Hand Hygiene and cleaning:
Proper hand hygiene cannot be emphasized enough, whether it be in the hospital setting, a clinic, a school, or a public place. The hospital setting is critical, because there are a number of microbes that can be easily transmitted, which can cause infectious, some of which can be serious or even deadly. Did you know that Norovirus (the most common virus that causes vomiting and diarrhea) and Clostridioides difficile are two microbes that are not destroyed by alcohol-based hand sanitizers? For this reason, washing one's hands with soap and water for at least 20 seconds is critical.
For the microbes that are not destroyed by alcohol-based hand sanitizers, and for dirt or other organic material that would be smeared by it, the best means of removal is soap and water. Soap acts as a surfactant, meaning that it has two ends, one of which binds to dirt or oils, and the other of which binds to water, which is removes it. The water-loving end is "hydrophilic" and the water-repelling end is "hydrophobic". Surfactants reduce the surface tension of water, "bending" the bonds so it can spread out easier. This is the chemical action of soap. The mechanical action of scrubbing the hands, creases, nails, palms, and backs of the hands removes dirt and organic material as well. The thermal action of warm water washes it all down the drain.
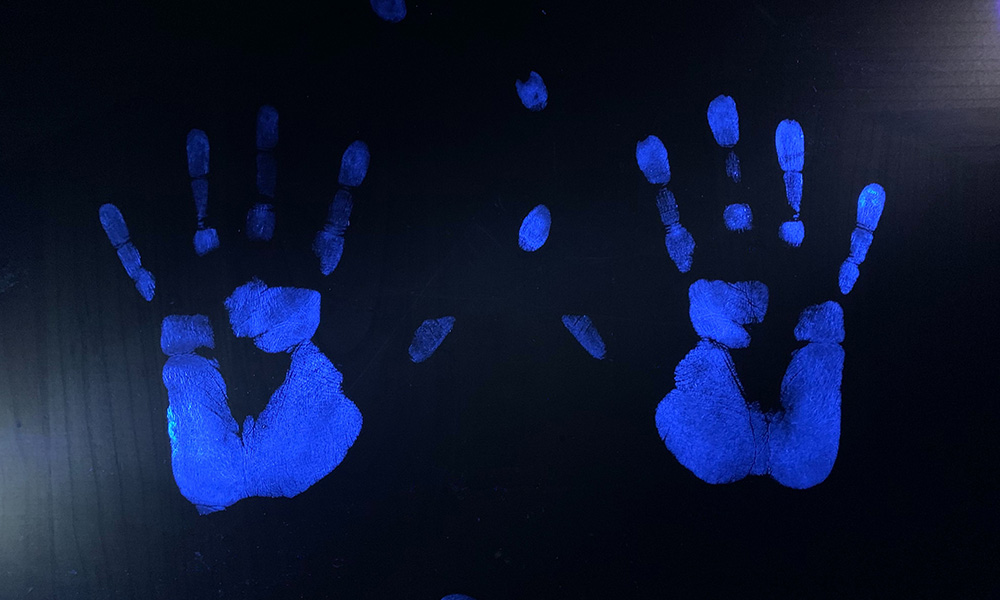
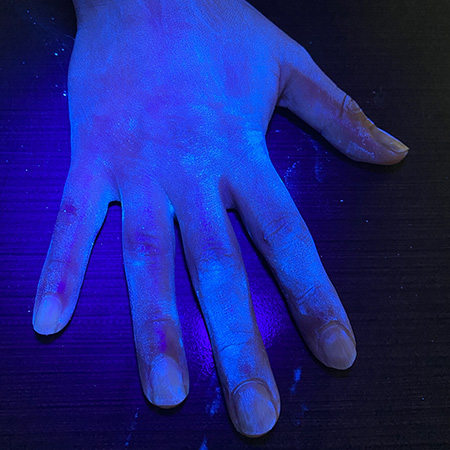
One of my favorite experiments has always been to perform the "GloGerm" experiment with students to show how and where microbes stick to the hands and to surfaces, and how and why it is so important to remove them. The GloGerm powders and lotions are meant to simulate microbes, including viruses, bacteria, fungi and parasites that might be contaminating surfaces and hands. Microbes are ubiquitous, meaning they are everywhere! Everything from your car door handle to your steering wheel to your cell phone to door knobs, vending machines, work areas, keyboards, are all subject to contamination by microbes. We can't see them with the naked eye. We can see bacteria, yeasts, molds, and protists with a Brightfield compound light microscope, however, viruses are still too tiny to be seen with this type of tool. They can only be seen with a scanning or a transmission electron microscope.
For the microbes that are not destroyed by alcohol-based hand sanitizers, and for dirt or other organic material that would be smeared by it, the best means of removal is soap and water. Soap acts as a surfactant, meaning that it has two ends, one of which binds to dirt or oils, and the other of which binds to water, which is removes it. The water-loving end is "hydrophilic" and the water-repelling end is "hydrophobic". Surfactants reduce the surface tension of water, "bending" the bonds so it can spread out easier. This is the chemical action of soap. The mechanical action of scrubbing the hands, creases, nails, palms, and backs of the hands removes dirt and organic material as well. The thermal action of warm water washes it all down the drain.
One of my favorite experiments has always been to perform the "GloGerm" experiment with students to show how and where microbes stick to the hands and to surfaces, and how and why it is so important to remove them. The GloGerm powders and lotions are meant to simulate microbes, including viruses, bacteria, fungi and parasites that might be contaminating surfaces and hands. Microbes are ubiquitous, meaning they are everywhere! Everything from your car door handle to your steering wheel to your cell phone to door knobs, vending machines, work areas, keyboards, are all subject to contamination by microbes. We can't see them with the naked eye. We can see bacteria, yeasts, molds, and protists with a Brightfield compound light microscope, however, viruses are still too tiny to be seen with this type of tool. They can only be seen with a scanning or a transmission electron microscope.
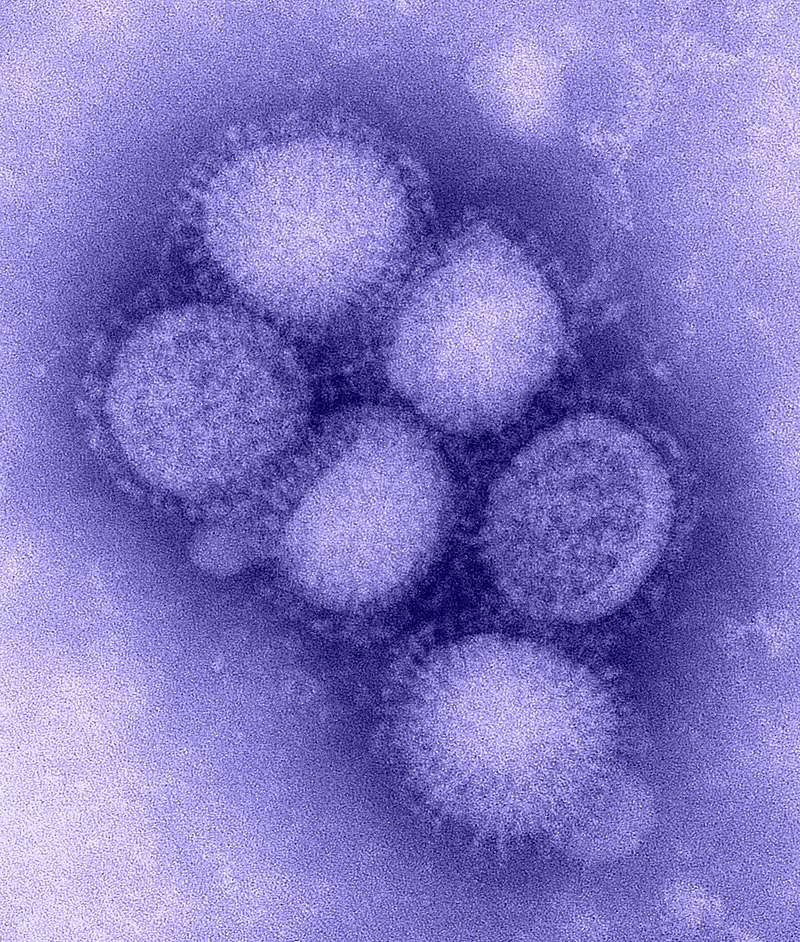
A virus: Influenza A (H1N1), https://upload.wikimedia.org/wikipedia/commons/thumb/f/f0/H1N1_influenza_virus.jpg/800px-H1N1_influenza_virus.jpg
|
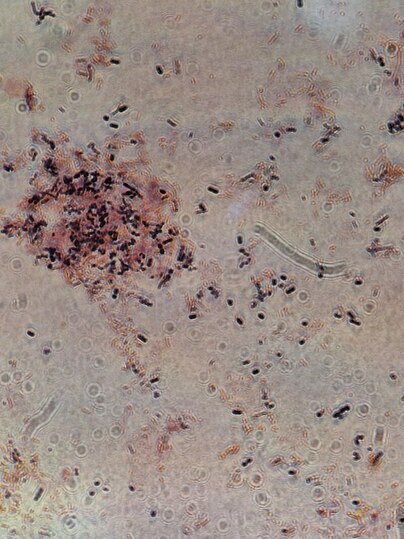
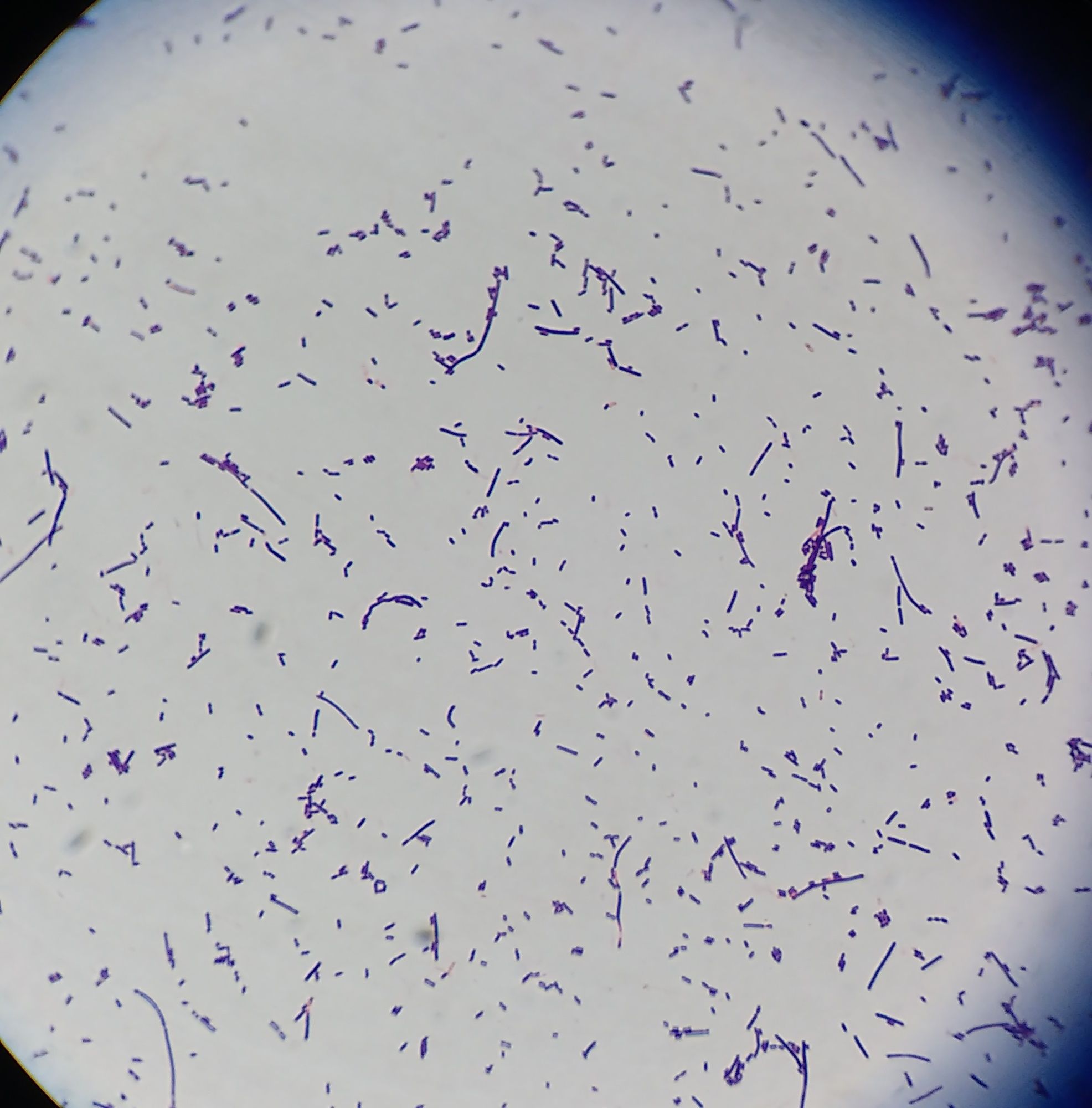
Bacteria: C. difficile; https://upload.wikimedia.org/wikipedia/commons/thumb/f/f7/Clostridium_difficile_gram_stain.jpg/800px-Clostridium_difficile_gram_stain.jpg
|
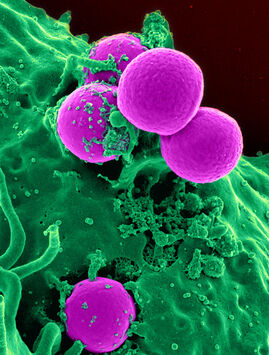
MRSA: https://upload.wikimedia.org/wikipedia/commons/thumb/0/01/Human_neutrophil_ingesting_MRSA.jpg/800px-Human_neutrophil_ingesting_MRSA.jpg
|

A protist: Trichomonas vaginalis (an STD); https://upload.wikimedia.org/wikipedia/commons/b/b9/Trichomonas_Giemsa_DPDx.JPG
|
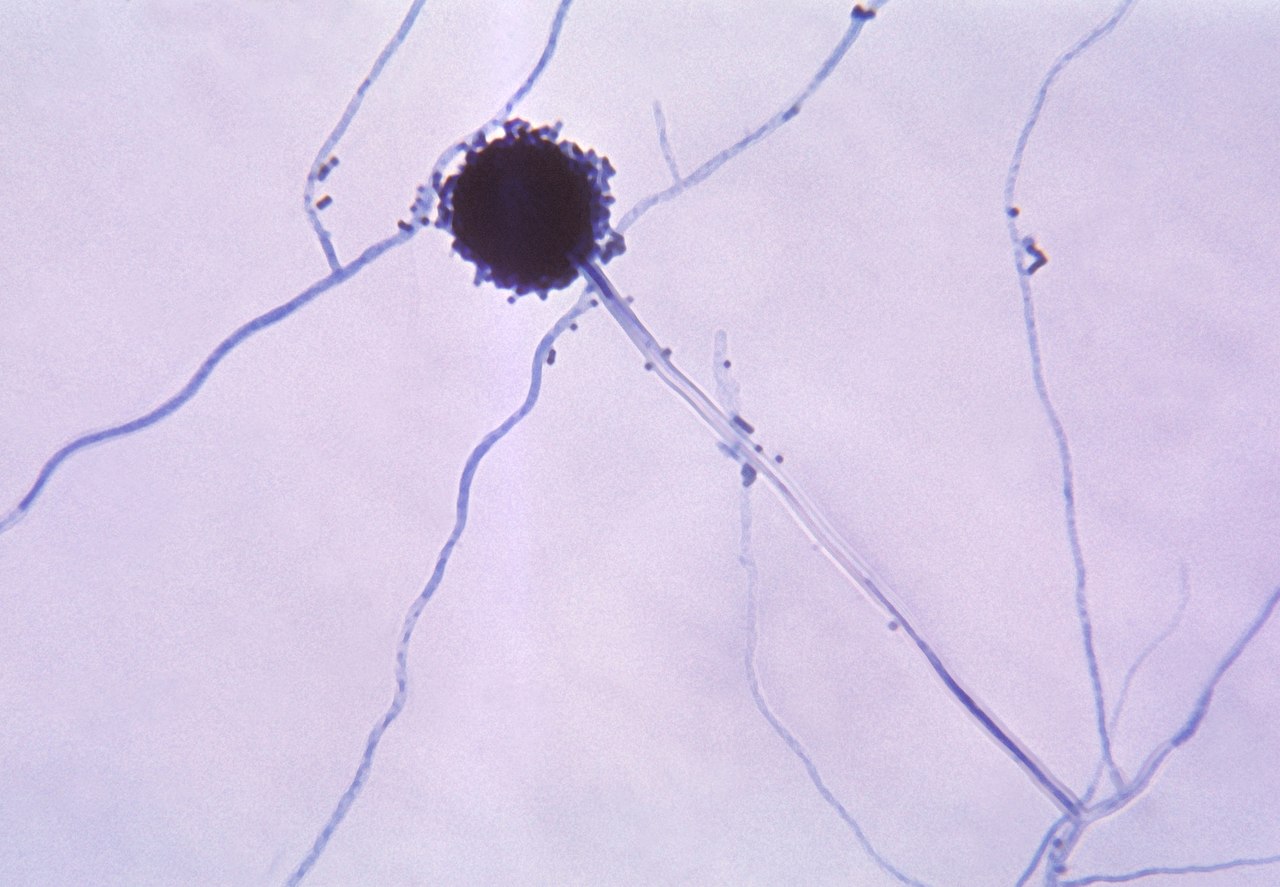
A fungus (Aspergillus spp mold); https://upload.wikimedia.org/wikipedia/commons/thumb/7/74/Aspergillus_niger_01.jpg/1280px-Aspergillus_niger_01.jpg
|
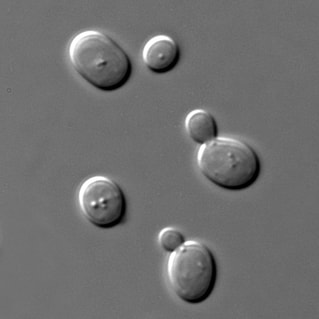
A yeast (Candida albicans); https://upload.wikimedia.org/wikipedia/commons/thumb/d/d9/S_cerevisiae_under_DIC_microscopy.jpg/1024px-S_cerevisiae_under_DIC_microscopy.jpg
|
https://i.pinimg.com/originals/3b/24/6c/3b246c6af0d9c77f6ad80b9a31b75aaa.jpg
|
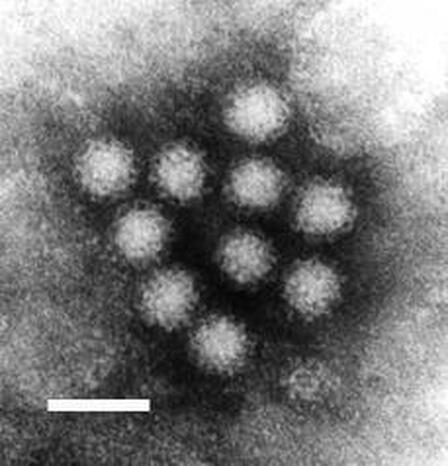
A virus: Norovirus (https://upload.wikimedia.org/wikipedia/commons/7/7b/Norwalk.jpg)
|
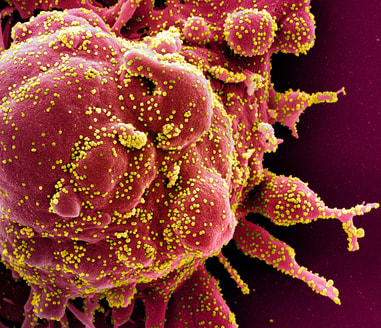
A virus: SARS-Covid-19 (yellow) and an antibody from the immune system (red); https://www.nih.gov/sites/default/files/news-events/research-matters/2020/20200630-covid-pink.jpg
Surfactants:
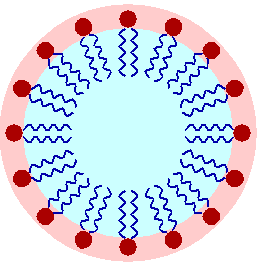
https://upload.wikimedia.org/wikipedia/commons/b/bb/A_lipid_micelle.png
|
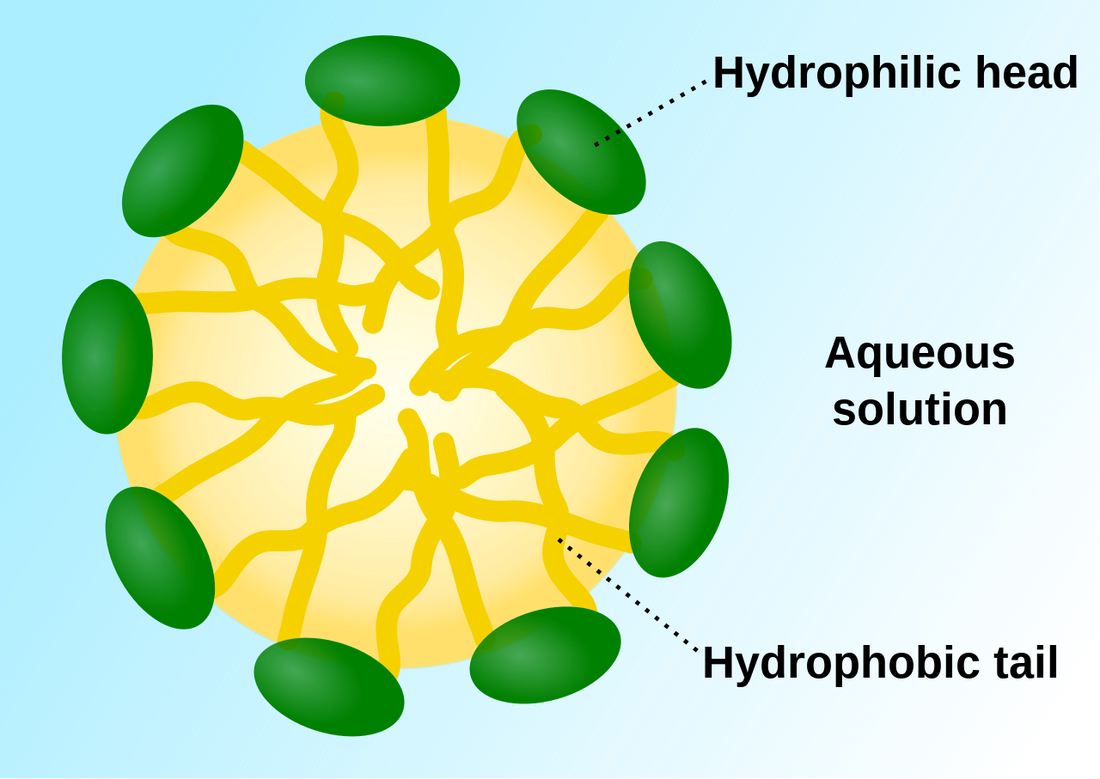
https://upload.wikimedia.org/wikipedia/commons/thumb/4/4d/Micelle_scheme-en.svg/1280px-Micelle_scheme-en.svg.png
|
How to perform the glogerm experiment:
Handwashing Training:
"1. Shake the bottle of Glo Germ oil well and place a small amount, about the size of a quarter, into the palm of one hand and spread over both hands completely as if applying hand lotion. Be sure to cover hands completely, particularly under nails, around cuticles and between fingers. Wipe off excess with paper towel. Do not let oil contact clothing as staining may result. When using white Glo Germ gel, use same procedure with a pad of gel about the size of a nickel. Wiping off excess is usually not necessary.
2. Place hands under UV lamp to view “glowing germs” that exist before hand washing. Demonstration works best in a darkened room.
3. Perform the FDA-recommended hand wash using soap and warm water. The amount of effort required to remove the simulated germs is equal to that of removing most bacteria.
Again, place hands under UV lamp, paying special attention to thumbs, areas around nails and between fingers, The UV lamp reveals the remaining “germs” as proof of improper hand washing.
4. Complete removal of Glo Germ with normal washing is more difficult if skin is chapped or cracked, indicating that bacteria is also harder to remove. This will require a hand care regime with a quality lotion twice daily and a judicious use of a hand sanitizing gel.
Surface Cleaning1. Lightly dust a small amount of Glo Germ powder over an entire surface area.
5. Clean the surface until all visible powder disappears.
6. Pass the UV lamp over the surface; the remaining traces of powder will glow on the areas that weren’t washed thoroughly. When checking restroom areas for cleanliness, UV lamp may be used for the detection of urine without using Glo Germ powder.
Food Cross-Contamination1. Sprinkle powder very lightly over a head of lettuce, tomato or another fruit or vegetable to be processed by trainees so that powder is not visible in ordinary light. Food used is to be discarded after demonstration.
7. Have trainee’s process food using their normal procedure and kitchen utensils.
8. Use UV lamp to show how the “glowing germs” are spread to hands, cutting boards, knives and to other foods." (Glo Germ, https://www.glogerm.com/handwashing.html)
"1. Shake the bottle of Glo Germ oil well and place a small amount, about the size of a quarter, into the palm of one hand and spread over both hands completely as if applying hand lotion. Be sure to cover hands completely, particularly under nails, around cuticles and between fingers. Wipe off excess with paper towel. Do not let oil contact clothing as staining may result. When using white Glo Germ gel, use same procedure with a pad of gel about the size of a nickel. Wiping off excess is usually not necessary.
2. Place hands under UV lamp to view “glowing germs” that exist before hand washing. Demonstration works best in a darkened room.
3. Perform the FDA-recommended hand wash using soap and warm water. The amount of effort required to remove the simulated germs is equal to that of removing most bacteria.
Again, place hands under UV lamp, paying special attention to thumbs, areas around nails and between fingers, The UV lamp reveals the remaining “germs” as proof of improper hand washing.
4. Complete removal of Glo Germ with normal washing is more difficult if skin is chapped or cracked, indicating that bacteria is also harder to remove. This will require a hand care regime with a quality lotion twice daily and a judicious use of a hand sanitizing gel.
Surface Cleaning1. Lightly dust a small amount of Glo Germ powder over an entire surface area.
5. Clean the surface until all visible powder disappears.
6. Pass the UV lamp over the surface; the remaining traces of powder will glow on the areas that weren’t washed thoroughly. When checking restroom areas for cleanliness, UV lamp may be used for the detection of urine without using Glo Germ powder.
Food Cross-Contamination1. Sprinkle powder very lightly over a head of lettuce, tomato or another fruit or vegetable to be processed by trainees so that powder is not visible in ordinary light. Food used is to be discarded after demonstration.
7. Have trainee’s process food using their normal procedure and kitchen utensils.
8. Use UV lamp to show how the “glowing germs” are spread to hands, cutting boards, knives and to other foods." (Glo Germ, https://www.glogerm.com/handwashing.html)
Experiment, by jeanette (jen) reynolds:
Learning Objectives:
Upon completion of these exercises, you will be able to:
- Explain how viruses are transmitted and spread through a population of humans.
- Differentiate between means of direct and indirect contact, droplets, aerosols, food borne, and vector borne transmission.
- Explain how asymptomatic individuals can transmit viral and other microbial illnesses.
- Name some reservoirs of disease, vectors, and fomites.
- Describe the best means of prevention of the spread of viruses.
- Discuss the role of vaccinations, immunizations, and the immune system in fighting off viral diseases.
- Explain the viral infection process and steps of infection through recovery.
- Explain why antibiotics are ineffective for treating viral infections.
- Describe general signs and symptoms of viral infections.
- Differentiate between acute and chronic illnesses.
- Discuss how various soaps and cleaners effectively kill viruses.
Materials Needed:
- GloGerm Lotion, Powder
- UV Lights
- Water, Soap
- Alcohol-Based Hand Sanitizers
- Paper Towels
- Computer
Listen to This Awesome Podcast: https://www2c.cdc.gov/podcasts/media/mp4/HandHygieneSavesLives_Short_OC.mp4
PART A: Transmission: The Spread of Viruses: (Read This Part and Use This Part to Answer the Questions)
Viruses spread (they are transmitted) in a number of ways, depending upon the type of virus.
Some important terminology to help you understand this section is as follows:
- Source: a place where an infectious agent hides out, such as a sink, the skin, a doorknob, a keyboard, a chair, a bedrail, a ceiling tile, a mirror, a faucet, a table, a countertop, a knob, and the microbe itself (a virus, bacterium, parasite, fungus or prion)
- Dry
- Wet (Examples: biofilm, water, stain, leak, spill, faucet, sink, cooling tower, ventilator, wet carpet)
- Indwelling medical device, such as a foley catheter, PICC line, port, IV line, etc...)
- Dust (construction, wet cellulose from wood or ceiling tiles or wallpaper)
- Fomite: an inanimate, nonliving source of transmission of disease
- Vector: a living carrier of a microbe or disease, and can be a healthcare worker, a patient, a visitor, an insect, an animal, or anything or anyone living
- Transmission: the means in which a microbe passes from one person to another or from a source to a susceptible person
- Touching something (contact), then touching the patient
- Splashes
- Aerosolization and sprays when coughing or sneezing, creating droplets that can travel up to 6 feet, which can land on a person's mucous membranes (conjunctiva, nose, mouth)
- Bigger droplets, which don't travel as far, but can still be inhaled, or which can land on surfaces
- Inhalation of aerosols that stay in the air for longer periods of time and can travel great distances (30 feet) and can travel in air currents when the sick person talks, coughs or sneezes
- Ingestion of contaminated food or water
- Puncture (sharps, bites, etc...)
- Susceptible: at risk for infection
- Unvaccinated individual
- Underlying illness, cancer, type 2 diabetes
- Broken skin/wound
- Post-surgery
- On certain types of medications, such as immunosuppressants or chemotherapy or certain antibiotics
- A person with an autoimmune disease or a compromised or weak immune system
- An individual with an indwelling device of any type
- A person who has had an organ transplant
- A person who is intubated or who is on a ventilator
- Host: a person carrying a disease
- Reservoir: harbors a pathogen that could cause a disease, and may be colonized with a microbe
- Carrier: a vector is an example of a carrier, but this is something or someone living that is harboring, colonized with, or infected with a microbe, however, they have no symptoms (they are asymptomatic) but they can still transmit it to others
Contact Transmission: This is the most common mode of transmission, and it is subdivided into two subgroups.
- Direct contact:
- Person-to-person: shaking hands, kissing, bodily fluids, blister fluid, blood, mucous membranes, breaks/cuts/abrasions in the skin
- Mites from a scabies-infested patient are transferred to the skin of a caregiver’s skin
- Indirect contact:
- Infected animals (reservoirs) can harbor disease and spread it to a person.
- Touching a contaminated surface (doorknob, computer keyboard, desk, phone, etc…)
- Fomite (inanimate object): clothing, linens, towels, bedding, a surgical instrument, chair, ceiling tile, mirror, bedrail, chair rails, thermometer, point-of-care instrument, stethoscope, blood pressure cuff, cart, toy, endoscope, clothing, scrubs, lab coats, isolation gowns, soiled garments, etc…
- Carriers: living people or animals that can be harboring a virus or other microbe, remain asymptomatic and never produce any symptoms, but can still transmit/pass it on to others, who may become very ill
- NOTE: This is why it is important to prevent transmission the best that you can.
- Airborne or aerosolized droplets (sneezing, coughing, talking, singing, suctioning, endotracheal intubation, chest physiotherapy, CPR, vomiting, diarrhea, even whispering or breathing)
§ 5-10 micrometers in size (airborne respiratory droplet)
§ <5 micrometers (aerosol droplet)
· These can stay in the air for up to 9 hours!
· They can travel up to 30 feet in a big sneeze!
§ Average distance they travel: 3 feet
§ A Few Examples: the common cold (upper respiratory infection), influenza virus, Covid-19, pneumonia, stomach viruses like Enterovirus or Norovirus, which can cause vomiting, diarrhea, headache, fatigue, and spread quickly, viral sore throat, viral ear infection)
- Foodborne or waterborne (eating or drinking something that is contaminated with the virus particles)
- Vector Borne (carried by an arthropod: an insect like a mosquito or a tick, a fly, a flea, a rat or other vermin, a bite or scratch)
Transmission-Based Precautions:
In the hospital setting, transmission-based precautions are designed to protect both the patient and the healthcare workers, as well as family members who may be with the patient or be visiting. These address the specific need for specific PPE to be worn during interactions with patients, their family members, and the surrounding environment, depending on where they are. The PPE required is based upon the type of infectious agent and the mode of transmission. The three main types include: contact, droplet and airborne, but there are some modifications and combinations of these, as you will read below, depending upon the disease.
It should be noted that these are in addition to Standard Precautions. The amount of time that precautions are needed depends on each facility's policy and is linked to the type of disease and mode of transmission, and each has its own unique timeframe. These are considered on a case-by-case basis, since patients may have underlying conditions or responses to microbial disease that warrant a longer time on the precaution. Infection prevention and nurses and their leadership work together to decide this in these types of situations.
If a patient has an alert for a precaution, a specific sign should be posted on their door so that everyone going into the room knows to follow specific guidelines for that precaution, including wearing specific PPE. The signs should be left on the door even after the patient is discharged so that the staff coming in to clean the room will know that they will also need to wear special PPE when they clean the room. It helps to have signs that are able to be easily wiped off with sanitizing wipes.
1. Contact Precautions:
Contact precautions are designed to prevent the spread of infections by skin-to-skin contact (direct contact) or through touching a contaminated object (indirect contact or fomite).
- MRSA or history of MRSA (methicillin-resistant Staphylococcus aureus)
- MDRO or VRE (a multidrug-resistant organism, particularly in the blood, or vancomycin-resistant Enterococcus faecalis)
- RSV (respiratory syncytial virus)
- Try to place the patient in a single room or space, if available
- PPE: gown and gloves for all patient contact, donning PPE prior to room entry, and doffing prior to exit to contain pathogens; don clean PPE prior to transport of a patient on contact isolation precautions
- Hand hygiene: before entering the room and putting on gloves and after removing gloves prior to leaving the room, as well as prior to transporting a patient
- Transport: only move patients if medically necessary for a procedure or transfer, making sure to cover the colonized or infected area(s)
- Patient care equipment: should be disposable or dedicated, and frequently cleaned with something like Cavicide wipes
- Cleaning: the cleaning and proper disinfection of rooms should be prioritized daily and between patients; clean frequently touched surfaces, such as light switches, doorknobs, tables, bed rails, chair rails
Another fact is that Enterococcus can survive fo months in the digestive or urogenital tract. This is called "colonization". In susceptible individuals, it can cause an opportunistic infection, such as a UTI, sepsis, endocarditis, meningitis, a wound infection, etc...If an individual was previously treated with an antibiotic like vancomycin or a combination like penicillin and gentamicin, and if they are hospitalized, or if they are on long-term antibiotic therapy, they can become very ill.
If a person is elderly, if they have an underlying illness, are immunocompromised or immunosuppressed, they are in the ICU, they have diabetes type 2, have cancer, or on certain medications, or those who have had surgery, are all at higher risk for infection. Those with indwelling urinary catheters, central intravenous catheters, ports, are all at higher risk for infection.
2. Aerosolization/Droplet Precautions:
Droplet precautions are important because they can help prevent the spread of infectious disease that travels in respiratory droplets. Droplets are >5 microns, travel short distances through the air currents, then land on surfaces. PPE should include a mask for the healthcare worker and the patient.
- Meningitis
- Pertussis (whooping cough)
- Influenza A, B
- SARS Covid 19
- Pneumonia
- Source: put a mask on the patient
- Try to put the patient in a single patient room or space if possible
- Teach the patient how to use respiratory and cough hygiene techniques
- PPE: don a mask before you enter the patient's room
- Transport: try to limit transport to medically necessary procedures or transfers, and if this is needed, then put a mask on the patient and yourself
Airborne precautions are put into place to prevent the transmission of the tiny respiratory particles <5 microns that can stay suspended in the air for longer periods of time. These precautions have a special requirement to use a negative air pressure room with the door closed if a room is available. A fit tested N95 respirator or PAPR should be worn.
- Mycobacterium tuberculosis (TB)
- This organism typically attacks the lungs, but extrapulmonary types can and do occur, including the bone, tissue, brain, joints, kidneys, and lymphatic system
- It is transmitted if an infected individual coughs, sneezes, speaks, or sings
- Symptoms: fatigue, coughing up blood, fatigue, weight loss, loss of appetite, low-grade fever
- Signs: Abnormal chest X-ray, + PPD test, + sputum culture with AFB
- Risks: foreign travel to places where it is endemic, born in an area where it is endemic, those who live in or work at a long-term care facility, the homeless, IV drug users, those who are immunocompromised, those who are immunosuppressed, HIV/AIDS + individuals
- Prevention: recognize symptoms, follow proper isolation, follow proper PPE protocol, ensure entire and complete treatment regime is followed
- This organism typically attacks the lungs, but extrapulmonary types can and do occur, including the bone, tissue, brain, joints, kidneys, and lymphatic system
- Measles
- Chickenpox
- Disseminated Herpes zoster (shingles)
- Nontuberculosis mycobacterium
- Aspergillus (mold)
- Source: put a mask on the patient
- They need to be in an airborne infection isolation room (AIIR), which is often a negative pressure room or a private room with the door closed (if an AIIR is not available)
- Healthcare Professionals: If susceptible, they should be restricted from entering the room if at all possible
- PPE: A fit-tested N-95 mask should be worn in addition to other PPE
- Transport: transport should be limited to medically necessary procedures or transfers, and the patient should wear a surgical mask, observe respiratory/cough hygiene and etiquette, and make sure any infectious lesions are covered up
- Immunization: offer immunization of susceptible individuals as soon as possible if they are exposed to someone with an airborne disease
Bloodborne pathogens standards were developed by the Occupational Safety and Health Administration (OSHA). They monitor and enforce these standards in hospitals, clinics, schools, and other settings in order to protect workers. These standards have a goal of minimizing the risk of exposure to bloodborne pathogens found in blood and body fluids and other potentially infectious materials, including tissues, organs, cellular material, and anything considered to be biohazardous waste.
These standards apply to every type of employer and employee who have a risk of occupational exposure to blood, body fluids, potentially infectious materials, skin, eye, mucous membrane, or a potential puncture, which may result from handling such materials. These standards also include the Neeldestick Safety and Prevention Act of 2000.
Employers are required to make sure that they identify, evaluate and put into place the safest medical devices possible. This includes things like Sharps containers, biohazardous waste containers, proper labels identifying them as such, protective needle covers or needleless systems. This also means that logs are kept for maintenance, and for recording any injuries related to such materials, and working to improve always. All of these places should have an Exposure Control Plan in place, such as who and where to report an exposure to, and how it will be handled.
Pertinent areas with facilities where exposures may occur should have eyewash stations and handwashing stations readily available, and some will also have showers available. These should be tested on a weekly basis, cleaned, and a log should be kept to make sure that they are functioning properly. Sharps containers with securely-fitted lids and methods of waste disposal are all methods of exposure control. There should never be any recapping or reusing of needles and no bending of needles in order to protect the worker and the patient.
Working safely and cautiously will help to prevent spraying or generating aerosols or droplets that could potential infect the worker, as will wearing appropriate PPE to create a barrier of protection. Being up-to-date on one's vaccinations can also help protect against infections. Treat all blood and body fluids and potentially infectious materials as if they were contaminated.
- HIV/AIDS
- HBV
- HCV
This type of precaution involves more than just the typical contact precautions. Unfortunately, alcohol-based hand sanitizers are unable to kill the endospores produced by Clostridium difficile. They also do not destroy Noroviruses. The best means of destroying these organisms is handwashing with soap and water. DO NOT used alcohol-based hand sanitizer as a substitute for handwashing with soap and water. PPE that should be worn includes gown and gloves.
Norovirus spreads fast, causes dehydration very quickly, and people who are sick with this organism can literally shed billions of the virus particles. The viral load needed for someone to become ill is minimal, and it an spread through direct contact, ingesting contaminated food and water, or by touching a contaminated surface.
- Gastroenteritis
- Norovirus
- C. difficile
This combination transmission precaution type is used in addition to standard precautions. This is put into place if a patient has COVID-19. PPE should include eye protection, a mask, preferably an N95 or PAPR if aerosol-generating procedures will be performed, gowns and gloves. The door to the patient's room should remain closed.
Standard Precautions:
According to the standards set by the CDC (Centers for Disease Control and Prevention), in the hospital and clinical healthcare setting, standard precautions are put into place to prevent the spread of disease. They are used for ALL patient care, so when YOU go to the doctor, or if you yourself are planning to go into healthcare, these are based on a risk assessment and include use of common sense practices and use of special personal protective equipment (PPE) to protect providers from infection and to prevent transmission of infection from person-to-person. Other components of standard precautions include:
- Respiratory hygiene and cough etiquette (cough into the crease of your elbow or sneeze into the crease of your elbow if you don't have any tissue paper to prevent spread of aerosols or droplets)
- Wear a mask if you are experiencing respiraory symptoms and try to maintain some distance from others
- Use safe injection practices and aseptic technique if you are a healthcare provider giving vaccinations or administering fluids or drawing blood or performing a special lumbar procedure
- Cleaning and disinfection of surfaces and equipment for the appropriate amount of time to decontaminate them
- Good hand hygiene
- Use of gloves (healthcare providers) during patient care
Drying of the washed hands is also important, and studies have shown that using dry paper towels works best at reducing microbes on the hands. Studies in 2008 have shown that using restroom air jet dryers actually increase microbes by >100% and can spread them to others up to 2 meters, or 6.6 feet, away!!! The same studies showed that warm-air hand dryers spread them up to 0.82 feet away, whereas paper towels showed no spread of microbes at all.
Studies have also shown, on the other hand, that when the skin gets too dried out, it can become cracked, leading to infection or colonization with microbes that can be spread, so special lotions should be offered to those who are susceptible, especially healthcare workers who may suffer from dermatitis or eczema and who are sensitive to alcohol-based hand rubs and to antimicrobial soaps.
Surgical scrubs are more in-depth and utilize sinks that can be turned on and off using a sensor or using one’s feet to prevent touching it with the hands, a chlorhexidine or iodine wash, sterile paper towels for drying afterwards, a sterile brush and nail pick for scrubbing and cleaning under the fingernails, plus all jewelry must be removed. This procedure includes washing one’s hands and forearms up to the elbow, for 2-6 minutes, or 10x per section (front of hand, back of hand, forearm, hind arm, upper arm, behind the upper arm). When rinsing, care must be taken to prevent water from running back onto the hands, and once it is completed, the hands are dried with a sterile paper towel and a surgical gown is donned. In other healthcare settings, antiseptic soap is used before and after tending to a sick person, and before and after changing one’s gloves.
The difference between regular soap and antibacterial soap is that washing with plain soap results in more than triple the rate of bacterial infectious disease transmitted to food as opposed to using antibacterial soap, which reduces Staphylococcus aureus.
Effective hand sanitizers should contain at least 60% alcohol solution as long as the hands are not visibly or excessively dirty or greasy or soiled, dirt is not present, and a spore-forming microbe is not suspected (Clostridium difficile, Bacillus cereus, Clostridium tetani, Clostridium perfringens), which is why they are not used in place of hand-washing in surgical settings and other healthcare settings, but can be used to supplement the hand-washing process afterwards. Studies have shown that this continues to reduce bacterial contamination by 26% after using antibacterial soap, but that soap and water reduces Influenza and noroviruses, as well as Clostridium difficile endospores from the hands. This should also be followed by moisturizing hand lotion to keep the hands from cracking or drying out, since dry skin can lead to damage, which can also increase the risk for transmission of infection. Good hand hygiene is essential to preventing the spread of infectious diseases everywhere and in every setting.
In the community setting, hand hygiene by hand washing with soap and water for at least 20 seconds followed by use of (not in place of) alcohol-based hand sanitizers, as well as using disinfectants, sanitizers, sterilizers and detergents to clean surfaces, are means we use to prevent the spread of viruses. This recommendation comes from the World Health Organization (WHO), before and after five critical times:
- After using the bathroom.
- After changing diapers.
- Before feeding a child.
- Before eating.
- Before and after preparing food or handling raw meat, poultry or fish.
- ***Also, wash your hands after sneezing, coughing, and more often when sick, after treating a cut or wound, blowing your nose, touching animal waste, handling animals, touching garbage, coming into contact with bodily fluids.
The CDC recommends following these steps and guidelines when washing one’s hands to prevent transmission of disease:
- Wet the hands first with warm or cold running water, since standing water might be contaminated.
- Lather up the hands by rubbing them with a generous amount of soap, including the palms, backs of the hands, the wrists, the thumb, between fingers, under the nails. Soap is a surfactant, lifting pathogens and grease and dirt from the skin, and water washes them down the drain.
- Scrub for at least 20 seconds. This creates mechanical friction, removing pathogens from the skin.
- Rinse thoroughly under running water.
- Dry the hands thoroughly with clean paper towels and allow them to air dry.
According to the CDC, when using hand sanitizer, enough of it should be used to thoroughly wet and cover both hands, front and back, between and at the ends of ALL fingers, and should be rubbed for approximately 30 seconds until it is dry. This goes for liquid, gel or foam applications. It should be noted that alcohol-based hand sanitizers are basically ineffective against the noroviruses (Norwalk viruses) that cause outbreaks of nausea, vomiting and diarrhea, and are the most common cause of contagious gastroenteritis. Hand sanitizers do not completely kill microbes, they just disinfect (reduce) them. They are not as effective as hand-washing with soap and water.
NOTE: Always read the fine print on the back of disinfectant and sanitizer cleaners because the time needed to sit on a surface varies and is different based on different microbial types. Many times, we simply spray and immediately wipe down a surface, but sometimes, a longer amount of time may be required.
Figure A (see below): A fingerprint without any handwashing or hand sanitizer; Figure B: A fingerprint after washing one’s hands with soap and water; Figure C: A fingerprint after using additional alcohol-based hand sanitizer, courtesy the Public Domain, https://upload.wikimedia.org/wikipedia/commons/thumb/8/8d/Hand_desinfection_test_with_blood_agar_plate.jpg/220px-Hand_desinfection_test_with_blood_agar_plate.jpg
Benefits of hand-hygiene include reducing the spread of viruses such as influenza A and B, COVID-19, RSV, the common cold, noroviruses, enteroviruses, and other infectious diseases and pathogens, such as MRSA. This reduces the spread of diarrhea, respiratory infections, vomiting and nausea due to viruses, reduces mortality rates, and reduces healthcare visits and costs related to them. Studies have proven that the simple action of washing one’s hands with soap and water can reduce mortality rates by 50% and can reduce diarrhea episodes by 48%. This is why it is promoted in the community, in schools, in homes, and in healthcare settings.
Children, elderly people, and those who are immunocompromised are at higher risk for developing infections. Pneumonia is the number one cause of mortality among children less than 5 years of age, followed by diarrhea, so making hand-washing a habit can help prevent disease and save lives.
When a person gets sick with a virus, they almost never get sick with the exact strain twice. Every time you get a cold or stomach virus or the flu, it is a different strain or sub strain. Viruses are constantly mutating and evolving, creating new strains that the immune system takes time to recognize. This is why you get symptoms and why it can take a while to completely recover. This is also why engineers work to create vaccinations/immunizations offered to trigger long-term memory and immune response, and antivenoms or antivirals to treat and lessen the severity of viral symptoms of infection. They may lessen the severity of the symptoms and amount of time an individual is ill.
It is important to note that antibiotics are ineffective against viruses. Antibiotics are designed only to kill bacteria, but viruses have a completely different structure. Prescribing antibiotics for viral infections leads to the bacteria becoming stronger and resistant to the antibiotics, which is why physicians try not to prescribe antibiotics for illnesses that are likely caused by viruses. The only true treatment for viral infections is rest, fluids, and over-the-counter relief medications for symptoms, and keeping a close watch if symptoms worsen. It is important to pay attention to symptoms during viral infections, since they can sometimes make a person more susceptible to a secondary bacterial infection, such as bacterial pneumonia.
PART B: Viral Infection Process:
What happens when a viral infection occurs? Viral replication happens in six steps:
- Attachment
- Entry
- Uncoating
- Replication
- Assembly
- Release/Budding
Attachment is the first phase during which a virus connects to your cell and an infection begins.
The entry stage involves a virus entering your cell’s cytoplasm. This is the point when the viral DNA or RNA gets inside your cell.
Uncoating is the step during which a virus loses its capsid. That’s the protein shell that protects viral DNA or RNA.
The replication stage is the point when the viral genome (DNA or RNA) replicates. It uses your cell’s ribosomes for protein synthesis.
Assembly occurs when the newly synthesized viral genome and viral proteins assemble to form a new virus.
Release is the last stage of viral replication when the new viruses are released in your organism. Viruses are released from host cells by budding. Enveloped viruses gain their envelope during this process by pinching off a piece of the host cell bilayer lipid membrane. Depending on a virus, sometimes the host cell dies during the release.
Bacteriophage Head-and-Tail Infections: Lytic Cycle and Latent Cycles: There are also viruses that can leave the host cell through the membrane and do not kill it. Either way, once out, the newly formed viruses may continue to spread and attack surrounding cells to replicate again, or they could stay dormant in your cells. An example of a virus that stays dormant in cells is the Varicella virus, which causes chicken pox. It can reactivate later as shingles. This is why a current vaccination series is available both for chicken pox (childhood series) and shingles (older adults).
PART C: Viral Infection in the Body: Signs and Symptoms:
Viruses are contagious for anywhere from a day to approximately a week before any symptoms appear, which is another reason why they spread so easily between people. This period of contagion is known as the incubation period, the period from the time of exposure to the virus until the first onset of symptoms, and it is different for every virus. Every virus lives for different amounts of time on surfaces and in the air, depending upon the virus. Some die very quickly, whereas others remain viable for hours or even days. During this period, the virus begins to replicate.
Examples:
· Influenza: 1-4 days
· Hepatitis B virus: 1.5-6 months
The next stage is the prodromal period, which is when the very first onset of symptoms occurs. This is typically that tired, run down feeling like you are coming down with something. This is when the virus is rapidly replicating in the host cells of the body. A low-grade fever may also begin at this point, as the virus “resets” the thermostat in the hypothalamus of the brain. The virus is contagious and can still be spread during this period. The body’s immune system is triggered, producing mild, nonspecific symptoms, including fatigue.
Example:
· Influenza: 2 days
This is followed by the period of illness, which differs from person-to-person and depends upon a number of factors, including the person’s underlying health, the virus type, and the viral load (how much virus is in the body). The fever may increase during this time, and symptoms are at their worst. The body’s immune response kicks in, which is the primary nonspecific response. The fatigue, brain fog, headache, pain, chills, swollen lymph nodes, and other symptoms of infectious disease are apparent.
Examples:
· Influenza or cold: about a week
· Hepatitis B: weeks to years (chronic if over 6 months)
· Herpes simplex virus or varicella virus: initially a week; can hide in a dormant state within nerve cells and reactivate later on.
Acute illness: comes on quickly and leaves quickly.
Chronic illness: may begin as acute, but lasts longer.
During the period of decline, the viral load and replication begins to decline. The viral antigen and antibodies produced by the immune system are typically able to be detected at this point for testing purposes. The immune system’s secondary, specific response (antibodies) are produced during this point, creating some long-term memory cells for a faster response the next time the individual encounters that same viral strain. The virus is still transmissible, however. Example: Influenza A, B (lasts about 7-10 days, but the person may still be transmitting it at this point)
During the convalescence period, the symptoms start to lessen and go away, and the individual begins to recover. This is also different from person-to-person and depends on the underlying health and the virus itself and the viral load. Depending upon the severity of infection, some people have permanent damage or effects, even after the infection resolves. Sometimes, the infection becomes chronic. Individuals are typically not contagious anymore at this point, and the fever is gone. Example: Influenza A, B (may still test positive at 2 weeks, but are no longer contagious)
Video on how the influenza virus infects the body: https://courses.lumenlearning.com/wm-biology2/chapter/steps-of-virus-infections/
Prevention:
While there are a number of things to prevent the spread of disease, the single best means of prevention is to wash your hands with soap and water. Scrub the front and back of your hands and wrists, in the creases, in between your fingers, under your fingernails, for at least 20 (preferably 30) seconds, or to the tune of “Happy Birthday”. If you are currently ill with a virus infection, the CDC recommends that you lengthen that time to 60 seconds.
Soap contains detergents and surfactants that bind to any microbes, oils and debris, lifting them up out of the creases, whereas water washes them down the sink. This is the best means of infection prevention. You should wash your hands before and after you eat, use the bathroom, prepare food, or if your hands are soiled. Also, if you work in healthcare, you should wash your hands before and after patient contact and after you remove your gloves.
Alcohol-based hand sanitizers are a great addition to use as a supplement along with washing your hands, but they should not be used in place of washing your hands with soap and water in the healthcare setting, because they do not kill endospore-forming bacteria. They do kill viruses, however.
Exercise 3: HANDS-ON GLOGERM EXPERIMENT:
Lab Objectives: The following exercises are designed to show you the following and upon completion of this exercise, you should be able to:
1) Explain how viruses spread and are transmitted, including how fomites (inanimate objects), and reservoir carriers (people) transmit them
2) Identify the prevalence of viruses and bacteria on surfaces and skin and other objects
3) Compare and contrast methods of hand hygiene for quality
a. Nothing
b. Water only
c. Hand sanitizer only
d. Soap and water – 30 seconds, 60 seconds
e. Paper towel only
4) Determine the best means of hand hygiene for prevention of the transmission of viruses
PART D: GloGerm Lab:
Watch These YouTube Videos to See What We Did in This Lab and What We Talked About:
https://youtu.be/I5-dI74zxPg
https://youtu.be/mJ3BE9sGm5w
Experimental Design:
One student volunteer will rub GloGerm lotion all over their hands really well. We will hold a UV light over the hands so you can observe an example of what happens when someone’s hands are contaminated with viral particles. Student one will shake hands with another student, who will shake hands with another student, etc…We will look at everyone’s hands with the UV light to see how the “virus” has spread. We will also look at surfaces to see if anything that was touched was “contaminated” with the “virus”. This is an example of the prevalence of microbes on hands and surfaces and what it theoretically resembles prior to washing one’s hands.
Another student volunteer will rinse their hands with water only, and we will observe again with UV light if water alone removed all of the “virus” particles.
A third student volunteer will rinse their hands with hand sanitizer only and we will observe with UV light if hand sanitizer alone was enough to remove all of the “virus” particles.
A fourth student volunteer will wash their hands with soap and water for the CDC’s recommended time, and we will observe with UV light if the soap and water method was effective enough to remove all of the “virus” particles. This simulation is a good example of the importance of hand washing for prevention of the spread of viruses.
A fifth student volunteer will wash their hands with soap and water for 30 seconds, followed by hand sanitizer. We will compare the five methods and see which one is most effective and which is least effective.
Worksheet 1: Critical Thinking Using Scientific Inquiry Every Time:
Observations and Questions: What observations did you make today based on these experiments?
What are the variables we changed for comparison? Did they make a difference?
Can you think of any other factors we could test for comparison?
Hypothesis or Hypotheses and Prediction(s):
Experiments/Tests: GloGerm Gel
GloGerm before rinsing, after 5 seconds with soap and water, after 20 seconds with soap and water, and after just hand sanitizer use. GloGerm after washing with soap and water for 30 seconds, but missing around the nails and knuckles and certain spots on the hands.
1. GloGerm lotion added/rubbed in under UV light
2. GloGerm after rinse and shake air drying
3. GloGerm after just water rinsing, no soap, no hand sanitizer
4. GloGerm after soap and water for < 30 seconds
5. GloGerm after soap and water rinsing for about 15 seconds
6. GloGerm after rinsing with soap and water for 30 seconds
Other: GloGerm after shaking hands with each other
Other: GloGerm after just paper towel usage
Hands after washing with soap and water for 30-60 seconds, scrubbing between fingers, under and around nails and nailbeds, knuckles, creases, palms, drying with paper towel, and followed up with hand sanitizer.
Data (Results/Information Gathered) and Analysis:
Use this area to draw a line graph or bar chart to compare and contrast the results of the experiments performed above. Copy down the big chart of class data we write on the board after this experiment.
Following GloGerm Application:
Variable: Type of Wash
Variable: Time of Wash
Results:
Which One Worked Best? Check (Recommendations)
GloGerm Application Only: No Rinse
N/A
Water Only and Paper Towel
20 seconds
Antibacterial Soap and Water and Paper Towel
15 seconds
Hand Sanitizer Only; No Paper Towel
30 seconds
Hand Sanitizer After Soap and Water and Paper Towel
15 seconds
Paper Towel Only
20 seconds
Soap and Water Rinse, Followed by Shaking Hands to Dry; No Paper Towel
20 seconds
Soap and Water, Paper Towel to Dry, Hand Sanitizer
30-60 seconds
Conclusion: What did you learn from this experiment and exercise today?
Worksheet 2: consider this worksheet for a lab report, INSERVICE, "LUNCH AND LEARN", or for ce's for infection control education:
Critical Thinking Questions: Refer to the Reading Sections in Parts A, B, and C to Answer the Following Questions:
What are some ways in which microbes are spread/transmitted?
What is the best means of prevention of the spread of disease produced by viruses and other infectious microbes?
What is the minimum amount of time one should scrub their hands according to the CDC?
Is it possible to be infected or colonized with a microbe without experiencing any symptoms?
Is it possible to transmit a microbe without experiencing any symptoms?
Define the following terms:
· Fomite:
· Vector:
· Carrier:
Why is it important to cover your mouth and nose when you sneeze?
Give examples of how microbes might be spread by the following means:
1) Direct contact:
2) Indirect contact:
3) Droplets:
4) Aerosols:
5) Foodborne/waterborne:
6) Vectorborne:
Why do you think it might be important to check the times on the backs of cleaners prior to wiping off a surface you have sprayed for cleaning?
Do ALL viruses leave the body once you’ve had an illness?
Are antibiotics effective against viruses? Why or why not?
Do alcohol-based hand sanitizers tend to kill most viruses and bacteria?
Which microbes do alcohol-based hand sanitizers not kill?
What bacterial structure do alcohol-based hand sanitizers not destroy? Example:
Why is it important to pay close attention to symptoms of viral infections?
What makes viruses and certain other microbes so contagious?
Can you spread a virus during the incubation period?
What is the prodromal period of viral infection?
Is the virus still contagious during the convalescent period?
What is the difference between acute and chronic illness?
Other observations and concepts learned during the reading portion:
Class Data Analysis: Virus Spread Questions Guide for the Board:
After the GloGerm lotion “virus” spread simulation in a class or group setting, record the following:
Initial person who shook hands: Index case (exchange 1)
Hypothesis:
Observations: How many individuals were “contaminated”? ___________________________________
Create a large table to show the + and – participants:
Participant:
Result: +/-
Exchange #1:
Exchange #2:
Exchange #3:
Data Analysis: What do the participant results show about the spread of disease?
Conclusion: Discuss how this experiment simulates real life transmission of microbes through a population and answer the following questions:
· What are some ways in which microbes are spread?
· What are some diseases that are spread through direct contact?
· What are some ways to prevent the spread of these diseases?
What are some ways in which microbes are spread/transmitted?
What is the best means of prevention of the spread of disease produced by viruses and other infectious microbes?
What is the minimum amount of time one should scrub their hands according to the CDC?
Is it possible to be infected or colonized with a microbe without experiencing any symptoms?
Is it possible to transmit a microbe without experiencing any symptoms?
Define the following terms:
· Fomite:
· Vector:
· Carrier:
Why is it important to cover your mouth and nose when you sneeze?
Give examples of how microbes might be spread by the following means:
1) Direct contact:
2) Indirect contact:
3) Droplets:
4) Aerosols:
5) Foodborne/waterborne:
6) Vectorborne:
Why do you think it might be important to check the times on the backs of cleaners prior to wiping off a surface you have sprayed for cleaning?
Do ALL viruses leave the body once you’ve had an illness?
Are antibiotics effective against viruses? Why or why not?
Do alcohol-based hand sanitizers tend to kill most viruses and bacteria?
Which microbes do alcohol-based hand sanitizers not kill?
What bacterial structure do alcohol-based hand sanitizers not destroy? Example:
Why is it important to pay close attention to symptoms of viral infections?
What makes viruses and certain other microbes so contagious?
Can you spread a virus during the incubation period?
What is the prodromal period of viral infection?
Is the virus still contagious during the convalescent period?
What is the difference between acute and chronic illness?
Other observations and concepts learned during the reading portion:
Class Data Analysis: Virus Spread Questions Guide for the Board:
After the GloGerm lotion “virus” spread simulation in a class or group setting, record the following:
Initial person who shook hands: Index case (exchange 1)
Hypothesis:
Observations: How many individuals were “contaminated”? ___________________________________
Create a large table to show the + and – participants:
Participant:
Result: +/-
Exchange #1:
Exchange #2:
Exchange #3:
Data Analysis: What do the participant results show about the spread of disease?
Conclusion: Discuss how this experiment simulates real life transmission of microbes through a population and answer the following questions:
· What are some ways in which microbes are spread?
· What are some diseases that are spread through direct contact?
· What are some ways to prevent the spread of these diseases?
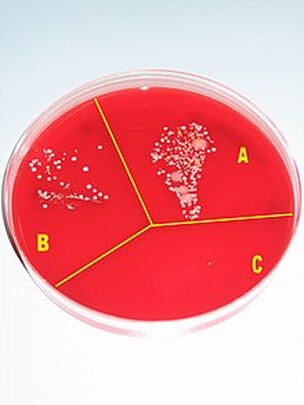
Microbial growth on a cultivation plate without procedures (A), after washing hands with soap (B) and after disinfection with alcohol (C); https://upload.wikimedia.org/wikipedia/commons/thumb/8/8d/Hand_desinfection_test_with_blood_agar_plate.jpg/220px-Hand_desinfection_test_with_blood_agar_plate.jpg
|
https://www.frostscience.org/wp-content/uploads/2020/04/glo-germ-blog-header.jpg
|
https://www.frostscience.org/wp-content/uploads/2020/04/hand-after-5-7-seconds-washing.jpg
|

https://www.frostscience.org/wp-content/uploads/2020/04/hand-after-20-seconds-washing.jpg
|
Hand Hygiene: handwashing
|
Now that you've seen the reasons why it is important to wash your hands, here is how the CDC recommends how to do it, and this came directly from their website:
"The Core Infection Prevention and Control Practices for Safe Care Delivery in All Healthcare Settings recommendations of the Healthcare Infection Control Practices Advisory Committee (HICPAC) include the following strong recommendations for hand hygiene in healthcare settings. Healthcare personnel should use an alcohol-based hand rub or wash with soap and water for the following clinical indications:
The 4 E's: "Clean and healthy hands count at every level of healthcare delivery. The Hand Hygiene in Healthcare Settings Video Series provides 4 short videos to help build a successful hand hygiene program. The video series describes foundations for engaging all healthcare personnel in hand hygiene, provides best practice techniques and practical tips for educating staff, exemplifies how to create an environment of accountability amongst personnel, and shows how to use data for action as a basis for continuous quality improvement. All 4 videos are appropriate for multiple audiences and can be used for training or education in healthcare settings." |
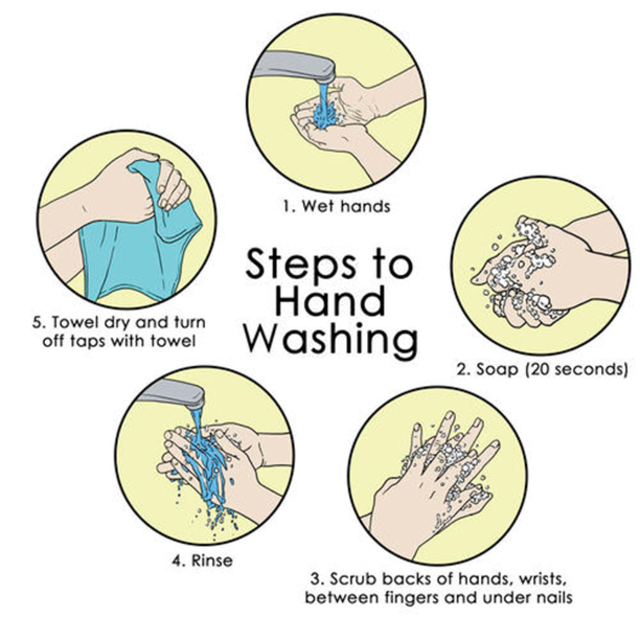
https://upload.wikimedia.org/wikipedia/commons/thumb/8/88/Steps_to_hand_washing.png/640px-Steps_to_hand_washing.png
|

https://upload.wikimedia.org/wikipedia/commons/thumb/1/1f/Steps_on_How_to_wash_your_hands_Steps_-_Infographic.png/640px-Steps_on_How_to_wash_your_hands_Steps_-_Infographic.png
|

https://upload.wikimedia.org/wikipedia/commons/thumb/c/c2/Prevention_of_spreading_of_covid-19_method.jpg/640px-Prevention_of_spreading_of_covid-19_method.jpg
|

https://upload.wikimedia.org/wikipedia/commons/thumb/6/6d/Water_and_soap_one_of_the_used_in_Rwanda_in_prevention_of_spreading_og_covid-19.jpg/640px-Water_and_soap_one_of_the_used_in_Rwanda_in_prevention_of_spreading_og_covid-19.jpg
|

https://upload.wikimedia.org/wikipedia/commons/thumb/1/12/Washing_hand_with_soap_in_prevention_of_covid-19.jpg/640px-Washing_hand_with_soap_in_prevention_of_covid-19.jpg
Great videos from the cdc on the 4 e's of hand hygiene for healthcare professionals:
|
|
|
|
|
|
Artificial nails:
While artificial nails are so beautiful, as seen in the two images below, those who provide direct patient care should not wear artificial nails in this type of setting while they are providing direct patient care. This includes gel, silicone, shellac, acrylic, silk wraps, overlays, linens, fiberglass, extensions, or nail enhancements.
Did you know that Hepatitis A outbreaks have been linked to artificial nails? Bacteria, viruses, fungi and even parasites can become trapped and lodged underneath the shellac or the artificial nail, which can be transmitted to a susceptible patient. They can also poke holes in gloves easier, creating an open door through which viruses and bacteria can exit through that broken barrier.
Did you know that Hepatitis A outbreaks have been linked to artificial nails? Bacteria, viruses, fungi and even parasites can become trapped and lodged underneath the shellac or the artificial nail, which can be transmitted to a susceptible patient. They can also poke holes in gloves easier, creating an open door through which viruses and bacteria can exit through that broken barrier.

https://upload.wikimedia.org/wikipedia/commons/thumb/d/d5/Dr._Sandra_Palmer.jpg/640px-Dr._Sandra_Palmer.jpg
|

https://upload.wikimedia.org/wikipedia/commons/thumb/d/df/%D0%9F%D1%80%D0%BE%D1%84%D0%B5%D1%81%D0%B8%D0%BE%D0%BD%D0%B0%D0%BB%D0%BD%D0%B0_%D0%9D%D0%BE%D0%BA%D1%82%D0%BE%D0%BF%D0%BB%D0%B0%D1%81%D1%82%D0%B8%D0%BA%D0%B0.JPG/1280px-%D0%9F%D1%80%D0%BE%D1%84%D0%B5%D1%81%D0%B8%D0%BE%D0%BD%D0%B0%D0%BB%D0%BD%D0%B0_%D0%9D%D0%BE%D0%BA%D1%82%D0%BE%D0%BF%D0%BB%D0%B0%D1%81%D1%82%D0%B8%D0%BA%D0%B0.JPG
|
references:
1. The Centers for Disease Control and Prevention (CDC), https://www.cdc.gov
2. Lumen Learning
3. Glo Germ: Handwashing Training, https://www.glogerm.com/handwashing.html
4. Jeanette (Jen) Reynolds, MS-Biology, M-ASCP, MLS-AMT, Certified in Emerging Diseases, Certified Instructor, Certified EKG Tech, Infection Preventionist
2. Lumen Learning
3. Glo Germ: Handwashing Training, https://www.glogerm.com/handwashing.html
4. Jeanette (Jen) Reynolds, MS-Biology, M-ASCP, MLS-AMT, Certified in Emerging Diseases, Certified Instructor, Certified EKG Tech, Infection Preventionist

{kind=link}