadelphia, PA.
- Gladwin, Mark; Trattler, Bill. 2008. Clinical Microbiology Made Ridiculously Simple, 4th Edition. MedMaster Inc., Miami, FL.
- Kern, M. Blevins, K. 1985. Medical Mycology: A Self-Instructional Text, 2nd Edition. F. A. Davis Company, Philadelphia, PA.
- Larone, Davise H. 2002. Medically Important Fungi: A Guide to Identification, 4th and 5th Editions. ASM Press, Washington, D. C.
- Mayo Clinic. 2024. Drugs and Supplements. https://www.mayoclinic.org/drugs-supplements/griseofulvin-oral-route/side-effects/drg-20064116?p=1
- McGinnis, M. D'Amato, R. Land, G. 1982. Pictorial Handbook of Medically Important Fungi and Aerobic Actinomycetes. Praeger Publishers, New York, NY.
- Public Health Image Library, CDC. Accessed 2024. <https://phil.cdc.gov/>
- Reynolds, Jeanette (MS-Biology, Certified in Emerging Diseases, M-ASCP, MLS-AMT). Personal Clinical Lab, Teaching and Writing Experience: Landstuhl Regional Medical Center, Germany, 2007-2010; Penrose Hosp, 2010-2012; NAU 2010-2012; MAMC, Fort Carson, Colorado Springs, CO 2010-2012; Brook Army Medical Center in Association With Medical Education and Training Center, Fort Sam Houston, San Antonio, TX 2013-2014; Joint Base Lewis-McChord, Tacoma, WA 2015-2016; Pierce College, Tacoma, WA 2015-2016; El Paso Community College and DaVinci School for Science and the Arts, TX, 2016-2017; Prisma Health 2017-2019; Lexington Medical Center 2014 and 2019-Present/Current; On Course Learning (CE Modules) 2016-Present; APass Education Writing (CE Modules/Test Questions) 2016-Present, Fortis College, Columbia, SC (2019-2022), Lexington Medical Center (2019-present), Southwestern Community College (2022-present), Relias Writing Contractor (2016-present)
- Westblade, L. Burd, E. Lockhart, S. Procop, G. 2023. Larone's Medically Important Fungi, A Guide to Identification, 7th Edition. ASM Press, Washington, D.C.
